Keywords
Leiomyosarcoma; Splenic Vein; Thrombosis
INTRODUCTION
Leiomyosarcoma (LMS) is a malignant smooth muscle tumor, most commonly found in the abdominal compartment or in the limbs. Two percent of LMSs affect the blood vessels wall and veins are involved five times more frequently than arteries. Inferior vena cava LMS accounts for roughly 0.5% of all adult soft tissue sarcomas and 75% of all primary venous LMSs [1, 2].
Splenic vein LMS is extremely rare, with only three cases reported in the literature [3-6]. In this article we briefly review the literature on the subject and we report a case of splenic vein LMS, the first treated with local excision and direct re-anastomosis of the splenic vein stumps.
CASE REPORT
A fifty eight year old woman was admitted to our Department for dull epigastric and left hypocondrium pain, with no other associated symptoms. She had no history of diabetes, previous cancer, pancreatic disease and alcohol or tobacco addiction. Her physical examination and blood tests were normal. An abdominal ultrasound scan was performed and found to be normal except for a 2-cm hypoechoic lesion identified along the posterior margin of the pancreatic body. A chest-abdomen CT scan was then performed, confirming a 15 mm mainly hypodense lesion along the posterior margin of the pancreatic body (Figure 1). The lesion was in close contact with the splenic vessels, which were patent with no sign of thrombosis. No lymphadenopathy or distant metastatic deposit was detected. Alpha-fetoprotein, carcinoembryonic antigen, carbohydrate antigen 19.9 and chromogranin A were normal. The differential diagnosis included metastasis, pancreatic adenocarcinoma, endocrine tumor, extraintestinal gastro-intestinal stromal tumor, Schwannoma, inflammatory myofibroblastic tumor and fibrous solitary tumor of the pancreas.
Figure 1. Computed tomography showing a 15-mm lesion along the
posterior margin of the pancreas body, in strict contact with the splenic
vessels. The lesion is hypodense in the arterial phase (A) and presents a
peripheral contrast-enhancement during the late venous phase (B).
A whitish, solid, well-capsulated 15 mm lesion arising from the splenic vein wall, behind the posterior margin of the pancreas, was observed (Figure 2). The lesion showed a rather stiff consistency with a non-infiltrating pattern and was easily dissected from the surrounding adipose and pancreatic tissue. The splenic vein was controlled and clamped on both sides of the lesion which was excised with a tract of the splenic vein. The continuity of the splenic vein was then restored by a direct end-to-end anastomosis between the two splenic vein stumps. The intraoperative histopathological examination was consistent with a stromal lesion with no clear sign of malignant transformation and the resection margins were therefore no further extended. The complete histopathological examination demonstrated a likely primary tumor of the splenic vein, characterized by bundles of spindle cells arranged in a dense fibrous stroma (Figures 3ab), with a strong positive immunohistochemistry staining for smoothmuscle actin (Figure 3c) and a focal positive staining for DOG1. Immunohistochemistry staining for S100, CD117, CD31 and pan-cytokeratin was negative. These findings were consistent with a grade 1 primary leio8myosarcoma of the splenic vein, according to the FNCLCC classification [7, 8]. The proliferation index calculated using Ki-67 was 20% (Figure 3D) and the mitotic index was 5/10 HPF. The radial and venous (proximal and distal) resection margins were free from tumor infiltration and the excision was complete.
Figure 2. Intraoperative snapshot. The deep-located lesion is whitish,
solid and well delimited from the surrounding tissues.
Figure 3. A. Hematoxylin eosin staining (2X magnification) showing
spindle cells arranged in a dense fibrous stroma. B. Hematoxylin
eosin staining (20X magnification). C. Diffuse positive staining for
smooth muscle actin. D. Proliferation index was 20% based on Ki67
immunostaining.
The postoperative course was complicated by a grade A [9] pancreatic fistula, most likely due to a pancreatic capsule tear, which healed spontaneously. Considering the intraoperative findings and the lesion features, no adjuvant chemotherapy or radiation therapy was administered. At 12 months follow-up the patient is in good health and free from recurrence.
DISCUSSION
In this article we report a rare case of primary leiomyosarcoma of the splenic vein. To our knowledge, this is the first case treated with local tumor excision and direct repair of the splenic vein by end-to-end anastomosis.
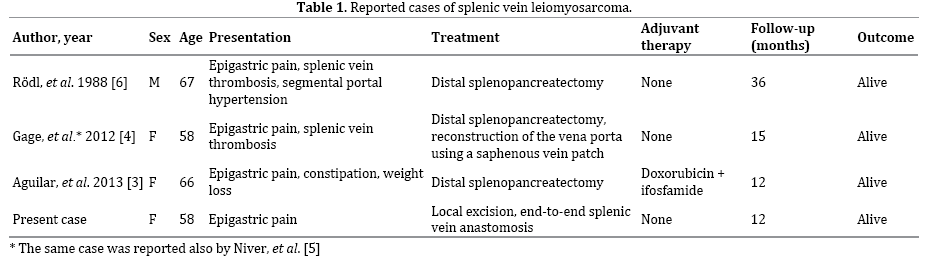
Splenic vein LMS is extremely rare. We performed a PubMed search using the terms “splenic vein leiomyosarcoma” and “primary venous leiomyosarcoma”, retrieving only three published cases. Rödl et al. [6] reported the first case of a 67-year-old man with a 15-cm splenic vein LMS involving the pancreatic tail and the splenic hilum, presented with long-term epigastric pain. This large mass compressed the gastric wall and caused splenic vein thrombosis, leading to segmental portal hypertension with perigastric varices. The patient was treated with a wide distal splenopancreatic resection and was alive at 3 years follow-up. Two further cases were reported (Table 1), both patients underwent a distal splenopancreatectomy and were alive at the end of follow-up. The case by Gage et al. [4] (also reported by Niver [5]) similarly presented with splenic vein thrombosis and required a partial reconstruction of the portal vein using an autologous saphenous vein patch. The last case reported by Aguilar et al. [3] was the first treated with adjuvant chemotherapy including doxorubicin and iphosphamide.
Similarly to other primary venous LMSs, those involving the splenic vein seem to occur mainly in women in their sixth decade of life [10].
Primary venous LMS is an aggressive disease with a reported 5-year survival of 33–68% [2, 10-16]. They are frequently asymptomatic for a long time and at the diagnosis the tumor is often of considerable size.
Complete en bloc surgical resection of all involved organs represents the treatment gold standard, occasionally achieving long-term survival [2, 10]. The prognostic value of the microscopic involvement of the resection margin is controversial [2]. Patients who are not fit for resection and those undergoing palliative intervention generally have a poor prognosis.
Another issue is the restoration of the venous flow, whose complexity mainly depends on the location/extent of the venous involvement and the presence collateral venous circulation [2, 11, 13, 15, 16].
In our case, a small sized and capsulated tumor, a complete resection with negative margin was obtained with local excision and direct splenic vein re-anastomosis. The choice of a “limited” resection was related to the macroscopic non infiltrating tumor appearances and the absence of malignant feature at the intraoperative histological examination.
The value of postoperative radiation therapy is also debated, but given the high risk of local recurrence there seems to be a rationale for adjuvant radiation therapy. Hines et al. [12] reported a 53% 5 years survival rate for inferior vena cava LMS and an increased median survival rate (6 versus 51 months) in patients treated with adjuvant radiation therapy. On the other hand, other Authors could not find evidence of improved survival rate due to radiation therapy [2, 11]. However, as the indication of possible confounding factors influencing the outcome of patients receiving radiation therapy, is lacking the assessment of its effectiveness is virtually impossible.
There is very little evidence of survival rate improvement in patients receiving adjuvant chemotherapy. Reported chemotherapy was heterogeneous and inconsistently administered [2, 3, 10-16] and there is a lack of prospective studies with new drugs.
A careful post-surgical follow-up is warranted for these patients, because of the risk of local recurrence and metastases (mainly involving liver and lung).
Our patient underwent radical surgery and no adjuvant chemotherapy/radiation therapy was therefore given. She is currently on follow up at our institution.
In conclusion, given the rarity of primary venous LMS of the splenic vein, it is difficult to state any management recommendation. Radical surgical resection is the treatment mainstay while the role of adjuvant therapy is controversial. All patients should be closely monitored after resection, due to the high recurrence rate and disease related mortality.
Conflict of Interest
Authors declare to have no conflict of interest.
References
- Ceyhan M, Danaci M, Elmali M, Ozmen Z. Leiomyosarcoma of the inferior vena cava. Diagnostic and interventional radiology. 2007; 13: 140-143. [PMID: 17846988]
- Hollenbeck ST, Grobmyer SR, Kent KC, Brennan MF. Surgical treatment and outcomes of patients with primary inferior vena cava leiomyosarcoma. Journal of the American College of Surgeons. 2003; 197: 575-579. [PMID: 14522326]
- Aguilar C, Socola F, Donet JA, Gallastegui N, Hernandez GA. Leiomyosarcoma of the splenic vein. Clinical Medicine Insights Oncology. 2013; 7: 263-268. [PMID: 24250242]
- Gage MJ, Newman E, Maldonado TS, Hajdu CH. Leiomyosarcoma of the splenic vein. Journal of vascular surgery. 2012; 55: 1485-1487. [PMID: 22051866]
- Niver BE, Megibow AJ, Faust MJ, Rosenkrantz AB. Multidetector CT appearance of leiomyosarcoma of the splenic vein. Clinical radiology. 2011; 66: 688-690. [PMID: 21356533]
- Rodl W, Hofmann-Preiss K. [Leiomyosarcoma of the splenic vein]. Radiologe. 1988; 28: 42-44. [PMID: 3344346]
- Guillou L, Coindre JM, Bonichon F, Nguyen BB, Terrier P, Collin F, et al. Comparative study of the National Cancer Institute and French Federation of Cancer Centers Sarcoma Group grading systems in a population of 410 adult patients with soft tissue sarcoma. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 1997; 15: 350-362. [PMID: 8996162]
- Miettinen M. Immunohistochemistry of soft tissue tumours - review with emphasis on 10 markers. Histopathology. 2014; 64: 101-118. [PMID: 24111893]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005; 138: 8-13. [PMID: 16003309]
- Mingoli A, Cavallaro A, Sapienza P, Di Marzo L, Feldhaus RJ, Cavallari N. International registry of inferior vena cava leiomyosarcoma: analysis of a world series on 218 patients. Anticancer research. 1996; 16: 3201- 3205. [PMID: 8920790]
- Dzsinich C, Gloviczki P, van Heerden JA, Nagorney DM, Pairolero PC, Johnson CM, et al. Primary venous leiomyosarcoma: a rare but lethal disease. Journal of vascular surgery. 1992; 15: 595-603. [PMID: 1560548]
- Hines OJ, Nelson S, Quinones-Baldrich WJ, Eilber FR. Leiomyosarcoma of the inferior vena cava: prognosis and comparison with leiomyosarcoma of other anatomic sites. Cancer. 1999; 85: 1077-1083. [PMID: 10091791]
- Kieffer E, Alaoui M, Piette JC, Cacoub P, Chiche L. Leiomyosarcoma of the inferior vena cava: experience in 22 cases. Annals of surgery. 2006; 244: 289-295. [PMID: 16858193]
- Kyriazi MA, Stafyla VK, Chatzinikolaou I, Koureas A, Chatziioannou A, Kondi-Paphiti A, et al. Surgical challenges in the treatment of leiomyosarcoma of the inferior vena cava: analysis of two cases and brief review of the literature. Annals of vascular surgery. 2010; 24: 826 e13-17. [PMID: 20471215]
- Laskin WB, Fanburg-Smith JC, Burke AP, Kraszewska E, Fetsch JF, Miettinen M. Leiomyosarcoma of the inferior vena cava: clinicopathologic study of 40 cases. The American journal of surgical pathology. 2010; 34: 873-881. [PMID: 20463568]
- Tilkorn DJ, Hauser J, Ring A, Goertz O, Stricker I, Steinau HU, et al. Leiomyosarcoma of intravascular origin--a rare tumor entity: clinical pathological study of twelve cases. World journal of surgical oncology. 2010; 8: 103. [PMID: 21092216]




