Keywords
Melanoma; Neoplasm Metastasis; Pancreas;
Pancreatectomy
Abbreviations
BL biochemical leak; CT computed tomography;
CTLA-4 cytotoxic T lymphocyte antigen 4; DP distal pancreatectomy;
F female; FDG fluorodeoxyglucose; FDA food and drug
administration; IL interleukins; LDH lactate dehydrogenase; Lap
laparoscopic; M male; MM malignant melanoma; NK not known; PD
pancreaticoduodenectomy; PD-1 programmed cell death protein 1;
PPPD pylorus-preserving pancreaticoduodenectomy; S splenectomy;
TP total pancreatectomy
INTRODUCTION
Malignant Melanoma (MM) is the 6th most common
cause of cancer in Western Europe (5th in the United States)
and the 16th most common cause of cancer-related death in
both Western Europe and the United States [1].
Solitary MM metastasis to the pancreas is rare and
occurs in approximately 1% of patients with metastatic
melanoma [2]. Historically most of these patients were deemed not suitable for resection. However, resection of
isolated pancreatic metastasis could allow disease-free
survival benefit, particularly in the absence of effective
systemic therapies. We present a case of pancreatic
resection for isolated malignant melanoma metastasis
along with a review of the related literature.
MATERIALS AND METHODS
The authors systematically reviewed the published
literature up to January 2019 using PubMed and following
the PRISMA guidelines [3]. The search was performed under
the following Medical Subject Headings (MeSH) terms:
melanoma, metastases, pancreas, and pancreatectomy.
All the literature published in the English language was
reviewed and the references were cross-checked for
additional studies. Most were case reports. Patients with
extra-pancreatic disease (diagnosed and treated before
or at the time of diagnosis of pancreatic metastases) and
patients who did not undergo surgery were excluded. The
following data were obtained from each study: authors,
year of publication, number of patients, age and gender,
primary site, interval between primary and metastases,
tumour size, surgery performed follow-up, outcome and
recurrence.
RESULTS
A forty-six-year-old, Caucasian, female patient with
previous history of right arm MM was referred to our Unit
after a pancreatic mass was detected in her routine follow-up
with thoracoabdominopelvic Computed Tomography (CT).
In 2007 she had underwent excision of a MM from
the right arm staged as a pT1b, Breslow thickness of 0.5
mm, with no lymphovascular or perineural invasion, or
micro satellite lesions identified; mitotic rate was 1 per 10
HPF.
In 2015, she presented with right side axilla
lymphadenopathy for which she underwent unilateral
axillary dissection. The pathology report revealed a
deposit of metastatic malignant melanoma, 67 mm, likely
representing a replaced lymph node. Extra-capsular
extension was not identified. Immuno-phenotyping was
consistent with metastatic MM (S100+; melanin A-). A
further 12 nodes sampled were negative for tumour. She
received adjuvant treatment with interferon alpha-2b.
In 2016, on a follow up CT scan, a new isolated
hypodense lesion in the tail of the pancreas measuring 1.7
cm was identified (Figure 1).
Figure 1: CT scan with a new isolated hypodense lesion in the tail of the pancreas measuring 1.7 cm.
A 18F-flurodeoxyglucose (FDG) positron emission
tomography revealed a 2 cm focus of markedly increased
FDG uptake in the tail of the pancreas, consistent with
a solitary metastasis, with no other hypermetabolic
suspicious areas identified (Figure 2).
Figure 2: PET-scan with a 2 cm focus of markedly increased FDG uptake in the tail of the pancreas.
The patient was referred to our Unit at this time and
in a multidisciplinary meeting the decision was made to
proceed with a laparoscopic distal pancreatectomy and
splenectomy. The patient did not have any other medical
history, medication or allergies. She also had a recent brain
CT and oesophagogastroduodenoscopy, both of which
were normal.
She underwent a laparoscopic distal pancreatectomy
and splenectomy in February 2017. She made an uneventful recovery and was discharged home four days
after the surgery with a surgical abdominal drain in situ,
due to a Biochemical Leak (BL) pancreatic fistula [4]. She
was reviewed in our out-patient clinic one week after
discharge and the drain was removed.
Pathology report revealed a deposit of metastatic
tumour in the pancreas consistent with metastatic
malignant melanoma, 28 mm maximum dimension.
Lymphovascular invasion was present. Two lymph nodes
out of 21 were positive for metastatic melanoma. The
resection margins were negative. The spleen was normal
(Figure 3).
Figure 3: (a). Macroscopic image of tumour cut surface of resected specimen. (b). Histopathological appearance of resected tumour; (b1). Hematoxylin and
eosin staining with tumour predominantly on the left with occasional residual pancreatic tissue and non-involved pancreas on the right (10x lens); (b2). Hematoxylin and eosin staining demonstrating a high mitotic rate (20x lens); (b3). Positive immunohistochemical staining of S-100 protein (10x lens).
The patient is currently well with no signs of recurrence
two years after the resection and is undergoing followup
at her local hospital. She did not receive any adjuvant
treatment.
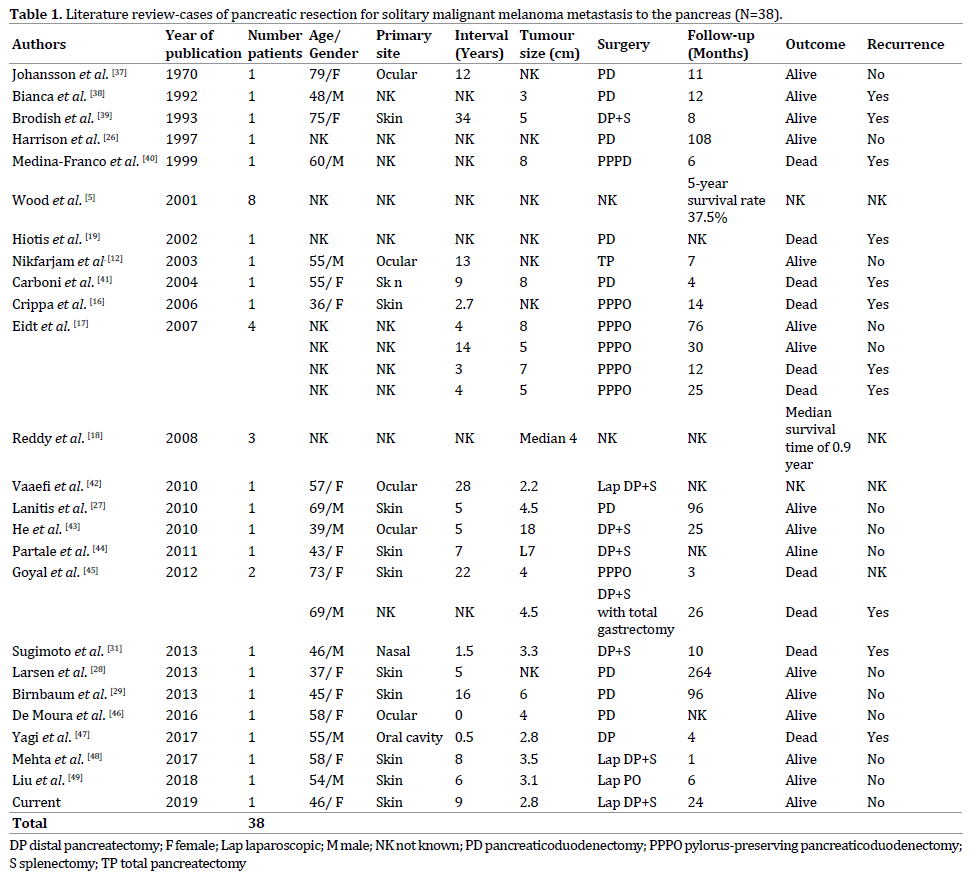
The literature search revealed three case series (more
than two patients) and 22 single case reports, for a total of
38 patients with isolated MM metastases to the pancreas
(Table 1). Among these patients, 11 had a primary skin MM,
five had ocular MM, one had nasal cavity MM, another had oral
cavity MM and in 20 the primary site was not reported. The
interval between the primary diagnosis and development
of metastases ranged from 0-408 months. The surgeries
performed were: nine pancreaticoduodenectomies;
seven pylorus-preserving pancreaticoduodenectomies;
one laparoscopic pancreaticoduodenectomy; one open
distal pancreatectomy; four open distal pancreatectomies
with splenectomy; one open distal pancreatectomy,
splenectomy and total gastrectomy; three laparoscopic
distal pancreatectomies with splenectomy; one total
pancreatectomy and in eleven cases the surgical procedure
performed was not reported. A five-year survival rate of
37.5% was reported in one of the case series [5]. Recurrent
disease was observed in 11 patients, 14 had no recurrence
and 13 had no information regarding recurrent disease.
Sixteen patients were alive, 10 patients had died and in 12
patients no information was available.
DISCUSSION
Malignant Melanoma is the 6th most common cause of
cancer in Western Europe (5th in the United States) and the
16th most common cause of cancer-related death in both
Western Europe and the United States [1]. According to the SEER program the incidence of MM has dramatically
increased (7.89/100000 in 1975 – 25.23/100000 in 2017)
[6] and in 2017 it is estimated that there will be 87,110
new cases of cutaneous melanoma and 9,730 people will
die of this disease [7]. MM is the most rapidly increasing malignancy in men, and the 2nd most common cancer in
women, surpassed only by lung cancer. The median age at
diagnosis is 59 years and the lifetime risk of developing
MM is 1 in 53 for men and 1 in 34 for women. Overall, a
patient loses 20.4 years of potential life as a result of MM
mortality compared to 16.6 for all malignancies [8].
Risk factors include male sex, age above 60, phenotypic
predisposition, previous personal or family history of MM,
use of immunosuppression and environmental factors [8].
The outcomes of MM depend, as with other
malignancies, on the stage at presentation according
to the TNM classification [8]. In the United States, it is
estimated that 84% of patients will present with localized
disease, 9% with regional disease, and 4% with metastatic
disease [8]. Patients with stage IV disease can be further
subdivided into those with only cutaneous metastases
(IVa), lung metastases (IVb), or other visceral metastases
(IVc) with associated 5-year survival rates of 18.8%, 6.7%,
and 9.5%, respectively [9]. MM frequently metastasizes
to the Gastrointestinal (GI) tract, with studies showing GI
tract involvement in 50% to 60% of patients with MM at
autopsies. However, a clinical diagnosis of GI involvement
is only made in 1.5% to 4.4% [10]. Although these patients
continue to have a poor prognosis, with a mean survival
of 8–10 months [9], long-term survival after complete
resection for GI tract metastases is reported [5, 11].
Metastatic tumours to the pancreas represent about
2% of all pancreatic malignancies [12, 13, 14]. According
to a review of 418 patients with secondary tumours of the
pancreas, the site of origin was renal cell carcinoma (70%),
followed by MM (9.1%), colorectal cancer (8.9%), breast
cancer (4.5%), sarcoma (4.3%), and lung cancer (3.1%)
[12]. In another review of 243 patients with resected
metastatic pancreatic tumours, the site of origin was renal
cell cancer (61.7%), colorectal cancer (7.8%), melanoma
(4.9%), sarcoma (4.9%), lung cancer (3.3%), gastric cancer
(3.3%), gallbladder cancer (3.3%), and breast cancer
(2.5%) [15].
Solitary MM metastasis to the pancreas is rare and
occurs in approximately 1% of patients with metastatic
melanoma [2]. Historically, most of these patients were
offered either systemic or palliative treatment and were
deemed unsuitable for resection. This was partly due to the
fact that the 5-year survival was less than 10% and there
was considerable morbidity and mortality associated with
pancreatic surgery [2, 16, 17]. On the other hand, with the
combined evolution of imaging techniques and surgical
expertise, these resections have been effectively and
safely performed with improvements in survival [16, 17, 18, 19]. Fletcher et al. achieved a 5-year survival of 18%,
with a median survival of 15 months, following complete
resection of solitary pancreatic metastases from MM [20].
Still, the role of resection in the management of isolated
metastatic MM involving the pancreas is not well defined
[18, 21].
Another factor to be taken into consideration is
systemic therapies for melanoma. They have evolved slowly since the approval of dacarbazine by the U.S. Food
and Drug Administration (FDA) in the seventies. Highdose
interferon alpha-2b was sanctioned in the nineties
for the adjuvant treatment of patients with MM. During
that period, Fletcher et al. stated that surgical resection
provides 5-year survival rates superior to any available
nonsurgical therapy [20]. Since then, many other therapies
have been or are being developed, namely, BRAF inhibitors,
systemic and intralesional IL-2, Imiquimod/toll-like
receptor activation, Bacillus Calmette-Guérin, interferon
therapy, cancer vaccines, oncolytic vaccines, and adoptive
cell therapy. More recently, the newer biologic agents,
such as anti-CTLA4 therapy and anti-PD-1 have made an
enormous impact on melanoma therapy [22].
Despite all the extensive research and drug
development in the field of MM treatment, Duetsch et al.
in a large study published in 2017 including 1623 patients
with abdominal MM metastases, demonstrated that
patients treated with surgical resection had better overall
survival and that systemic treatment with newer agents
did not have a significant effect on survival [23]. Several
other authors have also found that long-term survival
can be achieved when complete resection of pancreatic
metastases is undertaken, typically in patients with renal
cell cancer but also in patients with other primaries [11, 18, 19, 21, 24, 25]. Furthermore, some case reports, of
patients undergoing pancreatic resection for isolated
metastases from MM, support the idea that this approach
improves overall survival [5, 26, 27, 28, 29]. One must also
consider the benefits of a drug free period after surgical
resection with curative intent.
When reviewing the literature, the authors identified
few case series and single case reports in the surgical
treatment of patients with isolated pancreatic MM
metastases. Although pancreatic resections for juxta
pancreatic MM metastases have been reported, these
were excluded from our analysis [30]. Given the inherent
difficulties in performing randomized prospective clinical
trial in the management of this disease, it appears that
in carefully selected patients with isolated pancreatic
metastases amenable to complete resection, surgery may
offer an overall survival benefit [5, 11, 18, 19, 21, 24, 25, 26, 27, 28, 29]. When selecting which patients should undergo
surgery four principles should be considered. First, the
patient age and comorbidities [23]; second, the tumour
biology (primary site/pathology report of primary/
interval between primary and metastases) [2, 9, 10, 20, 23, 31, 32]; third the preoperative workup (imaging/LDH) [9, 10, 32, 33, 34, 35, 36]; and fourth a complete resection of
all identifiable disease should be achievable [10, 20, 23].
Finally, given the rarity of this indication, the authors
suggest that a large-scale multi-institutional, prospectively
updated survey on surgical treatment of pancreatic
metastases (in as much as the Livermet Survey for
colorectal cancer liver metastases) could provide a more
expanded knowledge on the prognostic factors involved,
thus aiding in the decision-making process.
CONCLUSIONS
The authors fully acknowledge the limitations of this
review. As stated above, the literature review revealed a
heterogeneous collection of retrospective small case
series and single case reports; the time interval between
the first and the last article is nearly fifty years, with all
the developments and expertise gained in the fields of
adjuvant treatment and surgery. Furthermore, it is well
recognised that cases/series with poorer outcomes are
usually not reported in the literature; and we are also
aware of the short follow-up in the case we describe.
Nonetheless, there is sufficient encouraging experience
with resection of isolated pancreatic metastases from MM
that it should be considered in selected patients, as it may
provide a significant survival benefit for a disease with
high mortality and lack of effective systemic therapies.
Multidisciplinary decision and treatment in high volume
centres is mandatory.
Conflict of Interest
All authors are in agreement with the contents of the
manuscript. There is no conflict of interest.
References
- Globocan - Cancer Today n.d. https://gco.iarc.fr/today/home.
- Nikfarjam M, Evans P, Christophi C. Pancreatic resection for metastatic melanoma. HPB 2003; 5:174–9. [PMID: 18332980]
- Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta- Analyses: the PRISMA Statement. J Clin Epidemiol 2009; 62: 1006-12. [PMID: 19631508]
- Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M, et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 2017; 161:584–91. [PMID: 28040257]
- Wood TF, DiFronzo LA, Rose DM, Haigh PI, Stern SL, Wanek L, et al. Does complete resection of melanoma metastatic to solid intraabdominal organs improve survival? Ann Surg Oncol 2001; 8:658–62. [PMID: 11569781]
- Horner MJ, Ries LAG, Krapcho M, Neyman N, Aminou R, Howlader N, et al. SEER Cancer Statistics Review, 1975-2006, National Cancer Institute 2009:2000.
- National Cancer Institute - SEER stat facts. Patient Manag n.d.
- Nelson WG, De Marzo AM, Isaacs WB. Prostate cancer. N Engl J Med 2003; 349:366-81. [PMID: 12878745]
- Balch CM, Gershenwald JE, Soong SJ, Thompson JF, Atkins MB, Byrd DR, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol 2009; 27:6199–206. [PMID: 19917835]
- McLoughlin JM, Zager JS, Sondak VK, Berk LB. Treatment options for limited or symptomatic metastatic melanoma. Cancer Control 2008; 15:239–47. [PMID: 18596676]
- Gutman H, Hess KR, Kokotsakis JA, Ross MI, Guinee VF, Balch CM. Surgery for abdominal metastases of cutaneous melanoma. World J Surg 2001; 25:750–8. [PMID: 11376411]
- Sperti C, Polizzi ML, Beltrame V, Moro M, Pedrazzoli S. Pancreatic resection for metastatic melanoma. Case report and review of the literature. J Gastrointest Cancer 2011; 42:302–6. [PMID: 20524082]
- Stankard CE, Karl RC. The treatment of isolated pancreatic metastases from renal cell carcinoma: a surgical review. Am J Gastroenterol 1992; 87:1658–60. [PMID: 1442695]
- Z’graggen K, Fernández-del Castillo C, Rattner DW, Sigala H, Warshaw AL. Metastases to the pancreas and their surgical extirpation. Arch Surg 1998; 133:413-417; discussion 418-419. [PMID: 9565122]
- Reddy S, Wolfgang CL. The role of surgery in the management of isolated metastases to the pancreas. Lancet Oncol 2009; 10:287–93. [PMID: 19261257]
- Crippa S, Angelini C, Mussi C, Bonardi C, Romano F, Sartori P, et al. Surgical treatment of metastatic tumors to the pancreas: A single center experience and review of the literature. World J Surg 2006; 30:1536–42. [PMID: 16847716]
- Eidt S, Jergas M, Schmidt R, Siedek M. Metastasis to the pancreas-- an indication for pancreatic resection? Langenbecks Arch Surg 2007; 392:539–42. [PMID: 17242893]
- Reddy S, Edil BH, Cameron JL, Pawlik TM, Herman JM, Gilson MM, et al. Pancreatic Resection of Isolated Metastases from Nonpancreatic Primary Cancers. Ann Surg Oncol 2008; 15:3199–206. [PMID: 18784960]
- Hiotis SP, Klimstra DS, Conlon KC, Brennan MF. Results after pancreatic resection for metastatic lesions. Ann Surg Oncol 2002; 9:675– 9. [PMID: 12167582]
- Fletcher WS, Pommier RF, Lum S, Wilmarth T. Surgical Treatment of Metastatic Melanoma. Am J Surg 1998; 175:413–7. [PMID: 9600290]
- Showalter SL, Hager E, Yeo CJ. Metastatic Disease to the Pancreas and Spleen. Semin Oncol 2008; 35:160–71. [PMID: 18396201]
- Maverakis E, Cornelius LA, Bowen GM, Phan T, Patel FB, Fitzmaurice S, et al. Metastatic melanoma – A review of current and future treatment options. Acta Derm Venereol 2015; 95:516–24. [PMID: 25520039]
- Deutsch GB, Flaherty DC, Kirchoff DD, Bailey M, Vitug S, Foshag LJ, et al. Association of Surgical Treatment, Systemic Therapy, and Survival in Patients With Abdominal Visceral Melanoma Metastases, 1965-2014 : Relevance of Surgical Cure in the Era of Modern Systemic Therapy. JAMA Surg 2017; 111:980–4. [PMID: 28384791]
- Varker K a, Muscarella P, Wall K, Ellison C, Bloomston M. Pancreatectomy for non-pancreatic malignancies results in improved survival after R0 resection. World J Surg Oncol 2007; 5:145. [PMID: 18162131]
- Zerbi A, Ortolano E, Balzano G, Borri A, Beneduce AA, Di Carlo V. Pancreatic Metastasis from Renal Cell Carcinoma: Which Patients Benefit From Surgical Resection? Ann Surg Oncol 2008; 15:1161–8. [PMID: 18196343]
- Harrison LE, Merchant N, Cohen AM, Brennan MF. Pancreaticoduodenectomy for nonperiampullary primary tumors. Am J Surg 1997; 174:393–5. [PMID: 9337160]
- Lanitis S, Papaioannou N, Sgourakis G, Seitz A, Zacharakis E, Karaliotas C. Prolonged survival after the surgical management of a solitary malignant melanoma lesion within the pancreas: A case report of curative resection. J Gastrointest Liver Dis 2010; 19:453–5. [PMID: 21188341]
- Larsen AK, Krag C, Geertsen P, Jakobsen LP. Isolated malignant melanoma metastasis to the pancreas. Plast Reconstr Surgery Glob Open 2013; 1:e74. [PMID: 25289269]
- Birnbaum DJ, Moutardier V, Turrini O, Gonçalves A, Delpero JR. Isolated pancreatic metastasis from malignant melanoma: is pancreatectomy worthwile? J Surg Tech Case Rep 2013; 5:82–4. [PMID: 24741425]
- Belágyi T, Zsoldos P, Makay R, Issekutz Á, Oláh A. Multiorgan Resection (Including the Pancreas ) for Metastasis of Cutaneous Malignant Melanoma. JOP 2006; 7:234–40. [PMID: 16525211]
- Sugimoto M, Gotohda N, Kato Y, Takahashi S, Kinoshita T, Shibasaki H, et al. Pancreatic resection for metastatic melanoma originating from the nasal cavity: A case report and literature review. Anticancer Res 2013; 33:567–74. [PMID: 23393350]
- Bhatia S, Tykodi SS, Thompson JA. Treatment of metastatic melanoma: an overview. Oncology (Williston Park) 2009; 23:488–96. [PMID: 19544689]
- Brady MS, Akhurst T, Spanknebel K, Hilton S, Gonen M, Patel A, et al. Utility of preoperative [(18)]f fluorodeoxyglucose-positron emission tomography scanning in high-risk melanoma patients. Ann Surg Oncol 2006; 13:525–32. [PMID: 16474909]
- Fogarty GB, Tartaglia C. The utility of magnetic resonance imaging in the detection of brain metastases in the staging of cutaneous melanoma. Clin Oncol 2006; 18:360–362. [PMID: 16703756]
- Fuster D, Chiang S, Johnson G, Schuchter LM, Zhuang H, Alavi A. Is 18F-FDG PET more accurate than standard diagnostic procedures in the detection of suspected recurrent melanoma? J Nucl Med 2004; 45:1323– 7. [PMID: 15299056]
- Perng P, Marcus C, Subramaniam RM. 18F-FDG PET/CT and melanoma: Staging, immune modulation and mutation-targeted therapy assessment, and prognosis. Am J Roentgenol 2015; 205:259–70. [PMID: 26204273]
- Johansson H, Krause U, Olding L. Pancreatic metastases from a malignant melanoma. Scand J Gastroenterol 1970; 5:573-5. [PMID: 5474426]
- Bianca A, Carboni N, Di Carlo V, Falleni M, Ferrero S, Liverani C, et al. Pancreatic malignant melanoma with occult primary lesion. A case report. Pathologica 1992; 84:531–7. [PMID: 1491895]
- Brodish RJ, McFadden DW. The pancreas as the solitary site of metastasis from melanoma. Pancreas 1993; 8: 276–8. [PMID: 8460104]
- Medina-Franco H, Halpern NB, Aldrete JS. Pancreaticoduodenectomy for metastatic tumors to the periampullary region. J Gastrointest Surg 1999; 3: 119-22. [PMID: 10457332]
- Carboni F, Graziano F, Lonardo MT, Lepiane P, Santoro R, Lorusso R, et al. Pancreaticoduodenectomy for pancreatic metastatic melanoma. J Exp Clin Cancer Res 2004; 23: 539–43. [PMID: 15595647]
- Vagefi PA, Stangenberg L, Krings G, Forcione DG, Wargo JA. Ocular melanoma metastatic to the pancreas after a 28-year disease-free interval. Surgery 2010; 148:151–4. [PMID: 19744448]
- He MX, Song B, Jiang H, Hu XG, Zhang YJ, Zheng JM. Complete resection of isolated pancreatic metastatic melanoma: a case report and review of the literature. World J Gastroenterol 2010; 16:4621–4. [PMID: 20857537]
- Portale TR, Di Benedetto V, Mosca F, Trovato MA, Scuderi MG, Puleo S. Isolated pancreatic metastasis from melanoma. G Chir 2011; 32:135–7. [PMID: 21453593]
- Goyal J, Lipson EJ, Rezaee N, Edil BH, Schulick R, Wolfgang CL, et al. Surgical Resection of Malignant Melanoma Metastatic to the Pancreas: Case Series and Review of Literature. J Gastrointest Cancer 2011; 43:431– 6. [PMID: 21912850]
- De Moura DT, Chacon DA, Tanigawa R, Coronel M, Cheng S, Artifon ÉL, et al. Pancreatic metastases from ocular malignant melanoma: the use of endoscopic ultrasound-guided fine-needle aspiration to establish a definitive cytologic diagnosis: a case report. J Med Case Rep 2016; 10:332. [PMID: 27906105]
- Yagi T, Hashimoto D, Taki K, Yamamura K, Chikamoto A, Ohmuraya M, et al. Surgery for metastatic tumors of the pancreas. Surg Case Rep 2017; 3:31. [PMID: 28214950]
- Mehta M, Omer E. Isolated Metastatic Melanoma to the Pancreas Diagnosed by Endoscopic Ultrasonography : A Case Report. JOP 2017; 18:144–6.
- Liu X, Feng F, Wang T, Qin J, Yin X, Meng G, et al. Laparoscopic pancreaticoduodenectomy for metastatic pancreatic melanoma: A case report. Medicine (Baltimore) 2018; 97:e12940. [PMID: 30383642]




