Keywords
Pancreas; Pancreatic Neoplasms
Abrreviations
IQR interquartile range; SPN solid pseudopapillary
neoplasm
INTRODUCTION
Solid pseudopapillary neoplasm (SPN, SPT) – is a rare
pancreatic tumor which arises from exocrine type cells and
has a specific progesterone receptors. It was described by
American pathologist Virginia Kneeland Frantz in 1959 [1].
SPN has different names such as solid pseudopapillary
tumor, Frantz tumor or Hamoudi tumor. SPNs compose
less than 1% of exocrine tumors of the pancreas. According
the data of National Health Institute of USA there were
2744 cases of SPN published in 484 articles in the world
literature for period 1961- 2012. Most of them are
presented as a case reports or series of several cases [2, 3].
At the present time SPN still stays a rare and difficult
pancreatic tumor for efficient preoperative diagnostics,
surgical treatment and adequate postoperative
morphological verification. In this paper we describe
diagnostic features and surgical techniques for patients
with SPN based on our experience of 37 cases.
MATERIALS AND METHODS
Retrospective analysis of medical records for period
2007 – 2017 was performed in Abdominal Department No.1
A.V. Vishnevsky Institute of Surgery, Moscow, Russia. It was
found 38 morphologically confirmed cases of SPNs. Surgical
treatment has been performed in 37 cases; one patient
without operative management was excluded from our study.
Data Presentation and Statistical Analysis
Sample-size calculation was not necessary because we
have not planed any comparison in this study. All recorded
data of population were analyzed according the Intentionto-
treat method. Dichotomous variables were recorded
as absolute frequencies (number of cases) and relative
frequencies (percentages).
Data were presented as median and interquartile range
(IQR) 25% and 75% if not indicated otherwise.
RESULTS
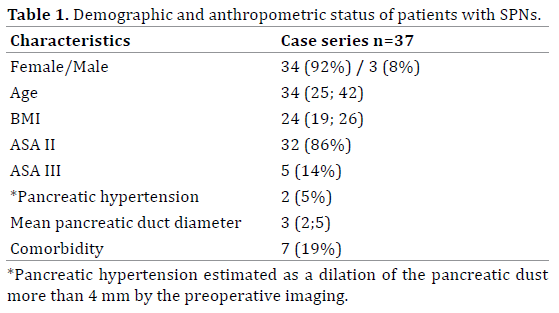
Demographic Data
Absolute majority of patients were female – 34 (92%)
cases, there were only 3 (8%) male with confirmed SPNs. Mean average age of patients was 34 (25; 42) years.
Preoperative anthropometric estimation included also
body mass index (BMI), ASA risk score stratification,
complications and comorbidities. Information about
demographic and anthropometric status is shown in Table 1.
Clinics and Preoperative Diagnostics
The most of SPN cases became an accident finding
during prophylactic checkup or examination because of
comorbidities. Clinically most common symptoms were
weakness or minimal nagging pain, rarely - nausea or even
palpated hard growth (Table 2).
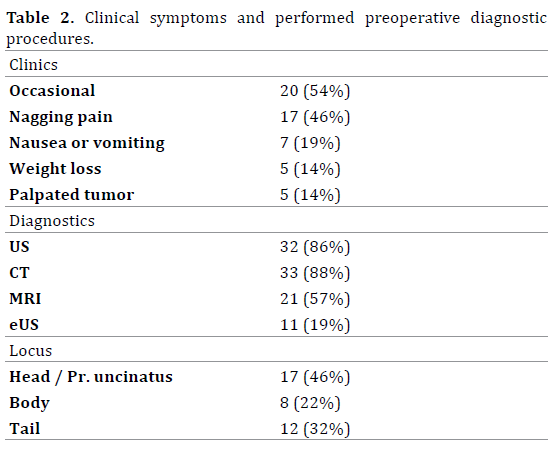
Preoperative diagnostic included transcutaneous
abdominal ultrasound (US), computed tomography (CT)
with obligatory intravenous contrast infusion, magnetic
resonance imagination (MRI) and endoscopic ultrasound
(EUS). Preoperative gastroscopy was routinely performed
in all cases. Quantity and percentage of diagnostic
procedures measured. In difficult cases ultrasound guided
fine-needle aspiration biopsy was performed. There were
no special laboratory tests such as Chromogranin A, CA 19-9,
CEA or α-FP performed during preoperative diagnostic step.
Preoperative instrumental examination showed that
frequently tumor was located in proximal part of the
pancreas, rarely – in pancreatic body and tail. Mean tumor
diameter was 42 (26; 73) mm. At the CT or MRI scans SPNs
looked like a solid round hyper – or isodense tumor without
pancreatic hypertension in most (95%) of cases (Figure 1).
Figure 1. Preoperative MRI of SPN located in pancreatic body. (a). MRI scan, axillar projection, (b). MRCP scan.
Performed Surgeries
After preoperative examination in 37 patients
underwent surgical treatment. All types of pancreatic
resections including standard and organ-preserving
procedures were performed. Type of resection depended
of tumor location, diameter and size of extra-pancreatic
component. Most of patients (78%) were operated
conventionally. In 8 (22%) cases procedure was realized
using robotic complex DaVinci S.
Most of all (81%), there were standard pancreatic
resections such as pancreaticoduodenectomy (PD)
or distal pancreatectomy (DP). Rarely, it were organ–
preserving procedures such as tumor enucleation (TE) or
median resection (ME) (Table 3). Indications for TE were
benign presence of tumor without loco-regional or distant
metastasis, more than 75% of extrapancreatic tumor
component and more than 3 mm distance from pancreatic
duct. MR was performed for intraparenchimatously
located pancreatic body tumors.
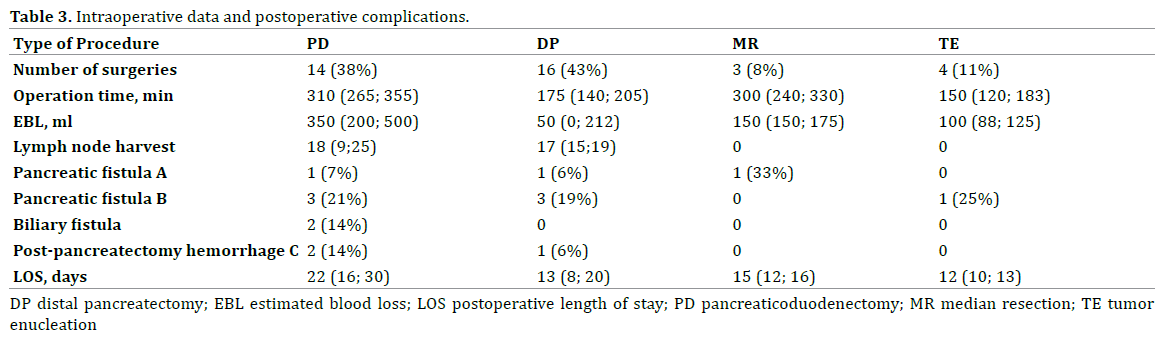
During PD or DP standard lymphadenectomy D2
was made with median lymph node harvests 18 and 17
respectively. While organ-preserving procedures normally
lymphadenectomy was not necessary. DP with spleen
preservation was preferred and performed in 13 (81%) of
all DPs.
Postoperative specific complications were typical
for pancreatic surgery. They were classified according
to ISGPS classification [4, 5, 6]. Most frequently it was
type B pancreatic fistula. There were no Type C fistulas.
Mortality rate was 1 (3%) of all performed surgeries. It
was young woman with severe postoperative necrotising
pancreatitis and respiratory distress syndrome. In Table 3 demonstrated details of intraoperative data and
postoperative complications.
Diagnosis Verification and Confirmation
The tissues were dissected and fixed in 10% formalin
(Fisher Scientific). The tissues were then embedded
in paraffin, and serial tissue sections were made at
five μm thickness. Immunohistochemistry (IHC) was
performed in cut sections of pancreatic tumors using
Synaptophysin, Cr A, PR, beta-catenin, CD99, CK 8/18
using the immunoperoxidase method. Antigen retrieval
was performed using CC1 antigen retrieval buffer (pH
8.5, EDTA, 100°C, 30 minutes; Ventana) for all sections.
Following incubation with the primary antibodies (37°C,
32 minutes) in phosphate buffered saline, pH 7.4 (PBS)
with 1% bovine serum albumin (BSA), sections were
stained on a Benchmark XT automated slide stainer using a
diaminobenzidine detection kit (UltraView DAB, Ventana).
Frozen section of resection margin was performed
during all procedures. Pancreatic resection margins were
tumor free (R0) in all cases.
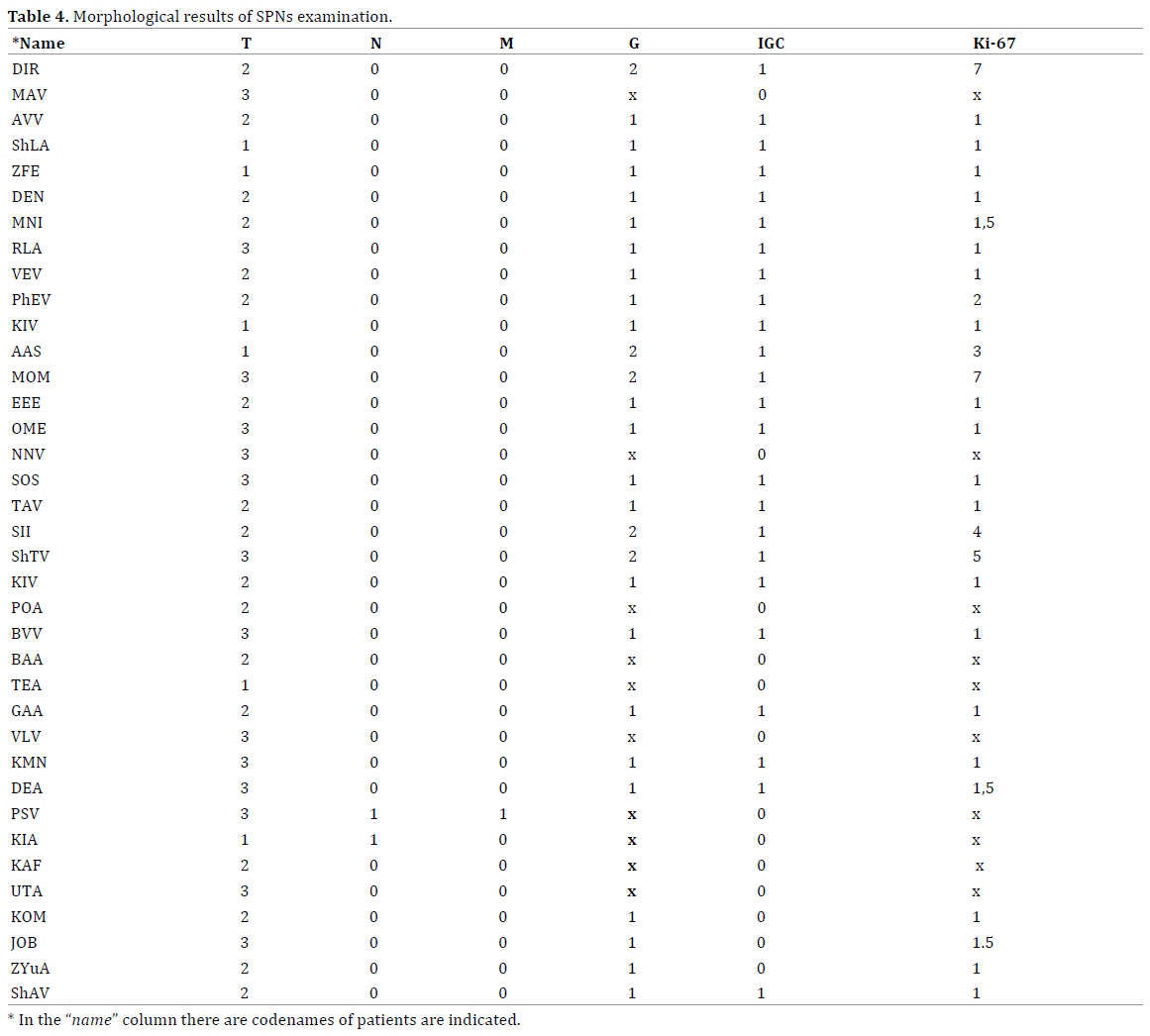
Morphological examination of specimens was routinely
performed. In 27 (73%) cases diagnosis of SPN was
confirmed with immunohystochemical analysis (IHC), otherwise by electronic microscopy. Morphological
specimen examination found out that most of tumors were
benign (G1), rarely it were grade 2 neoplasms. In two cases
lymph node metastasis were diagnosed and only in one
case there was confirmed liver metastasis. Unfortunately
in these cases IHC wasn’t performed, so proper tumor
grade wasn`t verified. Morphological characteristics with
TNM data, grade and Ki-67 index of tumors measured in
Table 4.
DISCUSSION
SPN still stays rare uncommon pancreatic neoplasm.
From the date of its official description until 2012 there
were only 2744 cases of this tumor revealed in the world
literature [2, 3]. Found papers included 484 publications;
most of them were presented as a case report or series of
several cases. From 2012 till present days several large
single- and multicentre studies of SPN surgical treatment
were published [3, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17,
18, 19]. After detailed literature review we revealed 3725
cases of confirmed SPNs in adult persons including our
experience (Table 5).
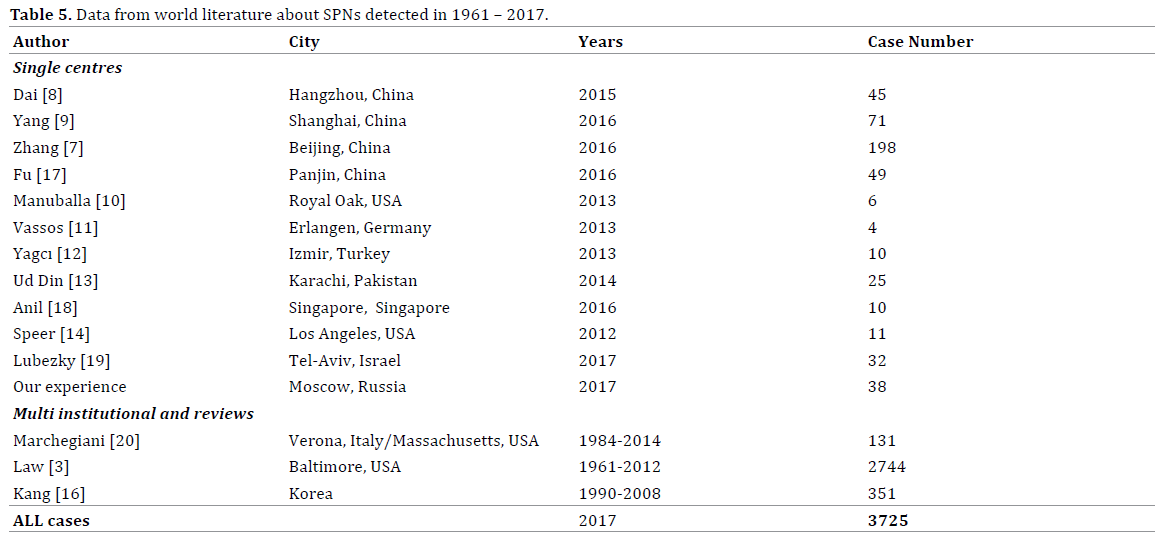
Most of recent studies were presented from large
clinics and research centres, especially from China. In our
opinion, explanation of this can be the concentration of
pancreatic surgery in multidisciplinary centres, adequate
and contemporary diagnostic verification. In Figure 1 we accommodated all found case series with more than 3
cases including not only single centre experience but also
multicentre collaborations and literature reviews. At the
same time we excluded earlier publications from the same
centres, which repeat cases cohorts.
Basing on our experience, we suggested that it will
be increasing prevalence of SPNs from year to year. But
analysis didn’t show significant deviation and didn’t
depend of progression in learning curve of our department
(Figure 2). Moreover, there were periods of time with
minimal detection of this tumor with twice lower grade
than the median value (Figure 2). It can be explained by
increasing quantity of high-volume pancreatic centres and
the rareness of this tumor.
Figure 2. Prevalence of SPNs in our centre from 2007 till 2017 (violate
line is the median of detection). There is no increasing of SPN diagnosed
in our centre.
SPN mostly occurs in young women under 35 years
[3, 15, 16]. There are no specific symptoms of this tumor
that’s why it can be frequently found during follow- up
examination or treatment because of comorbid disease.
Unlike of ductal adenocarcinoma it hasn’t invasive growth
and doesn’t develop pancreatic hypertension, parenchyma
atrophy or diabetes [20].
Considering the fact that SPN is a very rare tumor and
there are less than four thousand adult cases described
in the world literature, it’s very difficult to understand epidemiology and predictive growing factors of this tumor.
It`s definitely clear, that SPN has a specific progesterone
receptors so young women are the main risk group for this
disease. Moreover, it could be interesting to investigate
epidemiological features and predictive factors of
occurrence SPN in male cases.
We hope that described step-by-step diagnostics, surgical
treatment and morphological verification of SPN based on
our experience can become not only a guide for management
this group of patients but it can become a start to deeper
epidemiologic and survival analysis all over the world. We
think in that regard it’s more important to publish single
centres experience than collaborations between different
centres in one country even worse several countries on
different continents. And definitely clear that research centres
which are interested and have an experience in described
problem could work together to understand the nature of
disease and may be at some point absolutely eradicate it.
CONCLUSION
Solid pseudopapillary neoplasm of the pancreas is
a rare originating tumor with progesterone receptors.
At the present time there are about four thousand cases
described in the world’s literature. In our study we present
38 cases of SPN, and 37 of them underwent surgical
treatment. We think that international society has to be
formed to improve results of revealing, adequate surgical
and therapeutic treatment of this tumor.
Conflict of interest
Authors report no conflicts of interest. The authors
alone are responsible for the content and writing of the
paper.
References
- Frantz VK. Tumors of the pancreas. In: Bumberg CW, editor. Atlas of
tumor pathology. VII. Fascicles 27 and 28. Washington: Armed Forced
Institute of Pathology 1959; p. 32–39.
- Martin RC, Klimstra DS, Brennan MF, Conlon KC. Solid pseudopapillary
tumor of the pancreas: a surgical enigma? Ann Surg Oncol 2002; 9:35-
40. [PMID: 11833495]
- Law JK, Ahmed A, Singh VK, Akshintala VS, Olson MT, Raman SP, et
al. A systematic review of solid-pseudopapillary neoplasms: are these
rare lesions? Pancreas 2014; 43:331–7. [PMID: 24622060]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al.
Postoperative pancreatic fistula: an international study group (ISGPF)
definition. Surgery 2005; 138:8-13. [PMID: 16003309]
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, et
al. Postpancreatectomy hemorrhage (PPH): an International Study
Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007; 142:20-
5. [PMID: 16003309]
- Besselink MG, van Rijssen LB, Bassi C, Dervenis C, Montorsi M, Adham
M, et al. Definition and classification of chyle leak after pancreatic
operation: A consensus statement by the International Study Group on
Pancreatic Surgery. Surgery 2017; 161:365-372. [PMID: 27692778]
- Zhang H, Wang W, Yu S, Xiao Y, Chen J. The prognosis and clinical
characteristics of advanced (malignant) solid pseudopapillary
neoplasm of the pancreas. Tumour Biol 2016; 37:5347-53.
[PMID: 26561472]
- Dai G, Huang L, Du Y, Yang L, Yu P. Solid pseudopapillary neoplasms of
the pancreas: clinical analysis of 45 cases. Int J Clin Exp Pathol 2015;
8:11400-6. [PMID: 26617866]
- Yang F, Yu X, Bao Y, Du Z, Jin C, Fu D. Prognostic value of Ki-67 in
solid pseudopapillary tumor of the pancreas: Huashan experience
and systematic review of the literature. Surgery 2016; 159:1023-31.
[PMID: 26619927]
- Manuballa V, Amin M, Cappell MS. Clinical presentation and comparison
of surgical outcome for segmental resection vs. Whipple's procedure for
solid pseudopapillary tumor: Report of six new cases & literature review
of 321 cases. Pancreatology 2014; 14:71-80. [PMID: 24555981]
- Vassos N, Agaimy A, Klein P, Hohenberger W, Croner RS. Solidpseudopapillary
neoplasm (SPN) of the pancreas: case series and
literature review on an enigmatic entity. Int J Clin Exp Pathol 2013;
6:1051-9. [PMID: 23696922]
- Yagcı A, Yakan S, Coskun A, Erkan N, Yıldırım M, Yalcın E, et al.
Diagnosis and treatment of solid pseudopapillary tumor of the
pancreas: experience of one single institution from Turkey. World J
Surg Oncol 2013; 11:308. [PMID: 24289652]
- Ud Din N, Arshad H, Ahmad Z. Solid pseudopapilllary neoplasm of
the pancreas. A clinicopathologic study of 25 cases from Pakistan
and review of Literature. Ann Diagn Pathol 2014; 18:358-62.
[PMID: 25438925]
- Speer AL, Barthel ER, Patel MM, Grikscheit TC. Solid pseudopapillary
tumor of the pancreas: a single-institution 20-year series of pediatric
patients. J Pediatr Surg 2012; 47:1217-22. [PMID: 22703796]
- Kang CM, Choi SH, Kim SC, Lee WJ, Choi DW, Kim SW. Predicting
recurrence of pancreatic solid pseudopapillary tumors after surgical
resection: a multicenter analysis in Korea. Ann Surg 2014; 260:348-
55. [PMID: 24743622]
- Fu XB, Hao ZQ, He JY, Shang H, Fu QC, Hua XD, et al. Pathology
comparative study on the characteristic CT signs in solid
pseudopapillary neoplasm of the pancreas. Exp Ther Med 2017;
13:3523-3528. [PMID: 28587436]
- Anil G, Zhang J, Al Hamar NE, Nga ME. Solid pseudopapillary neoplasm
of the pancreas: CT imaging features and radiologic-pathologic
correlation. Diagn Interv Radiol 2017; 23:94-99. [PMID: 28089954]
- Lubezky N, Papoulas M, Lessing Y, Gitstein G, Brazowski E, Nachmany
I, et al. Solid pseudopapillary neoplasm of the pancreas: Management
and long-term outcome. Eur J Surg Oncol 2017; 43:1056-1060.
[PMID: 28238521]
- Naar L, Spanomichou DA, Mastoraki A, Smyrniotis V, Arkadopoulos
N. Solid Pseudopapillary Neoplasms of the Pancreas: A Surgical and
Genetic Enigma. World J Surg 2017; 41:1871-1881. [PMID: 28251269]
- Marchegiani G, Andrianello S, Massignani M, Malleo G, Maggino
L, Paiella S, et al. Solid pseudopapillary tumors of the pancreas:
Specific pathological features predict the likelihood of postoperative
recurrence. J Surg Oncol 2016; 114:597-601. [PMID: 27471041]



