Keywords
Alcohol sales; suicide rates; ARIMA time series analysis; Russia; Belarus; 1970-2014.
Introduction
Suicide is one of the leading external causes of death in many countries and it burden is expected to be rising over the next several decades [1]. The Slavic countries of the former Soviet Union (fSU) Russia and Belarus retain one of the highest suicide rates in the world, despite a gradual decline over the past decade [2,3]. The reason of high suicide mortality in fSU countries is not fully understood. A number of variables, including socioeconomic factors, religious and biological background should be considered [3,4]. The developments in suicide mortality in fSU countries have been particularly dramatic in connection with the societal processes of the last decades including the period of reforms known as “perestroika” and the collapse of the Soviet Union [5]. The dramatic fluctuations in suicide mortality in fSU over the past decades have been widely discussed in the scientific literature and are still relatively unexplored [5-10]. Although all the former Soviet republics experienced similar societal transformation, the effect of these transformations in relation to suicide mortality has not been identical [11].
Cross-country comparative studies may be particularly useful to test the hypothesis that social structure and macroeconomic differences across countries affect the suicide rates. The Slavic countries of the fSU Russia and Belarus share a longer common history and experienced similar socioeconomic development during the Soviet period [12]. The marked similarities in socioeconomic and mortality trends in the countries during the Soviet period contrast with their notable divergence after the collapse of the Soviet Union in 1991 [7]. In comparative perspective, the developmental path in Belarus has been somewhat different to that seen in Russia in the post-Soviet period. There has been less emphasis on economic reform in Belarus, with many aspects of the command economy being retained, as witnessed by the low level of privatization [13]. By contrast, Russia has chosen more radical forms of economic transformations, which have led to massive privatization campaigns [14].
Accumulated evidence suggests that the mixture of cultural acceptance of heavy drinking, high rate of distilled spirits consumption, and binge drinking pattern is major contributor to the suicide mortality burden in fSU countries [15-21]. Recent case-control study indicated that hazardous drinking substantially increases the risk of suicide among working-age Russian males, with nearly half of all suicides attributed to this drinking pattern [22]. Aggregate-level studies also reveal an association between population level drinking and suicide rates in Russia and Belarus [23-30]. Furthermore, evidence of the time series association dates back over a century for the Tsarist era and continues through the Soviet and post-Soviet period [31]. However, several studies did not confirm an association between alcohol consumption and suicide rates in the post-Soviet period [4,6].
The present study aims to analyze whether population drinking is able to explain the dramatic fluctuations in suicide mortality in Russia and Belarus from the late Soviet to post-Soviet period. More specifically, this study focuses on a comparative analysis of trends in suicide rates and alcohol sales per capita in these countries between 1970 and 2014.
Methods
Data
The data on suicide rates (per 100.000 of the population) and data on per capita alcohol sales (in liters of pure alcohol) are taken from the Russian State Statistical Committee (Rosstat) reports and Belarusian State Statistical Committee (Belsstat). The data were broken into two periods (from 1970 to 1999 and from 2000 to 2014) to determine whether the link between alcohol sales and suicide rates has altered in recent years.
Statistical analysis
To examine the relation between changes in alcohol sales and suicide rates across the study period a time-series analysis was performed using the statistical package "Statistica". The dependent variable was the suicide rates and the independent variable was aggregate alcohol sales. Bivariate correlations between the raw data from two time-series can often be spurious due to common sources in the trends and due to autocorrelation [32]. One way to reduce the risk of obtaining a spurious relation between two variables that have common trends is to remove these trends by means of a ‘differencing’ procedure, as expressed in formula:
∇xt = xt - xt-1
This means that the annual changes ‘∇’ in variable ‘X’ are analyzed rather than raw data. The process whereby systematic variation within a time series is eliminated before the examination of potential causal relationships is referred to as ‘prewhitening’. This is subsequently followed an inspection of the cross-correlation function in order to estimate the association between the two prewhitened time series. It was Box and Jenkins [33] who first proposed this particular method for undertaking a time series analysis and it is commonly referred to as ARIMA modeling. We used this model specification to estimate the relationship between the time series suicide rates and alcohol sales in this paper. In line with previous aggregate studies [32] we estimated semi-logarithmic models with logged output. A semi-logarithmic model is based on the assumption that the risk of suicide increases more than proportionally for a given increase in alcohol consumption [32]. The following model was estimated:
∇LnMt = a + β∇At + ∇Nt
where ∇ means that the series is differenced, M is suicide rates, a indicates the possible trend in suicide rates due to other factors than those included in the model, A is the alcohol sales, β is the estimated regression parameter, and N is the noise term. The percentage increase in suicide rates associated with a 1-litre increase in alcohol sales is given by the expression: (exp(β1)-1)*100.
The effect of alcohol consumption on suicide mortality rate will be expressed in terms of alcohol-attributable fraction (AAF), which is interpreted as the proportion of suicide deaths that is attributable to alcohol. AAF can be calculated from the estimates obtained in ARIMA models according to formula: AAF = 1-exp(- bX), where X is alcohol sales per capita and b is the estimated effect parameter [32].
Results
The average suicide rates figure for Russia and Belarus was 29.7 ± 5.4 and 25.7 ± 5.8 per 100.000 respectively. Since the early 1970s, suicide mortality in these countries has undergone sharp fluctuations (Figure 1). In general, the temporal pattern of suicide mortality fluctuations was similar for both countries: sharp decrease in the mid of 1980s, dramatic increase in the first half of 1990s followed by a decline. While the trends in suicide mortality have been similar in both countries during the Soviet period, there was market discrepancy after the collapse of the Soviet Union. In Russia suicide rate jumped dramatically between 1991 and 1994 (+57.3%). There was also a spike in suicide mortality between 1999 and 2001 in Russia. In Belarus, suicide rates increased dramatically between 1991 and 1996 (+67.3%) and then started to decrease. The comparative analysis of longterm evolution of suicide rate suggests that in the 1970s the rate was considerably lower in Belarus than in Russia, but this gap practically disappeared in most recent years.
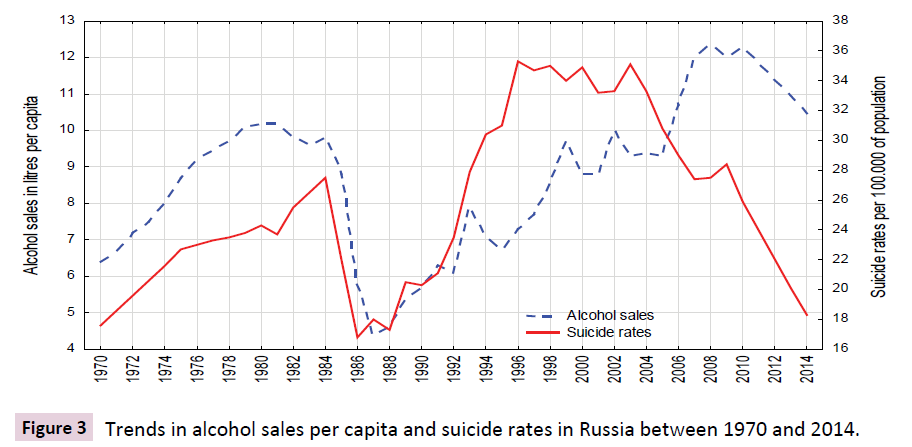
Figure 1: Trends suicide rates in Russia and Belarus between 1970 and 2014.
The average per capita alcohol sales figure for Russia and Belarus was 8.4 ± 1.8 and 8.6 ± 2.0 litres per capita respectively. The temporal pattern of alcohol sales per capita in Russia and Belarus was similar across the Soviet period (Figure 2 and 3). As can be seen, the alcohol sales decreased slightly in the early 1980s, and then decreased dramatically between 1984 and 1987. After the collapse of the Soviet Union, recorded alcohol consumption in Russia rose sharply between 1992 and 1995, decreased substantially in 1996, increased steadily up to 2007, and then started to decrease. In the post-Soviet Belarus alcohol sales increased steadily with several oscillations up to 2005, than jumped dramatically, and since 2011 started to decrease.
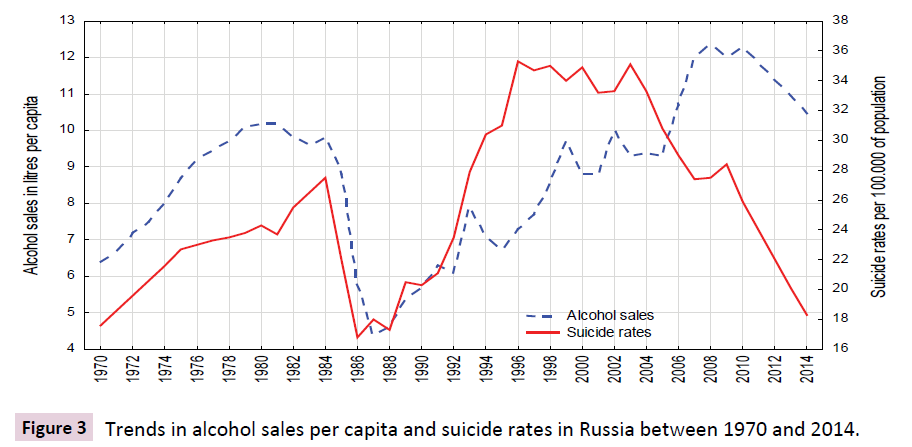
Figure 2: Trends in alcohol sales per capita and suicide rates in Russia between 1970 and 2014.
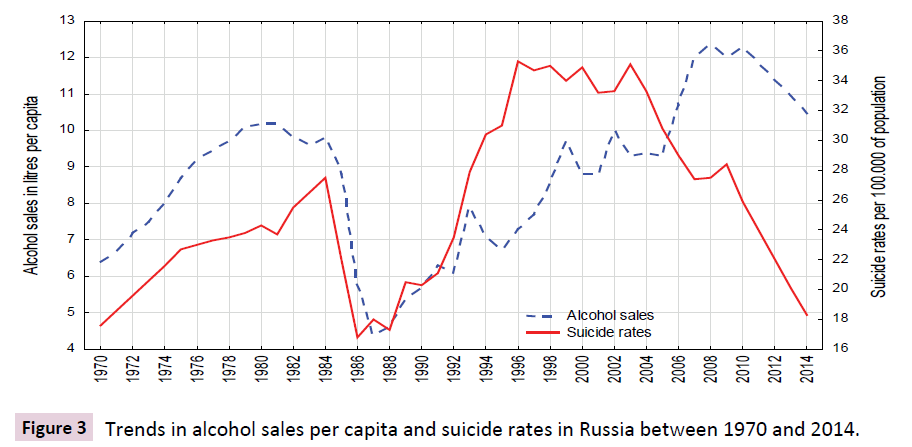
Figure 3: Trends in alcohol sales per capita and suicide rates in Russia between 1970 and 2014.
The graphical evidence suggests that in the Soviet period, the temporal pattern of suicide rates fits closely with changes in alcohol sales per capita in both countries (Figure 3). By contrast, there was significant discrepancy between these trends in the post-Soviet Russia and Belarus: decrease in suicide rates against upward trend in alcohol sales per capita between 2000 and 2007. There were sharp trends in the time series data across the study period. These trends were removed by means of a firstorder differencing procedure. The specification of the bivariate ARIMA model and outcome of the analyses are presented in Table 1. The estimates based on the first period of data suggest a strong association between alcohol sales and suicide rates in both countries, implying that a 1-l increase in per capita alcohol sales is associated with an increase in the suicide rates of 5.0% in Russia and of 6.1% in Belarus. However, the relationship between alcohol sales and suicide rates was non-significant in the last 15 years in both countries. Table 1 also shows the relative proportion of alcohol-attributable deaths to all suicide deaths by countries. The results of the analysis suggest that 55.3 % of all suicide deaths in Russia and 56.1% of all suicide deaths in Belarus could be attributed to alcohol.
| Parameter |
Model |
Estim. |
P |
AAF |
Suicides Russia
1970-1999 |
0.1.0* |
0.050 |
0.001 |
0.553 |
Suicides Russia
2000-2014 |
0.1.0 |
0.001 |
0.980 |
- |
Suicides Belarus
1970-1999 |
0.1.0 |
0.061 |
0.001 |
0.563 |
Suicides Belarus
2000-2014 |
0.1.0 |
0.001 |
0.959 |
- |
*The general form of non-seasonal ARIMA model is (p,d,q), where p - the order of the autoregressive parameter, d – the order of differencing, and q – the order of the moving average parameter. Q test for residuals are satisfactory in all models.
Table 1 Estimated effects (bivariate ARIMA model) of alcohol sales on suicide rates and alcohol-attributable suicides to all suicide deaths (AAF).
Discussion
According to the results of present analysis there was a positive and statistically significant effect of per capita alcohol sales on suicide rates in Russia and Belarus and the magnitude of this effect was similar in both countries. These results are consistent with the previous findings that highlighted close temporal association between suicide rates and population drinking [23,31]. Collectively, these findings indicate that alcohol has played an important role in the fluctuation of suicide mortality rate in the former Soviet republics during the last decades. It seems obvious that sudden decline in suicide rates between 1985-88 appears to be entirely due to Gorbachev’s anti-alcohol campaign that significantly reduced alcohol consumption by limiting its availability [34].
The collapse of the Soviet Union in 1991 was followed by socioeconomic crisis, which had devastating consequences on population physical and mental health across the region. The post-Soviet transition has had a dramatic impact on suicide mortality, which is often referred as an indicator of psychosocial distress [11]. In fact, trends in suicide mortality in the 1990s fit a typical stress related pattern: dramatic grows in the early 1990s (the acute stress) and decrease in the second half of the decade (the stage of adaptation). There is also strong evidence of a key role of alcohol in explaining of suicide mortality crisis during the post-Soviet transition [16-21]. The key point in debates on alcohol and suicide in Russia relates to the causes of increase of alcohol consumption in the early 1990s. There is evidence that alcohol is often used as medication for stress-related discomfort [35]. A prior study revealed that heavy drinking was most common among men who experienced loss in social standing during the transition [36]. This suggests that heavy drinking and psychosocial distress are closely linked since distress increase involvement in binge drinking that heightens the risk of suicide. So, collapse of Soviet Union has created psychosocial distress that increased demand for alcohol. This demand was met by factors that increased supply following the repeal of the state alcohol monopoly in January 1992 [16].
One possible explanation behind marked discrepancy in suicide trends during the post-Soviet period lies in the economic strategies that countries used. The cross-country evidence suggests that male suicide rates in the fSU are strongly related to the state of the macro economy [11]. Rapid mass privatization and increased unemployment rate was suggested as the major determinant of the mortality crisis in Russia in the early 1990s [13]. The association between macroeconomic instability, unemployment and suicides is well established [11]. A recent study in 27 European and 27 non-European countries reported an association between the magnitude of rises in unemployment and increases in suicide rates [37]. Similarly, a cross-sectional time-series analysis of a panel data from 13 countries of the former Soviet bloc between 1990 and 2008 indicated that variables measuring economic integration and regulation, such as unemployment and GDP per capita, significantly impacted on suicide rates [6].
There is, however, evidence that an increase in suicide rates during economic crisis is not inevitable. For example, the economic crisis in the former Soviet Baltic republics in 2008 has not been accompanied by an increase in suicide mortality [38]. Furthermore, in his cross-sectional study Makinen highlighted that the economic changes do not correlate significantly with changes in suicide rates in the Eastern Bloc countries [7]. Alternatively, population drinking retained its position as a predictor of suicide rates even after the socioeconomic variables were included in the model. It should be emphasized, that the magnitude of suicide mortality fluctuations during transition was similar in Russia and Belarus, despite the differences in the pace of economic reforms. This evidence suggests that rapid mass privatization, increase unemployment and psychosocial distress do not provide a sufficient explanation for cross-country differences in suicide trends during the transition to the post-communism.
A spike in suicide mortality in Russia between 1999 and 2001 might be explained by the financial crisis and a worsening economic situation in 1998. Alternatively, rise in suicide rates from 1998 may be associated with the increase in affordability of alcohol because of the drop in the price of vodka relative to those of other goods [16]. Remarkably, the 2008 global economic crisis does not seem to have had a significant impact on suicide rates in Russia.
Since 2001, Russia has experienced steep decline in suicide mortality rate. What is unclear, however, is whether this trend is simply the latest phase in a continuing cycle of fluctuations that have characterized suicide mortality in Russia over the past three decades, or whether there are new features that mark a break from the past. Several experts hypothesized that the reduction in the number of suicide deaths during the last decade might be attributed to the implementation of the alcohol policy reforms in 2006, which increased government control over the alcohol market [39,40]. In a recent study Predimore et al. [41] took advantage of this natural experiment to assess the impact on suicide mortality of a suite of Russian alcohol policies. They revealed that the alcohol policy in Russia led to a 9% reduction in male suicide mortality, meaning the policy was responsible for saving 4000 male lives annually that would otherwise have been lost to suicide.
There is, however, some doubts that recent decline in suicide rates in Russia is fully attributable to the alcohol control measures, since downward trend in suicide rate started before the implementation of the alcohol policy reforms. It might be especially true, since specific alcohol control measures were not implemented in Belarus during recent decade. An alternative explanation might be that the decline in Russian suicide mortality is simply following a regional pattern that happened to coincide with the implementation of alcohol control measures. The downward trend in the suicide mortality in the fSU countries over the past decade can be attributed to the macroeconomic stabilization.
Before concluding, we should address the potential limitations of this study. In particular, we relied on official alcohol sales data as a proxy measure for trends in alcohol consumption across the period. However, statistics on recorded alcohol consumption suffer from a high degree of uncertainty, especially in the post- Soviet period [16]. Furthermore, unrecorded consumption of alcohol was commonplace in Russia and Belarus throughout the study period, especially in the mid-1990s, when a considerable proportion of vodka came from illicit sources [42,43]. There may also have been potential problems with the suicide mortality data. In general, the quality of violent mortality statistic in countries of the former Soviet Union is sufficient for making cross-country comparisons. There was, however, sharp increase of deaths classified as injury with undetermined intent in Russia and Belarus following the collapse of the Soviet Union [44]. Substantial misclassification of suicides is likely to have distorted the time series association between population drinking and suicide rates in the post-Soviet period.
In conclusion, positive time series association between population drinking and suicide rates suggests that the dramatic mortality fluctuations in the Slavic countries of the former Soviet Union in the mid-1980s and in the first half of the 1990s were attributable to alcohol. Alternatively, alcohol cannot fully explain the downward trend in suicide mortality observed in these countries during the last decade. Similar regional pattern of suicide trends do not support the hypothesis that alcohol control policy was responsible for the decline in Russian suicide mortality during recent decade. Further monitoring of suicide mortality trends in the former Soviet countries and detailed comparisons with earlier developments in other countries remain a priority for future research.
References
- Bertolote JM & Fleishman A (2002) A global perspective in the epidemiology of suicide. Suicidology 7: 6–8.
- Razvodovsky YE (2008) A comparative analysis of dynamic of suicides in Belarus and Russia. Journal of Belarusian Psychiatric Association 14: 15-19.
- Kandrych?n SV, Razvodovsky YE (2015) The spatial regularities of violent mortality in European Russia and Belarus: ethnic and historical perspective. J Psychiatry 18: 305.
- Andreeva E, ErmakovS, Brenner H (2008)The socioeconomic etiology of suicide mortality in Russia. International Journal Environment and Sustainable Development 7: 21–48.
- Brainerd E& Cutler DM (2005) Autopsy on an Empire: Understanding mortality in Russia and the former Soviet Union. Journal of Economic Perspective 19:107–130.
- Kolves K, Milner A, Varnik P (2013) Suicide rates and socioeconomic factors in Eastern European countries after the collapse of the Soviet Union: trends between 1990 and 2008. Sociol Health Illn 35: 956–970.
- Makinen IH (2000) Eastern European transition and suicide mortality.SocSci Med 51: 1405–1420.
- Nemtsov AV (2003) Suicide and alcohol consumption in Russia, 1965-1999. Drug Alcohol Depend 1: 161–168.
- Razvodovsky YE (2013) Suicide trends in Belarus, 1980-2008. In: Pray L, Cohen C, Makinen IH, Varnik A, MacKellar FL (Eds.). Suicide in Eastern Europe, the CIS, and the Baltic Countries: Social and Public Health Determinants. Viena: Remaprint (pp. 21-28).
- Varnik A & Wasserman D (1992) Suicides in the former Soviet republics.ActaPsychiatrScand86: 76–78.
- Brainerd E (2001) Economic reform and mortality in the former Soviet Union: A study of the suicide epidemic in the 1990s. European Economic Review 45: 1007-1019.
- Stickley A, Leinsalu M, Andreew E, Razvodovsky YE, Vagero D, McKee M (2007) Alcohol poisoning in Russia and the countries in the European part of the former Soviet Union, 1970-2002. Eur J Public Health 17: 444–449.
- Stuckler D, King L, McKee M (2009) Mass privatization and post-communist mortality crisis: a cross-national analysis. Lancet 373:399-407.
- Earle JS, Gehlbach S (2010) Mass privatization and the post-communist mortality crisis, is there a relationship? Upjohn Institute Working Paper No 10: 162.
- Razvodovsky YE (2014) Alcohol and Suicide in Eastern Europe. J Addict Med TherSci 1: 101.
- Nemtsov AV &Razvodovsky YE (2008) Alcohol situation in Russia, 1980-2005. Social and Clinical Psychiatry 2:52–60.
- Pridemore WA (2006)Heavy drinking and suicide in Russia. Soc Forces 85: 413–430.
- Razvodovsky YE (2009) Alcohol and suicide in Belarus. PsychiatriaDanubina 21: 290–296.
- Razvodovsky YE (2010) Blood alcohol concentration in suicide victims. European Psychiatry 25:1374.
- Razvodovsky YE (2011) Alcohol consumption and suicide rates in Russia. Suicidology Online 2: 67–74.
- Razvodovsky YE (2014) The effects of alcohol on suicide rate in Russia. J Socialomics 3: 112.
- Pridemore WA (2013)The impact of hazardous drinking on suicide among working-age Russian males: an individual-level analysis. Addiction 108: 1933–1941.
- Landberg J (2008) Alcohol and suicide in Eastern Europe. Drug Alcohol Rev 27: 361–373.
- Razvodovsky YE (2001)The association between the level of alcohol consumption per capita and suicide rate: results of time-series analysis. Alcoholism 2: 35–43.
- Razvodovsky YE (2007) Suicide and alcohol psychoses in Belarus 1970-2005. Crisis 28: 61-66.
- Razvodovsky YE (2009) Beverage-specific alcohol sale and suicide in Russia. Crisis 30: 186–191.
- Razvodovsky YE (2009)Suicide and fatal alcohol poisoning in Russia, 1956-2005. Drugs: Education, Prevention and Policy 16: 127–139.
- Razvodovsky YE (2012) Alcohol and suicide in Belarus. Saarbruken: LAP LAMBERT Academic Publishing.
- Razvodovsky YE (2006) Alcohol consumption and suicide rate in Belarus. PsychiatriaDanubina 18: 64.
- Razvodovsky YE Kandrych?n SV (2014)Spatial regularity in suicides and alcohol psychoses in Belarus. ActaMedicaLituanica 21: 57–64.
- Stickley A, Jukkala T, Norstrom T (2011) Alcohol and suicide in Russia, 1870-1894 and 1956-2005: evidence for the continuation of a harmful drinking culture across time? J Stud Alcohol Drugs 72: 341–347.
- Norstrom T & Skog OJ (2001) Alcohol and mortality: methodological and analytical issue in aggregate analysis. Addiction 96:5–17.
- Box GEP& Jenkins GM (1976) Time Series Analysis: forecasting and control. London. Holden-Day Inc.
- Stickley A, Razvodovsky Y, McKee M (2009) Alcohol and mortality in Russia: A historical perspective. Public Health 23: 20–26.
- Koposov RA, Ruchkin VV, Eeisemann M, Sidorov PI (2002) Alcohol use in adolescents from northern Russia: the role of social context. Alcohol & Alcoholism 37: 297–303.
- Yukkala T, Mäkinen IH, Kislitsyna O, Ferlander S (2008) Economic strain, social relations, gender, and binge drinking in Moscow. SocSci Med 66: 663–674.
- Chang SS, Stuckler D, Yip P, Gunnell D (2013) Impact of 2008 global economic crisis on suicide: time trend study in 54 countries. BMJ 347: f5239.
- StankunasM, Linder J, Avery M,Sorensen R (2013) Suicide, recession, and Unemployment. The Lancet 381: 721.
- Schkolnicov VM, Andreev EM, McKee M, Leon DA (2013) Components and possible determinants of the decrease in Russian mortality in 2004–2010. Demographic Research 28:917–950.
- Razvodovsky YE (2014)Was the mortality decline in Russia attributable to alcohol control policy? Journal of Sociolomics 3:2.
- Pridemore WA, Chamlin MB, Andreev E (2013) Reduction in male suicide mortality following the 2006 Russian alcohol policy: an interrupted time series analysis. Am J Public Health 103: 2021–2026.
- Razvodovsky YE (2013) Estimation of the level of alcohol consumption in Russia. ICAP Periodic Review Drinking and Culture 8: 6–10.
- Razvodovsky YE (2008)Noncommercial alcohol in central and eastern Europe, ICAP Review 3. In: International Center for Alcohol Policies, ed. Noncommercial alcohol in three regions. Washington, DC: ICAP:17–23.
- Varnic P, Sisask M, Varnik A, Yuryev A, Kolves K, et al. (2010) Massive increase in injury deaths of undermined intent in ex-USSR Baltic and Slavic countries: hidden suicides? Scand J Public Health 38: 395-403.

