Giacomo Murana, Luca Di Marco*, Loforte Antonino, Jacopo Alfonsi, Roberto Di Bartolomeo and Davide Pacini
Cardiac Surgery Department, S. Orsola- Malpighi-Hospital, Alma Mater Studiorum, University of Bologna, Bologna, Italy
*Corresponding Author:
Luca Di Marco
Cardiac Surgery Department, S. Orsola- Malpighi-Hospital, Alma Mater Studiorum, University of Bologna, Bologna, Italy
Tel: 00390512143329,
Fax:+39-051-345990
E-mail: ludima08@libero.it
Received Date: January 14, 2016; Accepted Date: March 11, 2016; Published Date: March 16, 2016
Citation: Murana G, Marco LD, Antonino L, et al., Surgical Management of a Multi-Catheters Entrapment Following Percutaneous Coronary Intervention. Interv Cardiol J 2015, 2:1. DOI: 10.21767/2471-8157.100014
Keywords
Intravascular ultrasound, Percutaneous catheters entrapment, Percutaneous coronary intervention (PCI), Coronary artery bypass grafting (CABG)
Introduction
Intravascular ultrasound (IVUS) procedure is poorly associated (0.5%) with severe complications such as dissection, acute vessel closure, embolism, and thrombus [1,2]. Intracoronary entrapment of multiple percutaneous devices is even more-rare.
In the following case we describe a dramatic clinical scenario of a patient that underwent a rescue coronary bypass surgery following a double failing PCI procedure because of an IVUS catheter entanglement inside the left anterior descending artery (LAD).
Case Report
A 55-year-old man with the history of coronary artery disease was hospitalized to a local regional hospital for the onset of unstable angina symptoms. Nine years before he underwent a double bare metal stent (BMS) implantation in both the LAD and right coronary artery. An allergy to clopidogrel was reported.
The patients underwent urgent percutaneous coronary intervention (PCI) that revealed the patency of the previously implanted BMS in the right coronary artery and two new stenosis of the LAD (intra-BMS and of the distal tract of the vessel). A 40 MHz, 3.2F, IVUS (Atlantis SR Pro; Boston Scientific, MN, USA) was then performed to better evaluate the lesions of the LAD-BMS. It showed a significant lesion inside the BMS with a severely diseases distal coronary artery and no signs of stent malposition. During the procedure the tip of the IVUS catheter remained captured into the BMS mesh and fractured inside the vessel (Figure 1A). Several attempts to retract the IVUS catheter and to open the partially occluded coronary vessel were done. In the light of the failed procedure two hours later, the patient was then referred to our hospital for a heart team evaluation. Afterthat, we decided to perform an urgent PCI retrieval using a 5 mm AndraSnare nitinol loop (Andramed, Reutlingen Germany) (Figure 1B). Unfortunately, this second attempt to forceful withdrawal the guide of the IVUS caused a complex entanglement of the catheters with a consequent BMS migration and a complete occlusion of the coronary vessel (Figure 1C). The patient developed chest pain and electrocardiogram (ECG) indicated ischemic changes in the anterolateral region of the left ventricle. He was quickly transported inside the operating theater for emergency coronary artery bypass grafting. After median sternotomy and pericardial opening, the proximal portion of the coronary vessel appeared hemorrhagic (Figure 2A). The ascending aorta was opened. We try to manually retract the catheters but it could not be possible due to strong adhesions developed by the catheters. Therefore, the LAD was cut immediately before the stent origin and the entrapped catheters in the edge of the BMS structure were visualized. To completely remove the foreign materials inside the vessel and restore the physiologic blood flow an extended thromboendarterectomy was necessary (Figure 2B). Finally, the arterial rerouting was achieved with a jumping sequential anastomosis using the distal end of the vein graft to reconstruct the damaged artery (Figure 2C). During the first three days after surgery myocardial enzymes slowly normalized (max troponine 4441 ng/L). At discharge, ECG showed Q waves on the anterolateral wall region of the left ventricle and echocardiogram confirmed the area of akinesis (EF 45%). Patient went home on post-operative day 10.
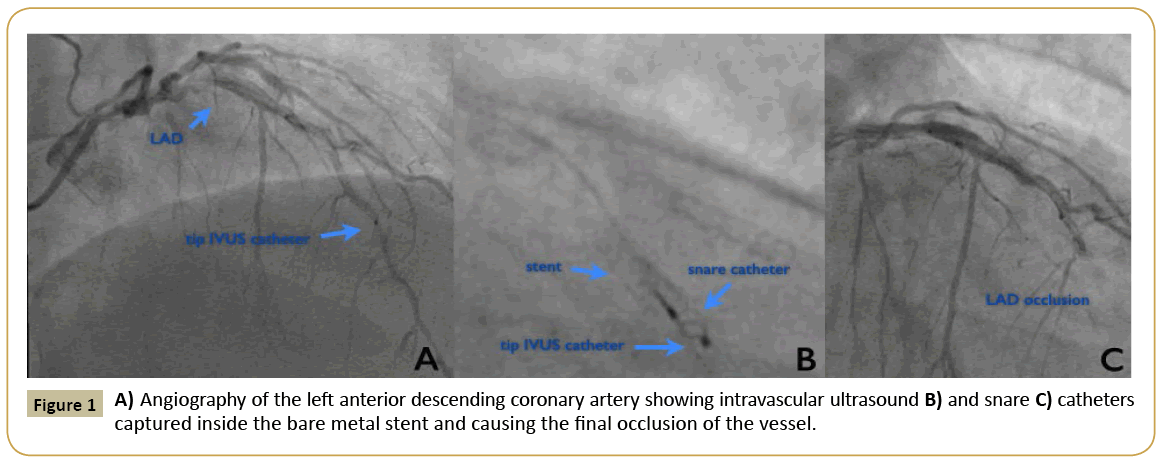
Figure 1: A) Angiography of the left anterior descending coronary artery showing intravascular ultrasound B) and snare C) catheters captured inside the bare metal stent and causing the final occlusion of the vessel.
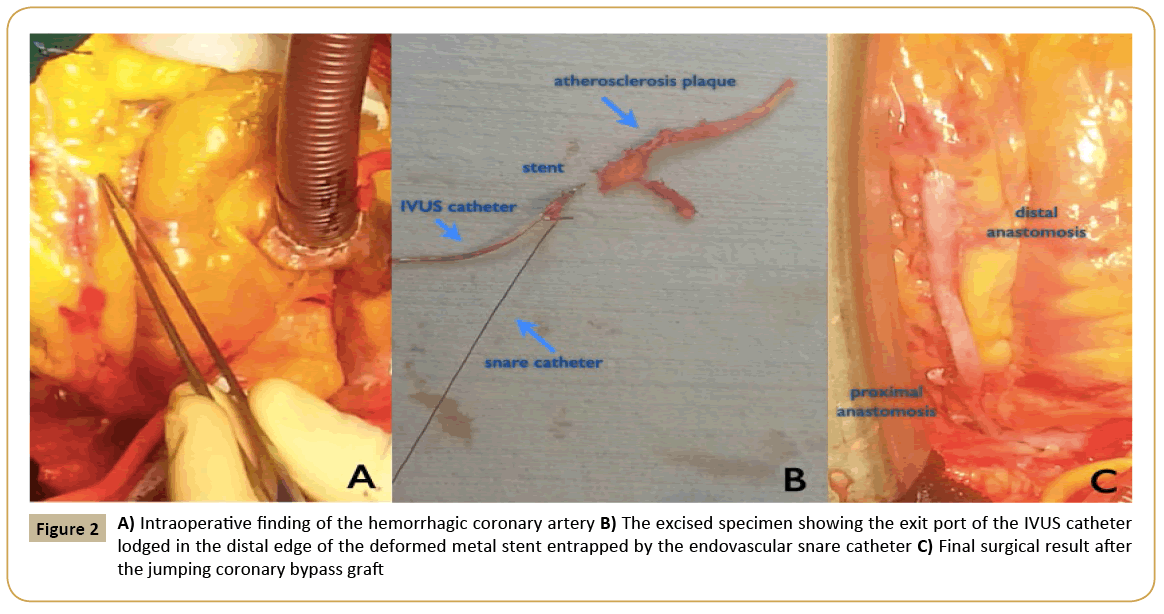
Figure 2: A) Intraoperative finding of the hemorrhagic coronary artery B) The excised specimen showing the exit port of the IVUS catheter lodged in the distal edge of the deformed metal stent entrapped by the endovascular snare catheter C) Final surgical result after the jumping coronary bypass graft
Discussion
In this unusual case a complex multi catheters entrapment occurred. Unfortunately, revascularization was obtained 6 hours later from the initial intimal ischemic injury inside the cardiac chat lab and this caused an extensive and irreversible damage of the myocardium. Major reasons can be found in the management of the unusual situation for the physicians in the local cardiology department and time necessary to reach the closest cardiac surgery after the trans-catheter procedure failed. According to literature a successful bypass surgery is determined primarily by the clinical status of the patient before the operation with a high risk of death (20%-50%) if the patients is in cardiogenic shock [3,4]. In our situation, the prolonged unstable hemodynamic status associated with the ST elevation myocardial infarction caused an extensive and irreversible damage of the myocardium. In a previous report, the mechanism of catheters entrapment during the IVUS procedure was the captured distal edge on the guide wire exit port in coronary stent after the catheter was retracted [5]. In our patient a more complex situation occurred because the second attempt to withdrawal the guide of the IVUS caused also the entaglement of the snare catheter causing the complete occlusion of the coronary vessel. Surgical treatment in this particular situation appears to be the only curative option in order to restore the blood flow in the LAD territory. In this case the procedure was technically demanding for several reasons. Firstly, a long arteriotomy was needed in order to remove the entire stent and take out the catheters that coiled around it. Secondly, an extended endarterectomy was necessary because the distal part of the coronary appeared to be totally occluded by the atherosclerotic plaque. Thirdly, the LAD was hardly reconstructed with a long pedicle of saphenous vein.
Conclusion
This type of PCI complication could be an example of daily heart team challenges. In our opinion, during complex cardiac endovascular procedures, it should be advised to have on-site the cardiac surgery to better manage possible complications of these high risky procedures.
References
- Hausmann D, Erbel R, Alibelli-Chemarin MJ, Boksch W, Caracciolo E, et al. (1995) The safety of intracoronary ultra- sound: a multicenter survey of 2207 examinations. Circulation 91:623-630.
- Nissen SE, Yock P (2001) Intravascular ultrasound: novel patho-physiological insights and current clinical applications. Circulation 103:604–616.
- Sasseen BM, Burke JA, Shah R, Costa MA, Zenni M, et al. (2002) Intravascular ultrasound catheter entrapment after coronary artery stenting. Catheter Cardiovasc Interv 57: 229-233.
- Minami H, Asada T, Gan K, Yamada A, Sato M (2011) Surgical removal of an intravascular ultrasonography catheter captured in a stent after percutaneous coronary intervention. Gen Thorac Cardiovasc Surg 59:181-183.
- Ako J, MorinoY, Honda Y, Hassan A, Sonoda S, et al. (2005) Late incomplete stent apposition after sirolimus-eluting stent implantation: a serial intravascular ultrasound analysis. J Am Coll Cardiol 46:1002-1005.

