Keywords
Hypoglycemia; Islets of Langerhans Transplantation; Pancreatitis, Acute Necrotizing
INTRODUCTION
Total pancreatectomy is associated with significant morbidity, involving both exocrine and endocrine dysfunction. In contrast to the gradual and isolated loss of beta cells as a result of autoimmune attack in type 1 diabetes [1], diabetes after total pancreatectomy is due to acute loss of beta cells, but also the loss of glucagon-producing alpha cells. Glucagon is a key counter-regulatory hormone providing protection from hypoglycemia [2]. Consequently, post-pancreatectomy diabetes is associated with a high frequency of hypoglycemia and the need for complex insulin regimens [3].
Islet auto-transplantation after total pancreatectomy (for non-malignant disease) has been performed since the 1970s with good success. Insulin independence is achieved in about a third of cases, and persistent long-term graft function with the continued production of C-peptide is observed in the majority of patients [4, 5].
More recently, whole pancreas allotransplants after total pancreatectomy have been reported to restore both endocrine and exocrine function, with ensuing improvement in the quality of life [6, 7].
To date, islet allotransplantation has been restricted to subjects with type 1 diabetes complicated by severe hypoglycemia and/or glycemic lability and has shown increasing success since the advent of the Edmonton protocol [8]. Insulin independence can often be achieved, albeit with two islet infusions in many cases. Long-term insulin independence can be maintained for a variable duration of time, depending on multiple patient and donor factors [9] and requires adequate control of both allo- and auto-immunity. Most importantly, islet transplantation results in stable (and good) glycemic control with elimination of severe hypoglycemia even in subjects returning to use some insulin, as long as some graft function persists [10].
We herein report the first case (to the best of our knowledge) of islet allotransplantation for brittle diabetes following total pancreatectomy.
CASE REPORT
Our patient was a 56-year-old man at the time of first presentation. In May 2005, he developed acute necrotizing pancreatitis with pancreatic abscess due to a gallstone causing occlusion of the common bile duct. He developed generalized peritonitis, septic shock and multi-organ failure, necessitating surgical intervention. Intra-operatively, he was found to have a large pancreatic abscess and extensive necrosis involving the entire pancreas and underwent near total pancreatectomy. He was started on insulin and pancreatic exocrine supplements (pancrelipase, Creon®, Abbot, IL, USA) post-operatively. In July 2005 (2 months following pancreatectomy), he was found to have some residual pancreatic endocrine function, as indicated by the persistent presence of C-peptide production (Figure 1).
Figure 1. Graft function indicated by stimulated C-peptide:
glucose ratio (dashed lines and open squares) at the end of a
mixed meal tolerance test and HbA1c (solid line and filled
circles) before and after islet transplantation. The grey line
indicates HbA1c of 6.5% which is the threshold for diagnosis of
diabetes.
Over the following year, he had increasing insulin requirements and, in spite of an intensive multiple daily insulin injection regimen using detemir (Levemir®, Novo Nordisk, Missisauga, ON, Canada) and aspart (Novorapid®, Novo Nordisk, Missisauga, ON, Canada), he was having daily episodes of hypoglycemia, requiring third party assistance and had experienced several episodes of severe hypoglycemia requiring the intramuscular administration of glucagon. He developed severe hypoglycemia unawareness, and had no symptoms (either autonomic or neuroglycopenic) of hypoglycemia at all. At the time of evaluation at our centre in September 2006, he was using an average of 60 units of insulin/day, had severe hypoglycemia and mild glycemic lability (HYPO score and lability index are shown in Figure 2 [11]). C-peptide production had declined since 2005 just above the lower level of detection (0.1 ng/mL) (Figure 1).
Figure 2. HYPO score and lability index (LI) before and after islet
transplantation. HYPO score is indicated by solid line and filled
circles. LI by dashed lines and open squares. The solid grey line
indicates a HYPO score of 1,047 which is the threshold for severe
hypoglycemia [11] and the dotted grey line indicates a lability
index of 433 which is the threshold for severe lability [11].
There was no family history of diabetes, and no history of any autoimmune disease. Autoantibodies (mIAA, GAD65, ICA512) were all negative. He had no other significant medical history of note nor any history of alcohol excess, and did not have diabetes prior to pancreatectomy. Prior to transplant liver imaging (ultrasound) and biochemistry were normal.
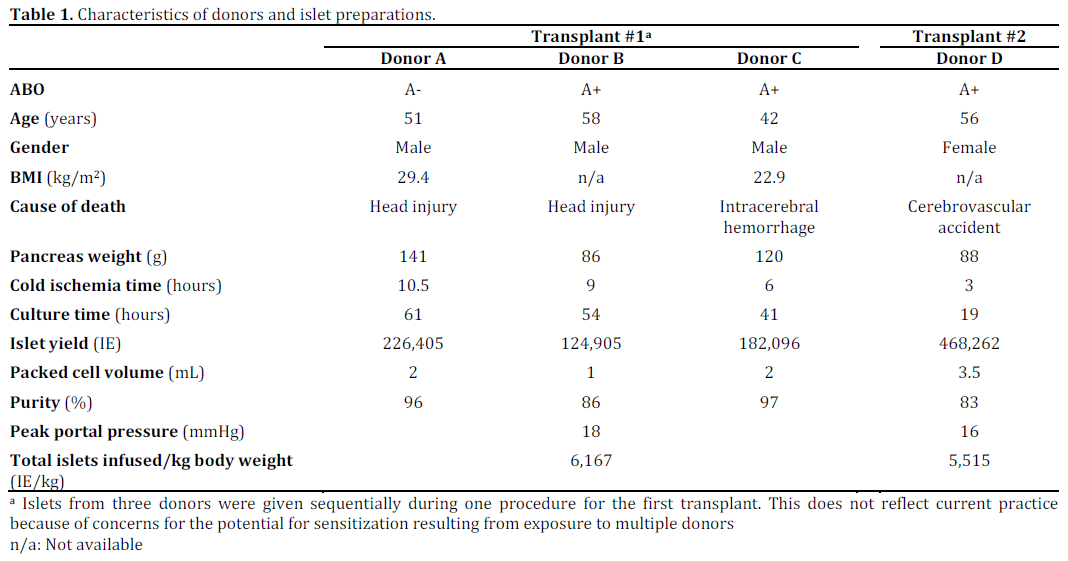
He underwent islet allotransplantation on January 9th, 2007, receiving islets isolated from three organ donors (Table 1) for a total of 6,167 IE/kg. For immunosuppression, he was given intravenous thymoglobulin (6 mg/kg) with etanercept, and maintained on tacrolimus (trough target level of 10 ng/mL for first 3 months and 8-10 ng/mL thereafter) and mycophenolate mofetil (1 g twice daily). Insulin requirement was halved to 25- 30 units/day following islet allotransplantation, with excellent glycemic control and more importantly, severe hypoglycemia was eliminated. Figure 1 shows HYPO score and lability index prior to and following islet allotransplantation.
Mild hypoglycemia was uncommon (less than once a week) and could be easily self-treated. At 6 months following islet allotransplantation, he reported restoration of hypoglycemia awareness, with symptoms of tremors and hunger occurring during one episode of hypoglycemia when the capillary blood glucose was 3.4 mmol/L.
He underwent a second alloislet infusion on November 11th, 2008, receiving 5,515 IE/kg isolated from a single donor (Table 1). He received daclizumab for induction, and continued on maintenance immunosuppression with tacrolimus and mycophenolate mofetil. One month after the second islet infusion, he was successfully weaned off insulin and remains so more than 4 years later, with excellent glycemic control (HbA1c 6.1%) and no hypoglycemia.
Graft function, as assessed during serial mixed meal tolerance tests, has remained stable to date (Figure 2), as has glycemic control reflected by HbA1c.
Transplant-Related Complications
The patient tolerated both islet transplant procedures well, with no peri-procedural complications. He has tolerated immunosuppressive therapy well, and has had no severe adverse events. There has not been any evidence of sensitization post-transplant based on annual measurements of panel reactive antibodies by flow cytometry (class I: 16±5%; class II: 0%).
Diabetes Complications
He continues to have no clinical or biochemical evidence of diabetic retinopathy, nephropathy or neuropathy.
DISCUSSION
This case illustrates that alloislet transplantation can be a feasible option for the treatment of brittle diabetes frequently seen after total pancreatectomy. Alloislet transplant has the advantages over whole pancreas transplant of being a minimally invasive procedure, with mild/no periprocedural complications and short length of hospital stay [9, 10] although both require long term immunosuppression. Islet transplantation does not restore exocrine function, but exogenous pancreatic enzyme supplements were effective and easily managed by this patient.
Although this patient required two islet infusions to become insulin independent, a single islet infusion was sufficient to reduce hypoglycemia at the same time as improving glycemic control. He remains insulin independent for more than four years with robust and stable metabolic function of the islet graft.
It is not wise to draw conclusions on the basis of a single case, but the robust function of his islet grafts is striking given that four year insulin independence rates among type 1 recipients of the same era was only 30% [12]. The absence of autoimmunity in our case should be advantageous for long term function since recurrent autoimmunity has been documented after whole pancreas transplant and the absence of autoantibodies is advantageous in islet transplantation [13, 14]. Our case also illustrates some other potential advantages over typical islet allotransplant recipients who generally have longstanding, autoimmune type 1 diabetes. The short diabetes duration in our case provides an opportunity for primary prevention of microvascular complications. The maintenance of adequate immunosuppression may be easier and better tolerated in the absence of gastroparesis or other co-morbidities associated with longstanding poor diabetes control.
In contrast to autoislet transplantation, alloislet transplantation requires long-term immunosuppressive therapy. However, current immunosuppressive regimens for islet transplantation are generally well tolerated [15], as was the case here. Although graft function has remained stable to date in this subject, it remains possible that graft function may deteriorate over time, contributed at least in part by the need for long-term immunosuppressive therapy with potentially diabetogenic agents [16].
Pancreatectomy is usually performed because of the presence of a pancreatic tumour. Clearly autoislet transplantation would not be considered in cases of malignancy. Furthermore there would be concerns of recurrent malignancy if such patients received immunosuppression which would be required for islet allotransplantation. Islet allotransplant might be considered if a patient were considered cured (i.e., no evidence of recurrence after 5 years) if there were significant difficulties with diabetes control.
In subjects undergoing total/near total pancreatectomy for benign pancreatic disease, including chronic, painful pancreatitis, autoislet transplantation would be preferred. There are several situations where autoislet transplantation may not be possible, even for non-malignant disease. For example, cases with extensive pancreatic necrosis (as in this case), severe pancreatic trauma, or where there is concern or evidence of pancreatic sepsis (because of a risk for hepatic abscesses). In cases of suspected malignancy, histological examination of the pancreas may confirm a non-malignant disease (e.g., autoimmune pancreatitis) but after allotransplantation would be possible. Thus in selected cases with major difficulties with diabetes control, after appropriate assessment and informed consent, alloislet transplantation could be considered as an alternative.
Conflicts of interest
The authors have no potential conflict of interest
References
- Weir G, Bonner-Weir S. Five Stages of Evolving Beta-CellDysfunction During Progression to Diabetes. Diabetes2004;53(suppl_3):S16–21. PubMed 15561905
- Cryer PE. Mechanisms of hypoglycemia-associatedautonomic failure and its component syndromes in diabetes.Diabetes 2005;54(12):3592–601. PubMed 16306382
- Parsaik AK, Murad MH, Sathananthan A, et al. Metabolic andtarget organ outcomes after total pancreatectomy: Mayo Clinicexperience and meta-analysis of the literature. Clinicalendocrinology 2010;73(6):723–31. PubMed 20681992
- Sutherland DER, Gruessner AC, Carlson AM, et al. Isletautotransplant outcomes after total pancreatectomy: a contrastto islet allograft outcomes. Transplantation 2008;86(12):1799–802. PubMed 19104425
- Webb MA, Illouz SC, Pollard CA, et al. Islet autotransplantation following total pancreatectomy: a long-termassessment of graft function. Pancreas 2008;37(3):282–7.PubMed 18815550
- Gruessner RWG, Sutherland DER, Dunn DL, et al. Transplantoptions for patients undergoing total pancreatectomy for chronicpancreatitis. J Am Coll Surg 2004;198(4):559–67–discussion568–9. PubMed 15051008
- Gruessner RWG, Sutherland DER, Drangstveit MB,Kandaswamy R, Gruessner AC. Pancreas allotransplants inpatients with a previous total pancreatectomy for chronicpancreatitis. J Am Coll Surg 2008;206(3):458–65. PubMed18308216
- Shapiro, Shapiro AM, Lakey JR, et al. Islet transplantation inseven patients with type 1 diabetes mellitus using aglucocorticoid-free immunosuppressive regimen. N Engl J Med2000;343(4):230–8. PubMed 10911004
- Ryan EA, Paty BW, Senior PA, et al. Five-year follow-up afterclinical islet transplantation. Diabetes 2005;54(7):2060–9.PubMed 15983207
- Alejandro R, Barton FB, Hering BJ, Wease S, CollaborativeIslet Transplant Registry Investigators. 2008 Update from theCollaborative Islet Transplant Registry. Transplantation2008;86(12):1783–8. PubMed 19104422
- Ryan EA, Shandro T, Green K, et al. Assessment of theseverity of hypoglycemia and glycemic lability in type 1 diabeticsubjects undergoing islet transplantation. Diabetes2004;53(4):955–62. PubMed 15047610
- Barton FB, Rickels MR, Alejandro R, et al. Improvement inOutcomes of Clinical Islet Transplantation: 1999–2010. DiabetesCare 2012;35:1436–45. PMC3379615
- Burke GW, Vendrame F, Pileggi A, Ciancio G, Reijonen H,Pugliese A. Recurrence of autoimmunity following pancreastransplantation. Curr Diab Rep 2011;11(5):413–9. PubMed21660419
- Jaeger C, Brendel MD, Hering BJ, Eckhard M, Bretzel RG.Progressive islet graft failure occurs significantly earlier inautoantibody-positive than in autoantibody-negative IDDMrecipients of intrahepatic islet allografts. Diabetes1997;46(11):1907–10. PubMed 9356046
- Koh A, Imes S, Ryan E, Shapiro AJ, Senior PA. ImprovedTolerability of Tacrolimus plus Mycophenolate Mofetil withoutGraft Compromise in Islet Transplantation. Diabetes2008;57(Supp 1):1952–P.
- Johnson JD, Ao Z, Ao P, et al. Different effects of FK506,rapamycin, and mycophenolate mofetil on glucose-stimulatedinsulin release and apoptosis in human islets. Cell Transplant2009; 18(8):833–45. PubMed 19500470



