Keywords
Pancreatic neoplasms; Pancreas cancer; Radiosurgery; Stereotactic; Stereotactic body radiation therapy (SBRT); Radiation; Radiotherapy
Introduction
In the year 2020, about 57,600 people will be diagnosed
with pancreatic cancer and approximately 47,050 people
will die of this devastating disease. Over the last several
decades, the survival rates among patients with pancreatic
cancer remain dismal [1]. The overall 5-year relative
survival rate for patients reported to the Surveillance,
Epidemiology, and End Results (SEER) database of the
National Cancer Institute from 1996 to 2004 was 5.1% [2].
Treatment strategies for early respectable and metastatic
disease are relatively clear and definite, namely resection
plus sequential adjuvant chemotherapy for the former and
systemic chemotherapy or supportive care for the latter
[3]. The role of radiation therapy in pancreatic cancer
continues to be investigated. Randomized trials have
yielded conflicting data in locally advanced disease. Also,
as radiation techniques have improved over time, findings in older trials may not be applicable in modern practice
[4]. Treatment for pancreatic cancer has been the subject
of debate [5]. Despite, and often because of, the results of
multiple contradictory clinical trials that have examined
various management strategies, the optimal manner in
which pancreatic cancer should be treated ultimately
rests in the judgment and preferences of the individual
oncologist [6]. At the center of much of this controversy
is radiation therapy. Therefore, to further investigate the
relationship between adjuvant radiation therapy and
pancreatic cancer patient prognosis, we used data from
the Surveillance, Epidemiology, and End Result (SEER)
database to explore the impact of adjuvant radiation on
cancer-specific survival in pancreatic cancer patients who
received surgical resection.
METHODS
Study Population
A retrospective cohort was identified using the
Surveillance, Epidemiology and End Results (SEER)
database, a project sponsored by the National Cancer
Institute [7,8] The SEER database was established in 1973
and is a set of extensive population-based cancer registries
that cover approximately 28% of the US population
(Alaska Native Tumor Registry, Connecticut, Georgia
Center for Cancer Statistics, San Francisco-Oakland, San
Jose-Monterey, Greater California, Hawaii, Idaho, Iowa, Kentucky, Los Angeles, Louisiana, Massachusetts, New
Mexico, New York, Seattle- Puget Sound, Utah). We queried
the November 2018 submission from 1973 to 2015. Using
the International Classification of Disease, Third Edition
(ICD-O-3) codes, we queried for Primary site "Pancreas".
Inclusion criteria were set as adenocarcinomas of the
exocrine pancreas. Since data in the SEER database is deidentified,
our study is exempt from Institutional Review
Board review.
Selection of variables
Variables of interest included the year of diagnosis,
patient demographics (age at diagnosis, gender, race, and
marital status), tumor characteristics (stage, grade, and
tumor size), surgery technique and details, radiotherapy
or chemotherapy administered, as well as survival in
months and patient status at the end of follow up period.
The race was recorded as white, black, Spanish-Hispanic-
Latino, Asian, and others.
Survival was defined as months from the time of diagnosis
to the point of last contact or the date of death in cases where
the patient was deceased. Patient status at the end of the
follow-up period was recorded as alive or deceased.
Statistical analysis
Data extracted from the SEER database was imported
on to the statistical package for the social sciences (SPSS)
version 23 IBM Corp, USA for analysis [8]. Both descriptive
and inferential analysis was conducted. Characteristics of
our sample population were described using frequencies,
percentages, means, and medians. Survival was estimated
using the Kaplan–Meier curve. Survival differences
between variables were compared using the log-rank test.
We subsequently computed propensity scores to assess
the probability of being assigned to a treatment group
(surgery only or surgery plus adjuvant radiation) based
on the observed patient's demographic, and pretreatment
clinical characteristics. The logistic regression model was
used to calculate the propensity scores derived from these
confounding preoperative parameters. These variables
included age, sex, race, year of diagnosis, marital status,
and preoperative tumor characteristics (size, grade, tumor
location). The most appropriately matched pairs were
selected based on the propensity scores using a 1:1 nearest
neighbor algorithm (R-plugin 2.14.2 for SPSS vs. 21.0).
A p-value of less than 0.05 was considered significant.
Confidence intervals (CI) were set at 95%. Multivariate
Cox-regression was used to study the relationship between
various patient and disease-specific factors and survival.
RESULTS
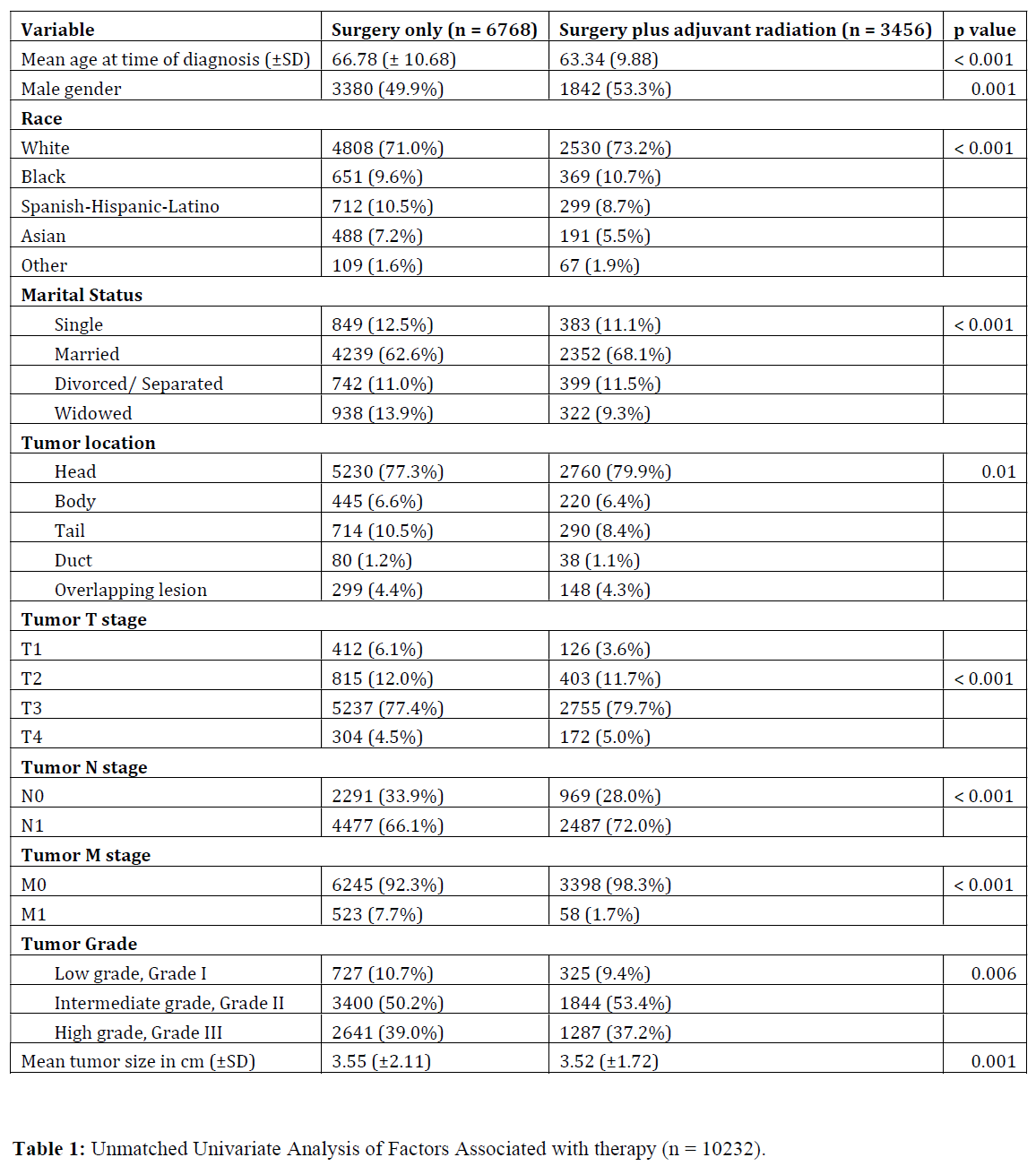
A total of 10,224 patients met our inclusion criteria
with 6768 (66.2%) patients treated with surgery only
and 3456 (33.8%) treated with surgery plus adjuvant
radiation. Table 1 compares the baseline characteristics
of the two groups. Significant differences between
patient demographics and tumor characteristics were
demonstrated.
Unmatched survival analysis
Patients who underwent surgery plus adjuvant
radiation had a significantly higher overall survival (OS)
than patients who underwent surgery only (p <0.001). The
median OS values were 21 and 16 months for surgery plus
adjuvant radiation and surgery only respectively.
Propensity Score Matching and Multi-variate Survival
Analysis
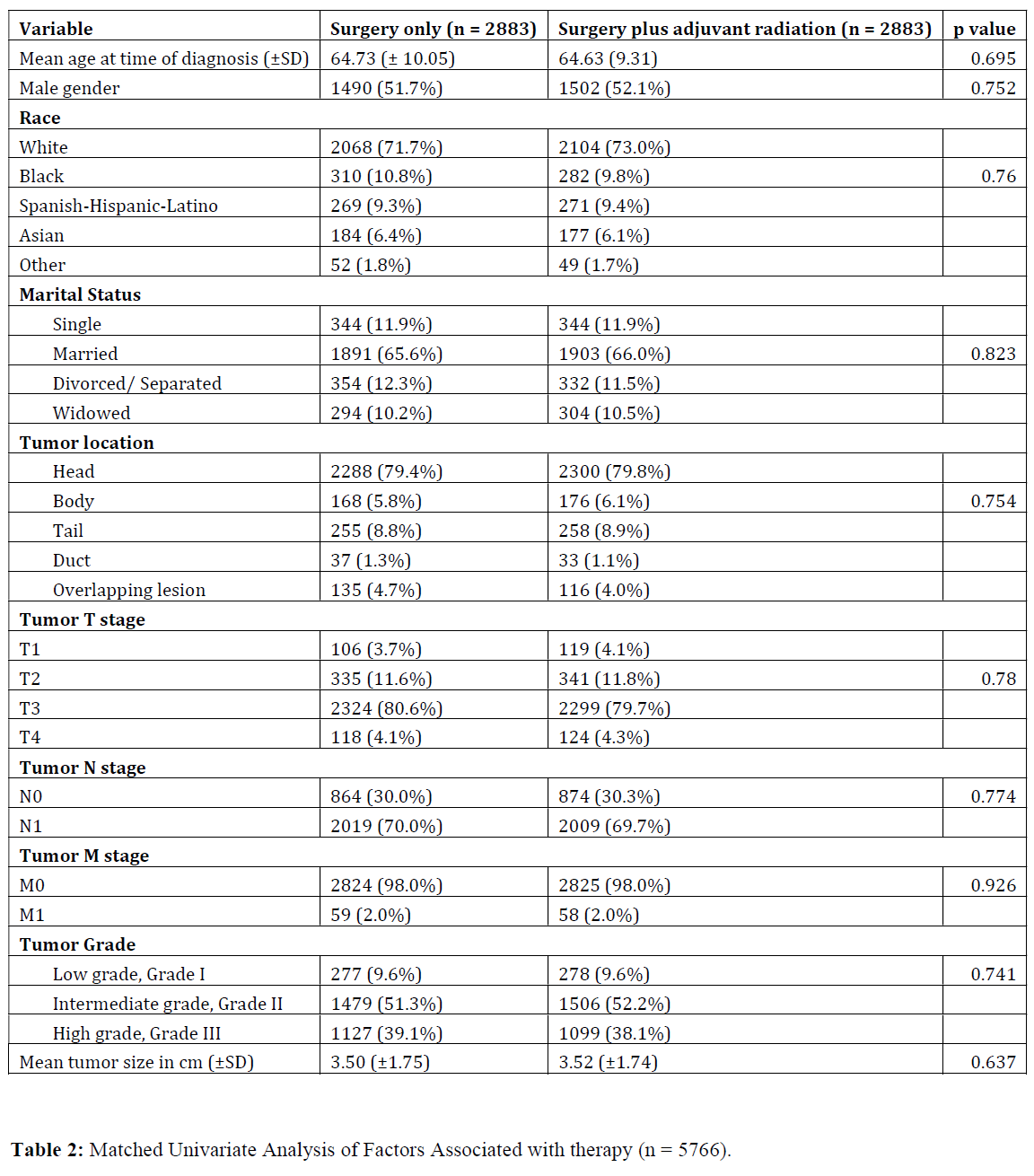
Propensity matching yielded 5766 patients (2883
matched pairs) from surgery plus adjuvant radiation and
surgery only groups. There were no significant differences
in baseline characteristics between the two groups after
matching (Table 2).
Patients following surgery plus adjuvant radiation
had significantly higher OS when compared to patients
undergoing surgery only (p < 0.001). The median OS
values were 21 and 16 months for surgery plus adjuvant
radiation and surgery only respectively.
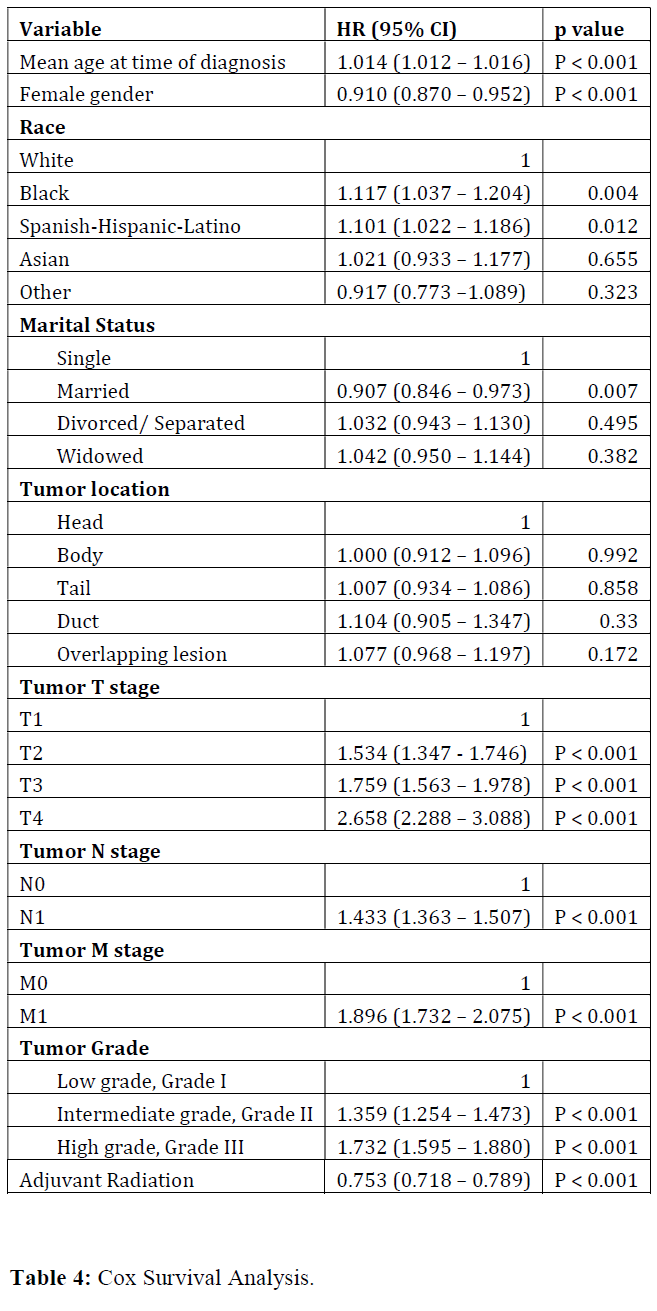
We further investigated the correlation between OS and
other covariates in a Cox Regression Analysis. Multivariate
analysis demonstrated that surgery plus adjuvant radiation
was associated with significantly improved survival (HR:
0.753, CI: 0.718 – 0.789, p < 0.001). Additionally, female
gender and married status were associated with better
survival (p < 0.05) while advanced age, Caucasian race,
higher TNM stage, and higher grade had worse survival
outcomes (p < 0.05) (Table 3).

Predictors of adjuvant radiation
In a logistic regression model evaluating factors
associated with receipt of adjuvant radiation (Table
4), older age, prior or current marital status, and higher
T and N stages were associated with receipt of adjuvant
radiation. Spanish-Hispanic-Latino and Asian races and
higher M stages were associated with adjuvant radiation
not being administered.
DISCUSSION
Our study showed a survival benefit in patients who
received adjuvant radiation therapy for pancreatic cancer.
This study adds to the growing literature of retrospective
studies on the role of radiation therapy following
pancreatic resection and highlights the need for a large
multicenter randomized trial.
Radiation therapy represents a highly complex and
technical treatment that is rapidly evolving. The modality
has undergone and continues to undergo, dramatic
transformations with advances in computational modeling
and medical imaging [9,10]. These advances will only
continue to accelerate in the coming years and will likely
follow a "double exponential" growth pattern leveraging
advances in both hardware and software capabilities.
While radiation therapy has historically been described as
a singular entity in oncologic management it represents a
broad treatment class, inclusive of a wide range of treatment
procedures and methods. Despite the spectrum of potential
treatments under the category of radiation therapy, the allencompassing
nomenclature may obscure the heterogeneity
that exists within the term radiation therapy.11
The GITSG trial randomized patients with pancreatic
adenocarcinoma resected to negative margins to 40 Gy
delivered with 2 Gy daily fractions with a split course
(2-week break after the first 20 Gy were delivered) with
concurrent 5-FU chemotherapy versus observation alone
[11]. Five-year OS was 15% vs. 5% and median diseasefree
survival (DFS) was 11 vs. 9 months, both favoring the
adjuvant chemoradiotherapy arm. The trial was closed
early due to poor accrual. However, this trial helped
establish adjuvant chemoradiotherapy (CRT) as the
standard of care in the United States.
Our results are in concordance with prior studies of
adjuvant radiation therapy for pancreatic cancer. Cox
analysis conducted by Blain et al. found that receiving EBRT
was an independent prognostic factor for an improved hazard ratio of dying from pancreatic cancer (HR=0.65,
p<0.0001) [12]. Sugawara and Kunieda analyzed 2,532
patients from the SEER database treated with surgery
plus/minus adjuvant radiotherapy from 2004 to 2009 [13].
They also found a survival advantage in the radiotherapy
group. Overall survival (OS) was 20 months vs. 16 months
in the adjuvant radiotherapy and observation groups,
respectively (p<0.0001). Disease-specific survival was
22 months vs. 18 months in the adjuvant radiotherapy
and observation arms, respectively. Opfermann et al.
analyzed 3,314 patients from the SEER database treated
with surgery plus/minus adjuvant radiotherapy from
1998 to 2006 [14]. They also found a survival advantage in
the radiotherapy group. OS was 19 months vs. 14 months
favoring the radiotherapy arm (p<0.001). The expanded
timeframe of our study is promising for the continued use of
this adjuvant therapy. Moreover, we found that the type of
surgery performed, and the location of the tumor does not
influence the benefit of adjuvant radiation. Alternatively, the
relatively short lifespan of these patients could mean that
survival differences are potentially attributable to the type
of surgery performed and the location of the tumor, both of
which do not appear within the available follow-up period.
Concerning trends regarding potential disparities in the
utilization of radiation therapy emerged from our analysis.
Namely, those white patients were more likely to receive
adjuvant radiation than Asian and Spanish-Hispanic-
Latino patients. Shavers et al similarly found that Hispanic
patients were less likely to receive radiation therapy for
pancreatic cancer than non-Hispanic whites (OR 0.50, 95%
CI, 0.27–0.95) [15] Gad et al found an increasing trend of
pancreatic adenocarcinoma incidence-based mortality
among Asian-American patients, with an annual increase
of 4.535% (95%CI 3.538-5.541; P<0.001) from 1992 to
2015 [16]. Their SEER analysis did not include trends in
radiation therapy. In concordance with our data, Eloubeidi
et al. identified no difference in radiation therapy by
race when comparing black and white patients (15.0% vs. 14.2% for white's vs. blacks, P=.65) on analysis of the
Alabama Statewide Cancer Registry from 1996 to 2000,
however, they did identify that black patients were less
likely to receive both chemotherapy (26.78% vs. 32.3%,
P=.02) and surgery (14.0% vs. 17.0% P=.09), which has
also been found on SEER analysis [17].
Healthcare inequities in the incidence and mortality
of pancreatic cancer are multifaceted. Given the survival
advantage identified among patients who receive surgery
and adjuvant radiotherapy, ensuring access to such
treatment modalities is an important step in improving
pancreatic cancer outcomes. Noel and Fiscella identified
that black and Hispanic patients with pancreatic cancer
had lower rates of surgical resection and were more likely
to be treated at low-volume hospitals, proposing that
differences in pancreatic cancer outcomes are driven by
race and socioeconomic status [18]. Continued analysis
of differential utilization of radiation therapy, both on
a population and individual patient level, is needed to
determine steps towards more equitable treatment.
It is important to note some important disadvantages
of using the SEER database. This database does not report
chemotherapy data and does not report the dose or duration
of radiotherapy. Also, margin status was not available in the
SEER database for this group of patients [19-22]. However,
previous meta-analyses conducted have suggested that the
benefit of adjuvant radiotherapy may be limited to patients
with positive margins, so perhaps these patients were
more likely to have gotten this adjuvant treatment in
the SEER database and thus would be over-represented
in the irradiation arm. Therefore, incorporating more
information on chemotherapy, radiotherapy, and margin
status would be useful in investigating the effects of these
factors on survival in pancreatic cancer patients. Data from
randomized clinical trials may also aid in the investigation
of the impact of various treatment approaches.
References
- Hall WA, Goodman KA. Radiation therapy for pancreatic adenocarcinoma, a treatment option that must be considered in the management of a devastating malignancy. Radiat Oncol 2019; 14: 114.
- Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med 2014; 371: 1039-49. [PMID: 25207767].
- Bockhorn M, Uzunoglu FG, Adham M, Imrie C, Milicevic M, Sandberg AA, et al. Borderline resectable pancreatic cancer: A consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2014; 155: 977-988. [PMID: 24856119].
- Tepper J, Nardi G, Sutt H. Carcinoma of the pancreas: review of MGH experience from 1963 to 1973. Analysis of surgical failure and implications for radiation therapy. Cancer 1976; 37: 1519-1524. [PMID: 1260670].
- Gudjonsson B. Cancer of the pancreas. 50 years of surgery. Cancer 1987; 60: 2284-2303. [PMID: 3326653].
- Griffin JF, Smalley SR, Jewell W, Paradelo JC, Reymond RD, Hassanein RE, et al. Patterns of failure after curative resection of pancreatic carcinoma. Cancer 1990; 66: 56-61. [PMID: 2354408].
- Whittington R, Bryer MP, Haller DG, Solin LJ, Rosato EF. Adjuvant therapy of resected adenocarcinoma of the pancreas. Int J Radiat Oncol Biol Phys 1991; 21: 1137-43. [PMID: 1938511].
- Baig MZ, Razi SS, Weber JF, Connery CP, Bhora FY. Lobectomy is superior to segmentectomy for peripheral high grade non-small cell lung cancer ≤2 cm. J Thorac Dis 2020; 12: 5925-5933. PMID: 33209425.
- Iacobuzio-Donahue CA, Fu B, Yachida S, Luo M, Abe H, Henderson CM, et al. DPC4 gene status of the primary carcinoma correlates with patterns of failure in patients with pancreatic cancer. J Clin Oncol 2009; 27: 1806-1813. [PMID: 19273710].
- Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 1985; 120: 899-903. [PMID: 4015380].
- No authors listed. Further evidence of effective adjuvant combined radiation and chemotherapy following curative resection of pancreatic cancer. Gastrointestinal Tumor Study Group Cancer 1987; 59: 2006-2010. [PMID: 3567862]
- Baine MJ, Lin C. Radiation therapy improves survival outcome in pancreatic adenocarcinoma: comparison of a 15-year institution experience at the University of Nebraska Medical Center with SEER data. J Radiother 2014.
- Sugawara A, Kunieda E. Effect of adjuvant radiotherapy on survival in resected pancreatic cancer: A propensity score surveillance, epidemiology, and end results database analysis. J Surg Oncol 2014; 110: 960-966. [PMID: 25146251]
- Opfermann KJ, Wahlquist AE, Garrett-Mayer E, Shridhar R, Cannick L, Marshall DT. Adjuvant radiotherapy and lymph node status for pancreatic cancer: Results of a study from the Surveillance, Epidemiology,and End Results (SEER) Registry Data. Am J Clin Oncol 2014; 37:112-116. [PMID: 23211221]
- Shavers VL, Harlan LC, Jackson M, Robinson J. Racial/ethnic patterns of care for pancreatic cancer. J Palliat Med 2009; 12: 623-630. [PMID: 19594347].
- Gad MM, Găman MA, Saad AM, Al-Husseini MJ, Shehata OA, Abou Saleh M, et al. Temporal trends of incidence and mortality in Asian-Americans with pancreatic adenocarcinoma: An epidemiological study. Ann Gastroenterol 2020; 33: 210-218. [PMID: 32127743].
- Eloubeidi MA, Desmond RA, Wilcox CM, Wilson RJ, Manchikalapati P, Fouad MM, Eltoum I, Vickers SM. Prognostic factors for survival in pancreatic cancer: A population-based study. Am J Surg 2006; 192: 322-329. [PMID: 16920426].
- Noel M, Fiscella K. Disparities in pancreatic cancer treatment and outcomes. Health Equity 2019; 3: 532-540. [PMID: 31663065].
- Aziz H, Genyk Y, Saif MW, Filkins A, Selby R, Sheikh MR. Review of oncology and transplant literature for the management of hepatic and pancreatic resections in Jehovah's Witnesses. Cancer Med J 2021; 4: 16-26. PMID: 32601622. [PMID: 32601622].
- Aziz H, Zeeshan M, Kaur N, Emamaullee J, Ahearn A, Kulkarni S, et al. A potential role for robotic cholecystectomy in patients with advanced liver disease: Analysis of the NSQIP Database. Am Surg 2020; 86: 341-345. PMID: 32391758. [PMID: 32391758].
- Aziz H, Hanna K, Saif MW, Rauf MA, Genyk Y, Sheikh MR. Hepatectomy for breast cancer metastasis and sarcoma are more likely to have adverse outcomes than hepatectomy for primary hepatocellular cancer or for colorectal metastasis. Cancer Med J 2020; 3:6-12. PMID: 33196059.
- Aziz H, Zeeshan M, Jie T, Maegawa FB. neoadjuvant chemoradiation therapy is associated with adverse outcomes in patients undergoing pancreaticoduodenectomy for pancreatic cancer. Am Surg 2019; 85: 1276-1280. [PMID: 31775971].

