Keywords
Suicide; Mental illness; Psychiatry; Psychopathology; Schizophrenia
Introduction
Suicidal behaviours are thoughts or tendencies that put a person at higher risk of committing suicide. Suicide is an act of intentionally terminating one’s own life. Suicidal behaviors are classified into three categories; suicidal ideation, suicide plan or intent and suicide attempts.[1-3] Data from World Health Organization indicated that approximately one million people worldwide die by suicide each year. This corresponds to one death every 40 s by suicide. Suicide attempts and suicidal ideation are far more common. The number of suicide attempts exceeds by 20 times the number of deaths by suicide.[3] According to WHO estimates for the year 2020, approximately 1.53 million people will die by suicide and 10 to 20 times more people will attempt suicide worldwide. These estimates represent on average one death every 20 s and one attempt every one to two seconds.[3-5] According to World Health Organization (WHO) and the Latest Burden of Disease Estimation, suicide is a major public health problem in high-income countries and is an emerging problem in low and middle-income countries where poor psychiatric services are available.[3,6] The global suicide rate as a whole is estimated to be 11.6 per 100,000 inhabitants per year. Suicide accounts for 1.4% of total mortality and 15% of injury mortality.[7]
Suicide rates have increased by 60% over the last 50 years and the increase has been particularly marked in developing countries.4 As a group people with a mental illness face statistically higher risk of suicide. Although it is generally accepted that 10% of people with mental illness commit suicide during their life time and approximately 90 percent of suicide cases meet criteria for psychiatric disorders, particularly major depression, substance use disorders, cluster B personality disorders and schizophrenia, most of them can be either extended or are even preventable.[8,9]
Although many researches showed suicide and suicidal behaviours are more common in high income countries, it is also increasing currently in low and middile income countries beacuase of various reasons.[10] Suicide and suicidal behaviours are higher in those who are divorced/separated/widowed,[11] being female, younger, single and less educated.[3,12-14] Complete suicide is more common in males where as nonfatal suicidal behaviours are more common among females.[3,15] Having family history of psychopathology are more suicidal compared with those not having family history of psychopathology.[16] The presence of mental disorders in general and co-morbidity in particular, are consistently reported as strong predictors of suicidal behaviors.[8,9,13,17-25] Among mental disorders, major depressive disorder is the strogest predictors of suicide and suicidal behaviours.[8,24,26-28] Other mental disorders like schizophrenia,[8,9,19,25,29,30] bipolar disorders[29,31] and anxiety disorders[26,32] are risk factors for suicidal behaviours. Substance use disorders and substance co-morbidity are also the predictors of suicide and suicidal behaviours.[8,9,17,18] From substance use disorders; alcohol use disorders,[25,29,33,34] tobacco and other illicit drug use[22] and cigarette smoking[35] are the predictors of suicide and suicidal behaviours.
Among few studies conducted in Ethiopia, a review of police and hospital records from Addis Ababa, the rate of completed suicide was found to be 7.76/100,000 persons per year.[36] The lifetime prevalence of suicidal ideation and attempted suicide was 64.8% and 19.2% among psychiatric out-patients at Gondar hospital psychiatry clinic,37 2.7% and 0.9% for an urban community in Addis Ababa,[38] respectively. Attempted suicide was 3.2% for a rural adult population in Butajira Ethiopia[39] and in 10 year cohort study among severe mental disorders in Butajira; 26.3% for major depression, 23.8% for bipolar I disorders, 13.1% for schizophrenia and the ratio of suicide attempters to suicide completed was 10.3:1.[40] Family history of sucicide was 3%.[41] There are notable differences in the type of disorder most strongly predictive of suicidal behaviors. However, more is needed to clearly understand the extent and risk factors of suicidal behaviors in many countries around the world, particularly in low and low middile income countries like Ethiopia.[42] Despite the public and health system costs of suicide and suicidal behaviors, there are a paucity of data about suicidal behaviours among people with mental illness in our country especially in Jimma university teaching hospital psychiatry clinic. The aim of this study was therefore to assess the extent, magnitude, means and predictors of suicidal behaviors among people with mental illness attending treatment as at JUTH psychiatry clinic from October 26 to November 24/ 2014.
Methods and Materials
Study area and period
Jimma University teaching hospital (JUTH) is found in Jimma town, Oromia regional state, south west Ethiopia. It is 352 km south west of Addis Ababa, the capital city of Ethiopia. The department of psychiatry under JUTH was established in 1988 next to Amanuel specialized mental hospital in the country. Currently there are about 5405 follow up outpatients and the clinic officially has 26 beds for inpatient services.[43] The study was conducted from October 26 to November 24/2014.
Study design
Facility based cross-sectional study design was employed.
Population
Source population: All people with mental illness attending treatment at JUTH psychiatry clinic were considered as a source population.
Study population: All sampled people with mental illness attending treatment at JUTH psychiatry clinic were considered as a study population.
Inclusion and exclusion criteria
Inclusion criteria: All adult people with mental illness who were attending the outpatient treatment at JUTH psychiatry clinic during data collection period were included in the study.
Exclusion criteria: Severely ill and those having cognitive, communicating and hearing problems were excluded.
Sample size determination and sampling procedures
Sample size determination: The sample size was determined by using single population formula assuming the prevalence of suicidal ideation and attempt among psychiatry outpatients was 64.8% and 19.2% respectively at a study done in University of Gondar specialized hospital, North West Ethiopia28 with 5% marginal of error, 95% confidence level of certainty and alpha 0.05. Based on this the actual sample size was determined by taking 64.8% for large sample size using single population proportion formula. New patients who come were included so correction formula was not necessary because the total population (N) was unpredictable. Adding 10% for non-response rate, therefore the total sample size was 385.
Sampling technique and procedures: All patients coming to JUTH psychiatry clinic during data collection period were included in the study by using consecutive sampling technique until the required sample size was achieved.
Study variables
Dependent variables: Status of suicidal behaviours.
Independent variables: Socio-demographic and economic variables like age, sex, marital status, religion, ethnicity, income, educational status and employment status were collected using a structured questionnaire. Mental illness and psychosocial related variables; like type of diagnosis, duration of mental illness, having family history of mental illness, suicide attempt, social support and living conditions were collected. Substance related informations were collected for alcohol, khat, cigarette and other substances (Cannabis/hashish/marijuana/ganja, Shisha).
Data collection procedures and instruments
Instruments: The initially developed structured questionnaire in English language was translated into Amharic and Afan Oromo and back to English by independent person to check for consistency and understandability of the tool. The questionnaire had six subsections; (i) Socio-demography, (ii) Mental health related, (iii) Means of suicidal attempts, (iv) Substance related, (v) Questions related to suicidal behaviours and (vi) social support. For alcohol use disorders CAGE was used which had scored of 0-4 and cutoff point ≥ 2 with sensitivity 0.71 and specificity 0.9044 and for nicotine dependence Fagerstrom Test was used which had four yes/no items scored no (0)/yes (1) and two multiple choose items scored 0 to 3 total scored of 0-10 and cutoff point ≥ 5 with sensitivity and specificity 0.75 and 0.80, respectively. The Oslo 3-items social support scale was used to measure the strength of social support. The scores range from 3-14. This scale has been used in several studies, confirming the feasibility and predictive validity with respect to psychological distress. A score ranging between 3 and 8 is classified as poor support, a score between 9 and 11 as moderate support, and a score between 12 and 14 as strong support. The Suicidal Behaviours Questionnaire revised (SBQ-R) is a self-report measure of suicidal behaviours. This shortened version of the SBQ consists of four questions and used a Likert type scale to assess suicidal behaviour history, current suicide status and self-appraisal and expectancies about the future likelihood of engaging in suicidal behavior. Specific items include: “Have you ever thought about or attempted to kill yourself?” (Rated 1-4); “How often have you thought about killing yourself in the past year?” (Rated 1-5); “Have you ever told someone that you were going to commit suicide, or that you might do it?” (Rated 1-3); “How likely is it that you will attempt suicide some day?” (Rated 0-6). A broad range of information is obtained in a very brief administration and has the sensitivity 80%, specificity 91% with a score of 3-18 and cutoff point ≥ 8 for adult clinical population. The other questionnaires are developed by the investigator from different literatures.
Data collection method: The data was collected by a face to face interview done for all people with mental illness at the JUTH psychiatric clinic outpatient by five BSC psychiatry nurses. For those data collectors and the supervisor one day training was given mainly focused on the process of data collection methods, tools and how to handle ethical issues of the participants’ were discussed.
Data quality assurance: Pre-test was conducted on 5% of the sample size before the actual study. Regular supervision, control as well as support were given to the data collectors by the supervisor and principal investigator. The collected data was properly reviewed and checked for completeness and consistency by the supervisor and principal investigator daily. Incomplete and unclear questionnaires were returned to the data collectors to get it corrected. The collected data was coded, edited, entered into Epidata version 3.1 in order to minimize error that occurs during data entry. Then, the data exported to SPSS version 20.
Data processing and analysis: The data were edited, cleaned and analyzed using statistical package for social sciences (SPSS version 20). Descriptive statistics; means, frequency, percentages and standard deviations were generated. To determine an association between dependent and independent variables adjusted odds ratio was used using logistic regression and p-value <0.05 at 95% CI was declared statistically significant.
Ethical considerations
Ethical approval was taken from the Ethical review board of Jimma University College of Health Sciences. Written informed consent was obtained from the study participants. Participant’s confidentiality was insured and their identity was not displayed. The data was used only for the purpose of this research. Those who were actively suicidal during the period of data collection were referred to the outpatient department and were managed accordingly.
Results
Socio-demographic and economic characteristics
A total of 385 patients were invited and fully participated in the study providing a response rate of 100%. Majority (72.2%) of the patients were males. The mean age and standard deviation of the patients was 32 year (± 9.83 years); with a minimum and maximum age value of 18 and 70 years, respectively. Two hundred fifteen (55.8%) and 142 (36.9%) of the patients were single and married respectively. Most of the patients 235 (61.0%) were Muslim by religion followed by 110 (28.6%) Orthodox Christian. With regard to ethnicity, majority of patients 276 (71.7%) were Oromo followed by Amhara 48 (12.5%) (Table 1).
| Variables |
Category |
Numbers |
Percent |
| Sex |
Males |
278 |
72.2 |
| Females |
107 |
27.8 |
| Age |
18-27 |
142 |
36.9 |
| 28-37 |
152 |
39.4 |
| 38-47 |
55 |
14.3 |
| ≥ 48 |
36 |
9.4 |
| Marital status |
Single |
215 |
55.8 |
| Married |
142 |
36.9 |
| Divorced/ separate/widowed |
28 |
7.3 |
| Religion |
Muslim |
235 |
61.0 |
| Orthodox |
110 |
28.6 |
| Protestant |
36 |
9.4 |
| OthersR |
4 |
1.0 |
| Ethnicity |
Oromo |
276 |
71.7 |
| Amhara |
48 |
12.5 |
| Gurage |
20 |
5.2 |
| Dawuro |
12 |
3.1 |
| OthersE |
29 |
7.5 |
| Educational status |
Illiterate |
120 |
31.2 |
| Primary school (1-8) |
93 |
24.2 |
| Secondary /high school (9-12) |
97 |
25.2 |
| Tertiary (12+) |
75 |
19.5 |
| Occupation |
Unemployed |
97 |
25.2 |
| Employed |
83 |
21.6 |
| Farmer |
56 |
14.5 |
| Student |
44 |
11.4 |
| Merchant |
34 |
8.8 |
| House wife |
33 |
8.6 |
| Daily labor |
22 |
5.7 |
| OthersO |
16 |
4.2 |
| Living condition |
Alone |
18 |
4.7 |
| With family |
349 |
90.6 |
| OthersL |
18 |
4.7 |
OthersL includes (those living other than parents, wife/husband and children). OthersR include (catholic and Jehovah witness religion). OthersE includes (Yem, Tigre, Silte, kefa, Wolayta, Benchi maji ethnic groups). OthersO includes (retire, house servant, preacher)
Table 1: Socio-demographic characteristics of people with mental illness attending treatment at JUTH psychiatry clinic, south west Ethiopia 2014 (n=385).
Ninety seven (25.2%) of the patients were unemployed while 83 (21.6%) of the patients were full time employee. About 120 (31.2%) patients were illiterate, 93 (24.2%) and 97 (25.2%) of the patients had completed primary and secondary school education respectively. The mean monthly family income and standard deviation was 1475.50 Ethiopian birr (± 1432.70 Ethiopian birr); with minimum and maximum value of 50 and 10,000 Ethiopian birr respectively. Majority of patients 349 (90.6%) were living with their family (Table 1).
Mental illness and social support related characterstics
Form the total respondents, 137 (35.6%) and 113 (29.4%) were diagnosed to have schizophrenia and major depressive disorders respectively. About 156 (40.5%) of patients had insidious (within 3-12 months) mode of illness onset while 111 (28.8%) of patients had acute (within 3 months) mode of illness onset. Majority of patients 289 (75.1%) had chronic course (≥ 2 years durations) followed by 69 (17.9%) patients had sub acute (three months to two years) durations. About 152 (39.5%) of patients had history of admission. Larger proportions of patients 356 (92.5%) had two or more follow up treatment while the rest 29 (7.5%) had only a single visit and treatment. Of the total patients only 55 (14.3%) of them had family history of mental illness. Regarding social support 137 (35.6%), 158 (41.0%) and 90 (23.4%) of patients had poor, moderate and strong social support respectively (Table 2).
| Variables |
Category |
Number |
Percent |
| Diagnosis |
Schizophrenia |
137 |
35.6 |
| Major depressive disorders |
113 |
29.4 |
| Bipolar disorders |
67 |
17.4 |
| OthersP psychotic disorders |
31 |
8.1 |
| Substance induced psychiatry disorders |
12 |
3.1 |
| Anxiety disorders |
11 |
2.9 |
| OtherD psychiatry disorders |
14 |
3.6 |
| Mode of illness onset |
Abrupt (within hours/days) |
59 |
15.3 |
| Acute (<3 months) |
111 |
28.8 |
| Insidious 3-12 months |
156 |
40.5 |
| Insidious ≥ 12 months |
59 |
15.3 |
Duration of
Illness |
Acute <3 months |
27 |
7.0 |
| Sub-acute 3months-2 years |
69 |
17.9 |
| Chronic ≥ 2 years |
289 |
75.1 |
| Family history mental illness |
No |
330 |
85.7 |
| Yes |
55 |
14.3 |
OthersD includes (somatoform, psychiatry disorders due to medical conditions, dysthymia, unspecified disorders, other mood disorders, dissociative disorders, adjustment disorders and personality disorders) OthersP includes (brief psychotic, schiaffective, schizophreniform and delusional disorders)
Table 2: Mental health related characteristics of people with mental illness attending treatment at JUTH psychiatry clinic, south west Ethiopia 2014 (n=385).
Magnitudes, extent and pattern of suicidal behaviors
The reliability of Suicidal Behaviors Questionnaire-Revised (SBQ-R) was calculated and found to have cronbach’s α=0.79. The prevalence of over all suicidal behaviors (as defined by SBQ-R a total score ≥ 8) was 28.6% (24.1%-33.1%) (Figure 1). The lifetime prevalence of suicidal ideation, intent and attempts with their confidence intervals were 21.8% (17.7%-25.9%), 16.9% (13.2%-20.6%) and 16.1% (12.4%-19.8%), respectively. The life time all suicidal ideation was 211 (54.8%). Number of suicide attempts ranges from 1-3 and only 8 (2.1%) of patients had more than one attempt. The prevalence of suicidal ideation in the past one year (12 months) was 115 (29.9%) (25.3%- 34.5%). Out of those 63 (54.8%) had once and 34 (29.6%) had twice suicidal ideation at two different point in time. Hundred nine (28.3%) patients had threat of suicide attempt or they told to other people as they were going to commit suicide. out of those 87 (79.8%) once and 22 (20.2%) more than once told to others. The likelihood of suicidal behavior in the future was reported only by 3 (0.8%) patients. Family history of attempted and completed suicide were 12 (3.1%) and 7 (1.8%), respectively (Table 3). Nearly half of the patients 174 (45.2%) never reported suicidal ideation, intent or attempt.
Figure 1: Lifetime prevalence of suicidal behaviors among people with mental illness attending treatment at JUTH psychiatry clinic, south west Ethiopia 2014.
| Variables |
Category |
Number |
Percent |
| Life time suicidal ideation, intent and/or attempts |
Never |
174 |
45.2 |
| Suicidal ideation |
84 |
21.8 |
| Intent |
65 |
16.9 |
| Suicide attempts |
62 |
16.1 |
| Life time all suicidal ideation |
211 |
54.8 |
| Frequency of suicidal ideation in the past one year |
Never |
270 |
70.1 |
| Once |
63 |
16.4 |
| Twice |
34 |
8.8 |
| 3-4 times |
14 |
3.6 |
| Always (≥ 5 times) |
4 |
1.0 |
| |
One year all suicidal ideation |
115 |
29.9 |
| Suicidal threats |
Once |
87 |
79.8 |
| Twice and more |
22 |
20.2 |
| Likely hood of suicide in the future |
Never |
260 |
67.5 |
| No chance at all |
64 |
16.6 |
| Rather unlikely |
46 |
11.9 |
| Unlikely |
12 |
3.1 |
| Likely |
3 |
0.8 |
| Frequency of suicide attempts |
Once |
54 |
87.1 |
| Twice and more |
8 |
12.9 |
Table 3: Magnitude of suicidal behaviors among people with mental illness attending treatment at JUTH psychiatry clinic, south west Ethiopia 2014 (number=385).
Places and methods of suicide attempt
Among 62 suicide attempters 47 (75.8%) were attempted at home. The most frequent means/methods used for suicide attempt were hanging in 28 (45.2%) followed by poison 11 (17.2%) and drug/medication overdose 10 (16.1%) (Figure 2). The involvement of family members aborted 38 (61.3%) of patients who were attempting suicide. Out of those who attempted suicide, 24 (38.7%) felt angry during the interview (Table 4).
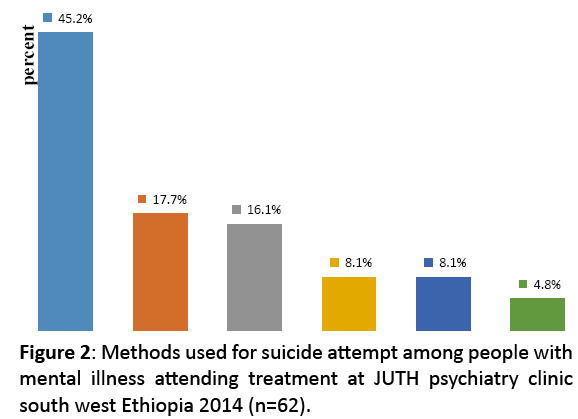
Figure 2: Methods used for suicide attempt among people with mental illness attending treatment at JUTH psychiatry clinic south west Ethiopia 2014 (n=62).
| Variables |
Category |
Number |
Percent |
Places of suicide attempts |
Home |
47 |
75.8 |
| Forest |
6 |
9.7 |
| Field |
4 |
6.5 |
| River |
3 |
4.8 |
| School |
2 |
3.2 |
| Abort of suicide attempt |
Family |
38 |
61.3 |
| Friends |
10 |
16.1 |
| God |
8 |
12.9 |
| Health profession |
3 |
4.8 |
| OthersS |
3 |
4.8 |
| Feeling after suicide attempt |
Felt angry |
24 |
38.7 |
| Felt guilty |
21 |
33.9 |
| Felt nothing |
17 |
27.4 |
Table 4: Details of patients who attempted suicide among people with mental illness who attending treatment at JUTH psychiatry clinic, 2014 (numbers=62).
Independent predictors of suicidal behaviors
In bivariate logistic regression analyses age, marital status, religion, ethnicity, education status, occupation, living condition, social support, diagnosis, having family history of mental illness, having family history of suicide attempt, mode of illness onset, duration of illness, frequency of hospital visit, alcohol use disorders, nicotine dependence, khat chewing and other substance use were become candidates for multiple logistic regression analysis at p-value <0.25. Sex is clinically important variable for the study and was added to the multivariate analysis. There is no any co-linearity among candidate variables because of tolerances above 0.1 and variance inflation factor below 10 for each candidate variable. The Hosmer and Lemeshow statistic has chi-square value of 7.306 and a significance of 0.504 which means that Hosmer and Lemeshow test is not statistically significant and therefore the model has a good fit. Because p-value exceeds level of significance (α=0.05), that shows, there is no significant difference between the observed and predicted model values and hence the model fits the data well.
Finally in the multivariate logistic regression analysi age category 18-27 and 28-37, presence of family history of mental illness, having duration of illness between 3 months to 2 years, major depressive disorders and presence of psychiatric diagnosis (like anxiety, psychiatry disorders due to medical illness, somatoform disorders, dysthemia, personality disorders and adjustment disorder) as a group, alcohol use disorder and nicotine dependence were independent predictors of suicidal behavior at p-value of <0.05 (Table 5).
| Variables |
Category |
Suicidal behaviors |
AOR (95% CI) |
P-value |
| Yes N (%) |
No N (%) |
| Age |
18-27 |
49 (34.5) |
93 (65.5) |
4.53 (1.37-14.93) |
0.01* |
| 28-37 |
46 (30.3) |
106 (69.7) |
3.25 (1.01-10.41) |
0.04* |
| 38-47 |
10 (18.2) |
45 (81.8) |
1.87 (0.48-7.28) |
0.37 |
| ≥ 48 |
5 (32.6) |
31 (86.1) |
Reference |
|
| Family history of mental illness |
Yes |
25 (45.5) |
30 (54.5) |
2.25 (1.11-4.57) |
0.03* |
| No |
85 (25.8) |
245 (74.2) |
Reference |
|
| Duration of illness |
Acute (<3 months) |
6 (22.2) |
21 (77.8) |
0.55 (0.19-1.61) |
0.27 |
| Sub-acute (3 months to 2 years) |
24 (34.8) |
45 (65.2) |
1.95 (1.02-3.74) |
0.04* |
| Chronic (≥ 2 years) |
80 (27.7) |
209 (72.3) |
Reference |
|
| Diagnoses |
Major depressive disorder |
41 (36.3) |
72 (63.7) |
4.48 (1.95-10.26) |
0.00* |
| Bipolar disorders |
13 (19.4) |
54 (80.6) |
Reference |
|
| Schizophrenia |
35 (25.5) |
102 (74.5) |
1.93 (0.81-4.61) |
0.14 |
| OthersP psychotic disorders |
9 (29.0) |
22 (70.1) |
1.39 (0.45-4.29) |
0.57 |
| Substance induced psychiatry disorders |
5 (41.7) |
7 (58.3) |
2.97 (0.61-12.67) |
0.18 |
| Other psychiatry disordersD |
7 (28.0) |
18 (72.0) |
3.84 (1.16-12.67) |
0.03* |
| Alcohol use behavior |
Not drink at all |
68 (23.1) |
227 (76.9) |
Reference |
|
| Non-alcohol use disorders |
13 (38.2) |
21 (61.8) |
1.30 (0.53-3.16) |
0.58 |
| Alcohol use disorders |
29 (51.8) |
27 (48.2) |
2.29 (1.08-4.85) |
0.03* |
Smoking
Behaviors |
Not smoke at all |
62 (24.1) |
195 (75.9) |
Reference |
|
| Non dependence |
13 (26.5) |
36 (73.5) |
1.31 (0.57-3.03) |
0.53 |
| Dependence |
35 (44.3) |
44 (55.7) |
2.21 (1.08-4.53) |
0.03* |
Table 5: Multiple logistic regression analysis of factors associated with suicidal behaviors among people with mental illness attending treatment at JUTH psychiatry clinic, 2014.
Patients whose age group were 18-27 and 28-37 were 4.5 times and 3.3 times more likely to develop suicidal behaviors as compared to patients whose age group was ≥ 48 with (AOR=4.53, 95% CI: 1.37-14.93) and (AOR=3.25, 95% CI: 1.01-10.41), respectively. Patients who had family history of mental illness were 2.3 times more likely to develop suicidal behaviors as compared to patients who had no family history of mental illness with (AOR=2.25, 95% CI: 1.11-4.57).
Patients with durations of mental illness between three months and two years were 2 times more likely to develop suicidal behaviors as compared to chronically ill (≥ 2 years) with (AOR=1.95, 95% CI: 1.02, 3.74). Patients with the diagnoses of major depressive disorders and with the diagnosis other psychiatry diagnoses (like anxiety, psychiatry disorders due to medical illness, somatoform disorders, dysthemia, personality disorders and adjustment disorder) as a group were 4.5 times and 3.8 times more likely to develop suicidal behaviors as compared to patients with diagnosis of bipolar disorders with (AOR=4.48, 95% CI: 1.95-10.26) and (AOR=3.84, 95% CI: 1.16-12.67), respectively. Patients who had alcohol use disorder and nicotine dependence were 2.3 times and 2.2 times more likely to develop suicidal behaviors as compared to non alcohol users and non smokers with (AOR=2.29. 95% CI: 1.08-4.85) and (AOR=2.21, 95% CI: 1.08-4.53), respectively (Table 5).
In the final model gender, religion, educational status, marital status, occupation, living condition, social support, numbers of hospital visit, family history of suicide attempt, khat chewing and other substance use (like shisha, hashish, cannabis, marijuana) were not associated with suicidal behaviors (Table 5).
Discussion
In this study the life time prevalence and predictors of suicidal behaviors were assessed. The methods and places of suicide attempt as well as supports for aborted suicidal attempt were also assessed. Generally it was found that the prevalence of suicidal behaviours was 28.6% (24.1%-33.1%). The lifetime prevalence of suicidal ideation, intent and attempts were 21.8% (17.7%-25.9%), 16.9% (13.2%-20.6%) and 16.1% (12.4%-19.8%), respectively. The prevalence of suicidal ideation in the past one year (12 months) was 115 (29.9%) (25.3%-34.5%). The independent predictors of suicidal behaviors were; major depressive disorders, other mental disorders (like anxiety, psychiatry disorders due to medical illness, somatoform disorders, dysthemia, personality disorders and adjustment disorder) as a group, age of 18-27 and 28-37, having family history of mental illness, Gurage ethnicity group, nicotine dependence, alcohol use disorders and having sub acute (3 months to 2 years) durations of mental illness.
The prevalence of suicide attempt in this study is consistent with a study done in Gondar hospital psychiatry outpatients (19.2%) but the suicidal ideation is lower than the study done in Gondar hospital psychiatry outpatients (64.8%). This might be due to that the SBQ-R used in this study could not assess how many of patients had suicidal ideation before attempting suicide. The instrument SBQ-R also assessed minor suicidal thought and intent separately. The investigator in Gondar hospital developed a structured questionnaire which enables to assess how many of suicide attempters had made suicidal ideations before attempting suicide.[39]
The lifetime prevalence of suicidal ideation and suicidal attempts in this study are higher than a community based study among adult population of Addis Ababa (the capital city of Ethiopia) that reported that the lifetime suicidal ideation and suicidal attempt 2.7% and 0.9%, respectively.[40] The lifetime suicide attempt was also higher than the lifetime suicidal attempt in a study conducted at Butajira (Southern Ethiopia) among general adult population which was 3.2%.[41] This is for the ovious fact that our study was conducted in a hospital sample of people living with mental illness in contrary to the above mentioned community based studies in Addis Ababa and Butajira Ethiopia. There are evidences that showed people living with mental illness are at higher risk of suicidal ideation and attempt compared to the general population.[8,15,16,24-30,32]
The lifetime prevalence of suicidal ideation, intent and suicide attempts in this study is lower than a national survey conducted in South Africa among adults who have a prior history of DSM IV diagnosied disorder of whom 61%, 64% and 70.3% of the patients reported suicidal ideation, plan and attempt respectively.[26] This discrepancy might be due to the reason that this study was conducted only among follow up patients who might have a controlled suicidal behavior as the result of the treatment. In addition to this, the instrument used and socio cultural difference of the study populations might contribute for the discripancy. However, the lifetime prevalence of suicidal ideation, intent and attempt in this study are higher than stress and health survey conducted in South African, where the lifetime prevalence rates of suicidal ideations, suicide intent and suicide attempts were 9.1%, 3.8% and 2.9%, respectively.[16] This might be again due to the fact that our study samples were people living with mental illness who are high risk populations as compared to a community survey conducted in South Africa.
But, the lifetime prevalence of suicidal behaviors and suicide attempt of this study are lower than a study conducted in Finland among bipolar patients. This also might be due to the fact that, patient with bipolar illness will have higher rate of suicidal behavior during the depressive episodes. This study also identified that depression as independent predictor for higher suicidal behavior. The prevalence of suicidal behaviors was 80% and suicide attempt was 51%.[31] And also lifetime prevalence of suicidal ideation and suicide attempt are lower than a study conducted in USA California among psychiatry outpatients who reported suicidal ideation and attempt of 55% and 25%, respectively.[24] This discrepancy might be due to that suicide also more common in western societies.[3,10,12,13,17] In this study majority of suicide attempt were occurred at home. The most common method used for suicide attempt reported was hanging followed by poisoning and drug/medication overdose. So this is important for prevention of access by educating family and arranging medication for patients with higher risk. Family involvement was the easily available and most common support made to abort attempted suicide. This is consistent with studies in other parts of the country.[29,39-41] The medication overdose is incomparable with other studies in other parts of Ethiopia. This might be due to the reason that this study is conducted among follow up outpatients who were taking medications.
In this study, patients being in the age group of 18-27 and 28-37 were significant predictors of suicidal behaviors. This is comparable with the finding of various studies in different settings.[3,11,35,40] It is known that late adolescent and younger adulthood is a developmental stage with much struggle to support self, psychological conflict between rejecting families ideaology influenced by peer pressure and being confused to get out to their own self identity which could inducing a lot of distress to their life that could contribute for higher rate of suicidal behavior.[30] In this study having a diagnosis of major depressive disorder was significantly associated with suicidal behaviors which are consistent with a study conducted in Butajira Ethiopia, among people with severe mental illness,[29] from a study done in South Africa[26] and from a study conducted in high income countries. Suicidal ideation was markedly prevalent in depressed patients and depression was found to be a precondition for suicide attempt as investigated by various studies.[8,27,28]
In addition to Major depressive disorder, other mental illnesses (like anxiety, psychiatry disorders due to medical illness, somatoform disorders, dysthemia, personality disorders and adjustment disorder) as a group were significantly associated with suicidal behaviors. This is incomparable with studies conducted in other parts of Ethiopia. This might be due to the reason that other studies conducted at community setting among people with no psychiatric illness while the rest studies were done among people with severe mental illness (MDD, bipolar and schizophrenia) only who might not be concerned for psychopathologies like anxiety, somatoform and somatic symptoms. But this is comparable with study done in high income countries.[23,26,28,32]
In this study having family history of mental disorders was significantly associated with higher rate of suicidal behaviors, which is incomparable to a study done at Gondar hospital psychiatry out patients.[39] However it is consistent with the finding from stress and health survey conducted in South Africa.[16] In our study duration of mental illness between 3 months and 2 years were significantly associated with suicidal behaviors which might be due to the effect of follow up treatment and patient’s psychological readjustment out of their experience living with the illness.This finding however is comparable with a study conducted in Butajira, Ethiopia which reported that there was a decrease of suicidal behavior among patient with schizophrenia as the duration of illness increases.[29] These warrants further study to explore out the relatishinship of suicidal behavior and duration of illness including factors explaining the scenario.
Alcohol use disorders had significant association with suicidal behaviors in our study which is comparable with a study conducted in Butajira, Ethiopia among people with severe mental illness[29] and with a study done among depressed inpatients in Malaysia.[33] It was also comparable with a study done among people with substance use disorders in USA California.[36] In addition to alcohol use disorders; nicotine dependence had significant association with suicidal behaviors. This is comparable with a study conducted in Iran among psychiatry inpatients about the association of smoking and suicide.[37] And also comparable with a study about suicidal thoughts and suicidal behaviors in Australia among adults: finding from national survey of mental health and well-being.[22]
This study has some strength as compared to other studies: 1. it used standard instruments than traditional way to assess suicidal behaviors 2. Substance co morbidities like alcohol use disorders, nicotine dependence, Khat use/abuse as well as social support were assessed extensively as it should be. Despite providing valuable baseline data, there are also some limitations encountered: 1. Social desirability bias as the data was collected by a face to face interviewer administered approach. So the respondents might reply in favorable of others that are either over reporting or under reporting. 2. Recall bias; there might be forgetfulness and there was not cross check about the information they gave us. 3. In this study only adult psychiatry patients were included, so it is difficult to generalize all psychiatry patients because children and adolescents psychiatry patients are not included in the study. The instrument SBQ-R and Fagerstrom Test were not used in developing countries before.
Conclusion
This study showed that the prevalence of suicidal behaviors is very high. Most of suicide attempts occur at home. The methods used for suicide attempt (hanging self, poisoning and drug/medication overdose) were preventable. The involvement of family members, were the main reasons for the aborted case of attempted suicide. Major depressive disorders and presence of other comorbid psychiatric disorders, alcohol use disorders, nicotine dependence, having family history of mental illness, being at younger age, and sub acute duration of illness were the independent predictors of suicidal behaviors. A routine screening and management of suicidal behaviors giving consideration for patient at younger age, patient with sub acute duration of illness, patient with depressive disorders, patient with co morbid substance use problems, patient with family history of mental illness shall be a very crucial element of the health care system practice. Since family involvement is a predictor for aborted suicidal attempt, educating and empowering family members in identifying and referring suicidal behaviors will be in favor of increasing access for emergency psychiatric management.
Acknowledgement
First and for most we would like to thank Jimma University College of Health Sciences for funding this research project and department of psychiatry for arranging this opportunity to carry out this study. We would also like to thank the participants for their volunteered participation.
Author’s Contributions
ES involved from the inception to design, acquisition of data, analysis and interpretation, drafting and editing the manuscript, LD involved in the inception to design, analysis and interpretation and revises and edits the manuscript for the final submission. MA involved in the inception to design, analysis and interpretation and revises and edits the manuscript for the final submission. All authors read and approved the final manuscript.
References
- Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, et al. Suicide and suicidal behavior. Epidemiologic Reviews 2008; 30: 133-154.
- Kessler RC, Nock MK. Prevalence of and risk factors for suicide attempts versus suicide gestures: Analysis of the national comorbidity survey. J Abnorm Psychol 2006; 115: 616-623.
- Gvion Y, Apter A. Suicide and suicidal behavior. Puplic health reviews 2012; 34: 1-12.
- World Health Organization (WHO) Statement for world suicide prevention day on 8 September 2008. International Association for Suicide prevention 2008.
- Bertolote JM, Fleischmann A. A global perspective in the epidemiology of suicide. Suicidologi 2002; 2: 6-8.
- World Health Organization (WHO). International association for suicide prevention. World suicide prevention day 2013.
- Värnik P. Suicide in the world. Int J Environ Res Public Health 2012; 9: 760-771.
- World Health Organization (WHO). International association for suicide prevention. World suicide prevention day 2012.
- Benedetto S, World Health Organization (WHO). Preventing mental disorders 2006.
- World Health Organization (WHO). Mental illness and suicide. Global perspective 2009.
- Nock MK, Hwang I, Sampson N, Kessler RC, Angermeyer M, et al. Cross-National analysis of the associations among mental disorders and suicidal behavior: Findings from the WHO world mental health surveys. PLoS Med 2009; 6: 6-14.
- Centers for Disease Control (CDC) and prevention. Surveillance for violent deaths; National violent death reporting system in United State from 16 States, 2008. Surveillance Summaries 60: 1-49.
- Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. The British Journal of Psychiatry 2008; 192: 98-105.
- Fleming TM, Merry SN, Robinson EM, Denny SJ, Watson PD. Self-reported suicide attempts and associated risk and protective factors among secondary school students in New Zealand; Australian and New Zealand. Journal of Psychiatry 2007; 41: 213-221.
- Larry Culpeper. Recognizing suicide risk factors in primary and psychiatric care. Medscape Psychiatry and Mental Health 2010.
- Atwoli L, Nock M, Williams DR, Stein DJ. Association between parental psychopathology and suicidal behavior among adult offspring: Results from the cross-sectional South African stress and health survey. BMC Psychiatry 2014; 14: 65
- Karaman D, Durukan I. Suicide in children and adolescents. Current Approaches in Psychiatry 2013; 5: 30-47.
- Mofidi N. Studies on mental health in Kurdistan – Iran: Umeå Sweden 2009; 22-36.
- Hocaoglu C, Tekin ZB. Suicidal ideation in patients with schizophrenia. Isr J Psychiatry Relat Sci 2009; 46: 195-203.
- Nock MK, Greif JG, Hwang I, McLaughlin KA, Kessler RC, et al. Prevalence, correlates and treatment of lifetime suicidal behavior among adolescent’s results from the national comorbidity survey replication adolescent supplement. JAMA Psychiatry 2013; 3-5.
- Nock MK, Hwang I, Sampson NA, Kessler RC. Mental disorders, comorbidity and suicidal behavior: Results from the National Comorbidity Survey Replication. Molecular Psychiatry 2010; 15: 868-876.
- Johnston AK, Pirkis JE, Burgess PM. Suicidal thoughts and behaviours among Australian adults: Findings from the 2007 National survey of mental health and wellbeing; Australian and New Zealand. Journal of Psychiatry 2009; 43: 635-643.
- Mekonnen D, Kebede Y. The prevalence of suicidal ideation and attempts among individuals attending an adult psychiatry out-patient clinic in Gondar, Ethiopia. African Health Sciences 2011; 11: 103-107.
- Asnis GM, Friedman TA, Sanderson WC, Kaplan ML, van Praag HM, et al. Suicidal behaviors in adult psychiatric outpatients. Am J Psychiatry 1993; 150: 108-112.
- Cicek H, Babuc TZ. Suicidal ideation in patients with schizophrenia. Isr J Psychiatry Relat Sci 2009; 4: 195-203.
- Khasakhala L, Sorsdahl KR, Harder VS, Williams DR. Lifetime mental disorders and suicidal behaviour in South Africa. Afr J Psychiatry (Johannesbg) 2011; 14: 134-139.
- Campos RC, Mesquita C. Testing a model of suicidality in community adolescents: A brief report. J Child Adolesc Behav 2014; 2:147.
- Oquendo M, Brent DA, Birmaher B, Greenhill L, Kolko D, et al. Post-traumatic stress disorder, major depression and the risk for suicidal behavior. Am J Psychiatry 2005; 162: 560-566.
- Shibre T, Hanlon C, Medhin G, Alem A, Kebede D, Teferra S, et al. Suicide and suicide attempts in people with severe mental disorders in Butajira, Ethiopia: 10 year follow-up of a population-based cohort. BMC Psychiatry 2014; 14: 150.
- Sadock BJ, Sadock VA. Kaplan & Sadock's synopsis of psychiatry. Behavioral Sciences/Clinical Psychiatry (10th Edition) Lippincott Williams & Wilkins, New York 2007; 280.
- Valtonen H, Suominen K, Mantere O, Arvilommi P, Esometsa ET, et al. Suicidal ideation and attempts in bipolar I and II disorders. J Clin Psychiatry 2005; 66: 1456-1462.
- O’Neill S, Ferry F, Murphy S, Corry C, Bolton D, et al. Patterns of suicidal ideation and behavior in Northern Ireland and associations with conflict related trauma. PLoS ONE 2014; 9: e91532.
- Fong CL, Shah SA, Maniam T. Predictors of suicidal ideation among depressed inpatients in a Malaysian sample. Suicidology Online 2012; 3: 33-41.
- Suokas JT, Perälä J, Suominen K, Saarni S, Lönnqvist J, et al. Epidemiology of suicide attempts among persons with psychotic disorder in the general population Schizophrenia. Research 2010; 124: 22-28.
- Conwetl Y, Duberstein P. Suicide in older adults: Determinants of risk and opportunities for prevention. Prevention and treatment of suicidal behavior: From science to practice 2005.
- Tiet QQ, Ilgen MA, Byrnes HF, Moos RH. Suicide attempts among substance use disorder patients: An initial step toward a decision tree for suicide management. Alcohol Clin Exp Res 2006 30: 998-1005.
- Hooman S, Zahra H, Mitra S, Mohammad FH, Mohammad MR. Association between cigarette smoking and suicide in psychiatric inpatients. Tobacco Induced Diseases 2013; 11: 5.
- Bekry AA. Trends in suicide, parasuicide and accidental poisoning in Addis Ababa, Ethiopia. Ethiop J Health Dev1999; 13: 247-261.
- Mekonnen D, Kebede Y. The prevalence of suicidal ideation and attempts among individuals attending an adult psychiatry out-patient clinic in Gondar, Ethiopia. African Health Sciences 2011; 11: 103-107.
- Kebede D, Alem A. Suicide attempts and ideation among adults in Addis Ababa, Ethiopia. Acta Psychiatrica Scand 1999; 100: 35-39.
- Alem A, Kebede D, Jacobsson L, Kullgren G. Suicide attempts among adults in Butajira, Ethiopia. Acta Psychiatr Scand Suppl 1999; 397: 70-76.
- Mikami I, Akechi T, Kugaya A, Okuyama T, Nakano T, et al. Screening for nicotine dependence among smoking-related cancer patients. J Cancer Res 1999; 90: 1071-1075.
- Dalgard S, Dowrick C, Lehtinen V. Negative life events, social support and gender difference in depression. A multinational community survey with data from the ODIN study. Soc Psychiatry Psychiatr Epidemiol 2006; 41: 444-451.
- Osman A, Bagge CL, Cuttlerrez PM, Konick LC, Kooper BA, et al. The suicidal behaviors questionnaire-revised (SBQ-R): Validation with clinical and nonclinical samples. Assessment 2001; 8: 443-453.

