Andre Luiz De Souza1 and Muhammad Wasif Saif2
1Metrowest Medical Center and 2Department of Hematology/Oncology,
Tufts Medical Center. Boston, MA, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Hematology/Oncology Department Tufts Medical Center
800 Washington Street Box 245Boston, MA 02111USA
Phone +1-617.636.5627
Fax +1-617.636.8535
E-mail wsaif@tuftsmedicalcenter.org
Received August 29th, 2014 - Accepted September 05th, 2014
Keywords
Carcinoma; Case Reports; Neoplasms, Squamous Cell; Pancreas
Abbreviations
5-FU: 5-fluorouracil CEA: carcinoembryonic antigen CK: cytokeratin c-kit: cellular kinase receptor DFS: disease free survival HMB-45: human melanoma black monoclonal antibody 45 S-100: soluble 100% in saturated ammonium sulfate solution SMA: alpha smooth muscle actin SUV: standardized uptake values (for PET/CT scan)
Dear Sir,
We previously published our and Johns Hopkins data titled: "Platinum-based therapy in adenosquamous pancreatic cancer: experience at two institutions” [1]. We will here like to submit a related case report as a letter to the editor to JOP in reference to the above paper.
Squamous cell carcinoma of the pancreas has various reported incidence rates, ranging from 0.5% to as high as 5% of pancreatic ductal carcinomas [2, 3]. Of the 1300 cases of pancreatic cancers observed at autopsy in a survey in Japan in 1992, 0.7% were squamous cell carcinoma [4]. A Mayo clinic review of very rare exocrine tumors showed an even rarer incidence of squamous cell carcinoma when compared to acinar and small cell carcinoma of the pancreas [5]. This discrepancy in the reported incidence rates related to the fact that some of the cases represent adenosquamous carcinoma rather than pure squamous cell carcinoma of pancreas. In an analysis of 25 patients, mean age at diagnosis of pancreatic squamous cell carcinoma was 62 years (range: 33–80 years) and there was no gender difference [6]. There is no study about the molecular profile of squamous carcinoma of the pancreas. There are no retrospective or prospective studies about the best therapy for these tumors.
We describe here one case of a patient with squamous cell carcinoma of the pancreas. A 61-year-old male presented with anorexia and 15 pounds weight loss to his primary care physician in November 2011. He developed mild right upper back and stomach pain and was sent to abdominal ultrasound that revealed a large gastrohepatic mass. An urgent CT of the abdomen confirmed a perigastric mass arising from the pancreas and encroaching the liver. PET-CT of the mass revealed a SUV of 19.1. Tumor markers (beta-HCG, alpha-fetoprotein, CEA, CA 19-9) were unremarkable. Complete blood count showed mild normocytic normochromic anemia and liver function tests were within normal limits. Tumor cells were strongly positive for pancytokeratin P63, CK 5/6, while negative for c-kit, vimentin, HMB-45, S-100 SMA, chromogranin and synaptophysin, supporting a morphologic diagnosis of squamous cell carcinoma. He was diagnosed with stage IV squamous cell carcinoma of the pancreas. He was initially treated with gemcitabine 1000 mg/m2 and cisplatin 50 mg/m2 every 14 days. He had stable disease for 4 months with restaging CT scans performed every 8 weeks. His major toxicities on this regimen included grade 3 nausea, grade 2 vomiting and grade 2 dehydration. He continued to be treated with single agent gemcitabine, while cisplatin was omitted from the regimen due to worsening nausea despite maximum use of antiemetics. He progressed after 8 weeks of the end of gemcitabine. He subsequently received 5-FU and leucovorin as second-line therapy that produced stable disease for an additional 3 months but treatment was terminated due to worsening performance status. The patient expired approximately 26 days later.
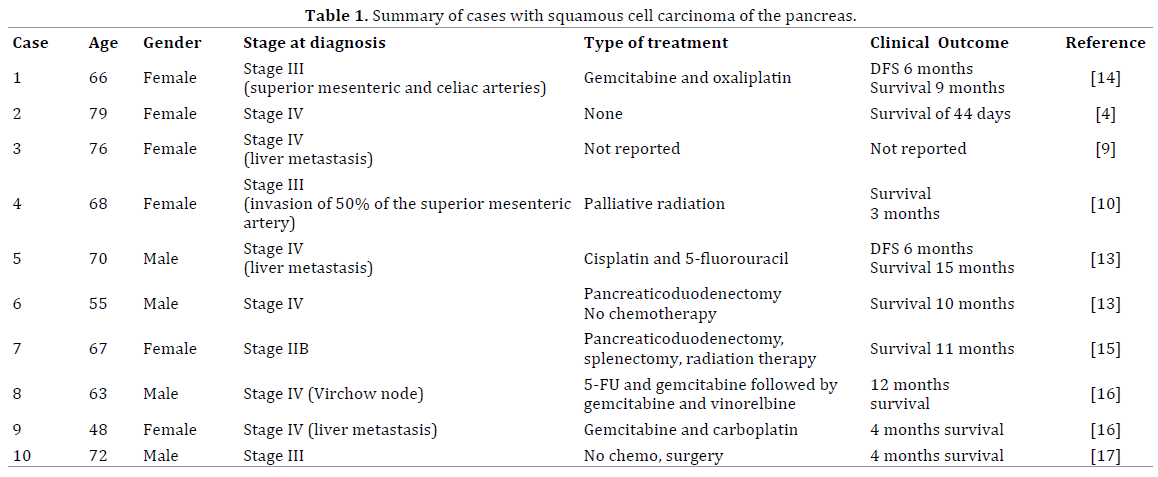
The clinical presentation of squamous cell carcinoma of pancreas does not differ from pancreatic ductal adenocarcinoma, but case reports document presence of hypercalcemia independent of bone metastasis or primary hyperparathyrodism [7]. Table 1 summarizes data on few cases and case series with available data. Metastatic squamous cell carcinoma of the pancreas is much more common as a cause of pancreatic squamous cell carcinoma lesions than the primary squamous cell carcinoma, with the most common primary tumor been the lungs [8]. Primary pancreatic squamous cell carcinoma is such a rare event that the finding of pure squamous cell carcinoma on pancreatic carcinoma biopsy warrants an extensive workup to rule out the possibility of other more common primary sources, including head-and-neck, lung, and esophagus [8]. Endoscopic ultrasound-guided fine needle aspiration has been used for diagnosis of squamous cell carcinoma of the pancreas [9,10]. Minami et al. also reported an elevated level of squamous cell carcinoma antigen (14.9 U/mL) upon diagnosis, which immediately declined to within normal limits after complete resection of the tumor [11]. In a review of 25 cases, median overall survival was 7 months for patients who underwent curative resection and 3 months for patients who did not undergo curative resection [10]. The longest survival reported for squamous cell carcinoma of the pancreas was 15 months, after treatment with cisplatin and 5-fluorouracil [12].
Squamous cell carcinoma is a rare type of pancreatic cancer that requires not only histologic confirmation but also confirmation of its origin, as most of them is known to be metastatic lesions from other primary tumors. The clinical and biologic profile of squamous cell carcinomas is similar to pancreatic ductal adenocarcinoma, with a variable prognosis from the published case reports. It is important to recognize that most squamous carcinomas in the pancreas will be distant metastasis from lung, esophageal and head and neck tumors. Squamous cell carcinoma antigen may be a good predictor of chemotherapy as it disappears after complete resection of the tumor. We describe here a case report of a patient who was initially treated with a platinum-based therapy with gemcitabine maintenance, and posteriorly started on second-line fluoropyrimidine therapy. Although there is scarcity of data of clinical outcomes in squamous cell carcinoma of the pancreas, a 3-month stable disease outcome in our article suggests a role of fluoropyrimidines as second-line chemotherapy for these tumors in addition to platinumbased therapy as first-line option. Taxanes may also be beneficial in this setting and needs to be investigated.
Conflict of interest
The authors have no potential conflict of interest
References
- De Souza AL, Saif MW. Platinum-based therapy in adenosquamous pancreatic cancer: experience at two institutions 2014; 15: 144-146. [PMID: 24618440]
- Sears HF, Kim Y, Strawitz J. Squamous cell carcinoma of the pancreas. J SurgOncol. 1980; 14: 261–265. [PMID: 7392648]
- Baylor SM, Berg JW. Cross-classification and survival characteristics of 5,000 cases of cancer of the pancreas. J SurgOncol. 1973; 5: 335–358.
- Nakashima H, Hayakawa T, Hoshino M, Kamiya Y, Ohara H, Yamada T, Mizuno K, Inagaki T, Nakazawa T, Yamada H, et al. Squamous cell carcinoma of the pancreas with massive invasion of the retroperitoneum. Intern Med. 1995; 34: 61-64. [PMID: 7718985]
- Mansfield A, Tafur A, Smithedajkul P, Corsini M, Quevedo F, Miller R. Mayo Clinic experience with very rare exocrine pancreatic neoplasms. Pancreas. 2010; 39: 972-975. [PMID: 20622706]
- Layfield LJ, Cramer H, Madden J, Gopez EV, Liu K. Atypical squamous epithelium in cytologic specimens from the pancreas: cytological differential diagnosis and clinical implications. DiagnCytopathol. 2001; 25: 38–42. [PMID: 11466811]
- Brayko CM, Doll DC. Squamous cell carcinoma of the pancreas associated with hypercalcemia. Gastroenterology. 1982; 83: 1297 – 1299. [PMID: 7129033]
- Itani KM, Karni A, Green L. Squamous cell carcinoma of the pancreas. J Gastrointest Surg. 1999; 3: 512-515. [PMID: 10482708]
- Lai LH, Romagnuol J, Adams, Yang J. Primary squamous cell carcinoma of pancreas diagnosed by EUS-FNA: a case report. World J Gastroenterol. 2009; 15: 4343–4345. [PMID: 19750582]
- Zacharia G, Levine J, Winstead NS, Antillon MR, Davis NK. Primary squamous cell carcinoma of the pancreas diagnosed by endoscopic ultrasound-guided fine needle aspiration. J Gastrointestin Liver Dis. 2012; 21: 321-323. [PMID: 23012676]
- Minami T, Fukui K, Morita Y, et al. A case of squamous cell carcinoma of the pancreas with an initial symptom of tarry stool. J GastroenterolHepatol. 2001; 16:1077–1079. [PMID: 11595080]
- Kodavatiganti R, Campbell F, Hashmi A, Gollins SW. Primary squamous cell carcinoma of the pancreas: a case report and review of the literature. J Med Case Rep. 2012; 6: 295. [PMID: 22973995]
- Qiang-pu C, Kun O, Qing-hai G, Fan Z. Squamous cell carcinoma of the pancreas with liver metastasis: a case report. Chinese Medical Journal 2008;121: 853-854 [PMID: 18701054]
- Nikfam S, Sotoudehmanesh R, Pourshams A, Sadeghipour A, Sotoudeh M, Mohamadnejad M. Squamous cell carcinoma of the pancreas. Arch Iran Med. 2013; 16: 369-370. [PMID: 23725072]. Adachi K. Primary squamous cell carcinoma of the pancreas: a case report. JOP. 2011; 12: 181-184. [PMID: 21386649]
- Soto Iglesias S, Baltar Arias R, Vázquez Rodríguez S, Alvarez M, Gómez Martínez P, Alvarez Sánchez MV, Vázquez Astray E. [Virchow's node as the form of onset of squamous cell carcinoma of the pancreas]. GastroenterolHepatol. 2009 Dec; 32(10):693-696. [PMID: 19748706]
- Shehri A, Silverman S, King KM. Squamous cell carcinoma of the pancreas. CurrOncol. 2008; 15: 293-297. [PMID: 19079631]
- Anagnostopoulos GK, Aithal GP, Ragunath K, Kaye P, Rowlands BJ. Squamous cell carcinoma of the pancreas: report of a case and review of the literature. JOP. 2006 11; 7: 47-50. [PMID: 16407618]

