Keywords
Complications; Pancreas; Pancreatectomy
Abbreviations
LLP laparoscopic left pancreatectomy; LLSP laparoscopic left splenopancreatectomy
INTRODUCTION
In the recent years, the laparoscopic approach to left pancreatectomy has been increasingly adopted in most high volume pancreatic surgery centers. However, even with the acquired experience over the years and the development of new surgical instruments, it is still considered a technically demanding surgical procedure due to various factors, such as the retroperitoneal localization of the pancreas and its anatomical relationship to the mesenteric and celiac vessels. In spite of that, laparoscopic left pancreatectomy (LLP) goes towards becoming the gold standard [1] in next years for the treatment of pancreatic lesions located left to the mesenteric vessels.
One of the major concerns about pancreatic surgery, both open and laparoscopic, is the presence of complications in the postoperative period, both related and unrelated to the pancreas. Without doubt, the most frequently acknowledged complication after a pancreatectomy is the appearance of pancreatic fistula; nevertheless, other complications can occur. There are many studies in the literature comparing the incidence of complications between open and laparoscopic left pancreatectomies [2- 14], and their results show a consistent advantage of the laparoscopic approach in terms of intraoperative blood loss, postoperative hospital stay, and overall complications.
On the other hand, when performing a LLP, one of the most important decisions is whether to preserve the spleen or not. It is generally admitted that, in case of malignant disease of the body-tail of the pancreas, the spleen must be resected, while when dealing with a benign lesion, it can be preserved. However, laparoscopic splenic vessel preservation may be a technically difficult procedure, while, while the widespread adoption of the spleen preservation without splenic vessels preservation (Warshaw technique [15]) has raised concerns about its safety and its association with postoperative complications, such as splenic infarction, splenic abscesses and development of a perigastric collateral circulation [16].
Since the occurrence of major complications after LLP may have an important impact on the postoperative outcome, the aim of this study is to identify preoperative and intraoperative risk factors associated with major complications after a LLP in a series of 115 consecutive patients, in order to be able to avoid them.
PATIENTS AND METHODS
Patients
All patients operated of LLP in Hôpital Haut-Lévêque, CHU Bordeaux (Bordeaux, France) and Centre Hépato- Biliaire Paul Brousse (Villejuif, France) since 1997 were prospectively recorded in a database. The total number of consecutive patients included in this study and treated by LLP from 1997 to 2014 was 115. A retrospective analysis of this prospective recorded database was made.
All surgical interventions were performed by three senior surgeons (ASC, BM, CL), all of them with extensive previous experience of both pancreatic and laparoscopic surgery.
Surgical Technique
Three different surgical techniques for LLP were used, which have been previously described. Briefly, for all patients, installation in the operating room was similar: patients were placed in the supine position with open legs. The main surgeon stayed between the patient’s legs with two assistants, one at each side of the patient. One or two surgical monitors were positioned at the left or at each side of the patient’s head. Penumoperitoneum was created with an open technique with a 10 mm midline incision 1 to 2 centimeters above the umbilicus. Four trocars were inserted under direct view in the majority of the procedures: a 10 mm trocar placed at the supraumbilical incision for the optics, a 10 mm trocar in the left midclavicular line at the same level of the previous one, a 5 mm trocar in the right midclavicular line still at the same level than the previous one, and finally a 5 mm in the sub-xiphoid area for retraction.
The first part of the intervention consisted in a systematic view of the abdominal cavity, and a liver ultrasound was performed in those cases with a suspicious for malignancy. Then, the stomach was retracted cranially and the lesser sac was entered between the omentum and the transverse colon preserving omental and gastroepiploic vascularization. In this step, it is of the utmost importance the preservation of the short gastric vessels if spleen preservation is attempted. After identification of the pancreatic gland, an intraoperative ultrasonography of the pancreas was performed in order to identify the lesion and its relationships to the surrounding anatomical structures. After confirming the preoperative findings, and without any formal contraindication to resection, surgical dissection of the pancreas was started. After dissection of the inferior border of the pancreas at the neck, the superior mesenteric vein (SMV) was identified. Dissection continued in the cranial direction and the splenic vein was identified. Then, dissection of superior border of the pancreas was performed, identifying the splenic artery and dissecting the space between the common hepatic artery and the gastroduodenal artery until the portal vein (PV) was visualized. Finally, dissection of the SMV towards the PV was finalized, creating a tunnel behind the pancreatic neck. The pancreatic neck is encircled and suspended by a tape passed through the retropancreatic tunnel. Then, dissection of the inferior pancreatic border continues from right to the left of the patient until reaching the spleen. At the end of dissection, pancreatic transection was performed with a 60 mm endostapler. At this moment, depending on the operative findings, the preoperative diagnosis and the surgeon’s choice, one of the following surgical procedures was chosen:
Laparoscopic Left Splenopancreatectomy (LLSP)
After completing pancreatic transection, splenic artery and vein are clipped and divided. This maneuver will allow for a reduction of the spleen volume and bleeding. Dissection of the inferior pancreatic border continued until the splenocolic and splenorenal attachments, which were divided, as well as the short gastric vessels. Posterior dissection of the pancreas and spleen was completed.
Laparoscopic Left Pancreatectomy with Splenic Vessels Preservation (LLP-SVP)
After pancreatic transection, careful dissection of the splenic vessels towards the spleen was performed, ligating and sectioning all small venous and arterial tributaries. Once the tail end of the pancreas was reached and freed from splenic vessels, surgical specimen was obtained.
Laparoscopic Left Pancreatectomy without Splenic Vessels Preservation, Or Warshaw Technique (LLP-WT)
The splenic artery was dissected, clipped and divided at the origin, with the purpose to reduce the bleeding. Then, posterior pancreatic dissection was performed towards the pancreatic tail. At this point, the splenic hilum was transected by means of stapling or by ligating and dividing each arterial and venous branch. Finally, the splenic vein was clipped and divided at its origin.
Definition of Complications
Patients' complications were prospectively noted in the database after each patient discharge and classified according to Dindo-Clavien classification of surgical complications [17]. We considered major complications the events with a grading equal or superior to grade III.
STATISTICAL ANALYSIS
Results are shown as number of cases and percentage from total number of patients. For the univariate analysis, a 2x2 categorical analysis using the Fisher’s exact F test was performed. The multivariate analysis was performed using multiple logistic regression tests of all factors proved to be statistically significant in the univariate analysis. A measurement was considered statistically significant if p<0.05. The statistical analysis of the data was carried out using the SPSS Statistics 18.0 (SPSS, Chicago, IL) computer program.
RESULTS
Patients and Types of Surgical Procedures
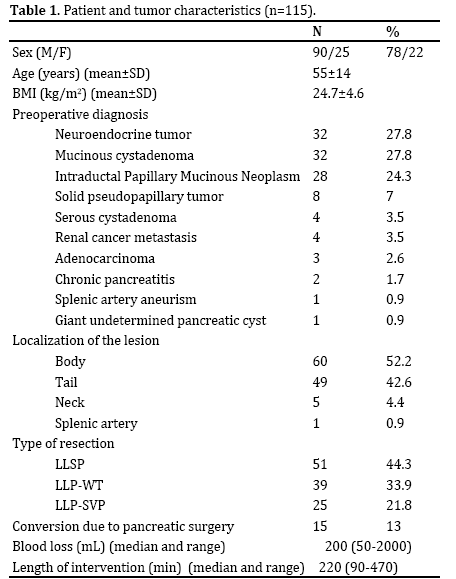
This study includes 115 consecutive patients who underwent LLP from 1997 to 2014. Patients' demographic aspects, preoperative diagnosis, tumor localization, type of resection and intraoperative results are reported in Table 1.
Postoperative Complications
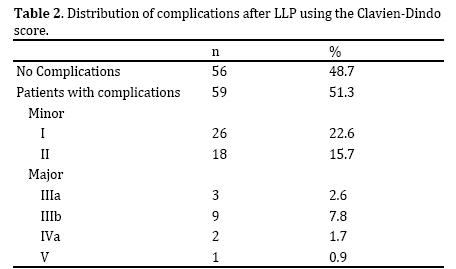
In this series of 115 consecutive patients, overall complications occurred in 59 patients (51%) in the first 60 postoperative days. Two more patients needed further surgery beyond 60 days, one due to incisional hernia, and one because the pancreatic lesion (small neuroendocrine tumour) was not found in the surgical specimen after pathologic examination. Major complication rate was 13%, and the mortality rate was 0.87%. Table 2 shows postoperative complications stratified according to the Dindo-Clavien classification.
Morbidity
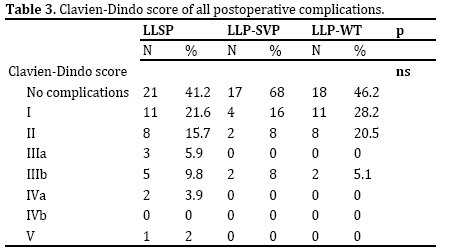
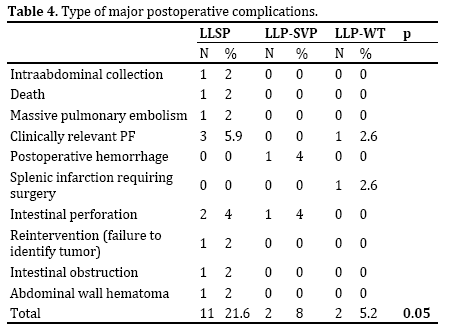
Out of the 59 patients with postoperative complications, 44 patients (74.6%) presented a minor postoperative complication (Dindo-Clavien grades I and II), whereas 15 patients (13% of all patients, 25.4% of the complicated patients) developed a major complication. Three patients presented a complication IIIa: they presented an intraabdominal fluid collection needing percutaneous drainage placement; in two of them the collection was a consequence of a clinical pancreatic fistula, while in the other the origin was an infected postoperative collection not related to any pancreatic fistula. Nine patients presented a complication IIIb: they presented a postpancreatectomy hemorrhage (3), intestinal perforation evidenced by drainage output (2), abdominal wall hematoma (1), intestinal occlusion due to postoperative adherences (1), splenic infarction after LLP-WT which required splenectomy (1), and an intraabdominal collection treated by percutaneous drainage under general anesthesia (1). Finally, two patients had a complication graded IVa: one patient presented a postoperative hemorrhage needing reintervention and a further laparotomy for intestinal perforation which required ICU treatment. The other patient presented a massive pulmonary embolism which also required transfer to the ICU. Table 3 shows all postoperative complications depending on the chosen surgical procedure. In addition, major complications by procedure are summarized in Table 4.
Mortality
One patient died 48 hours after surgery. This particular patient was a 79-year-old man with important comorbidity (obesity, aortic aneurysm, insulin-dependent diabetes mellitus and pulmonary emphysema) with a preoperative diagnosis of ductal adenocarcinoma of the pancreatic tail. The cause of death was a non-recoverable cardiac arrest due to cardiac infarction.
Univariate Analysis of Risk Factors for Major Complications
Both preoperative and intraoperative potential risk factors for major morbidity were evaluated, as depicted in Table 5.
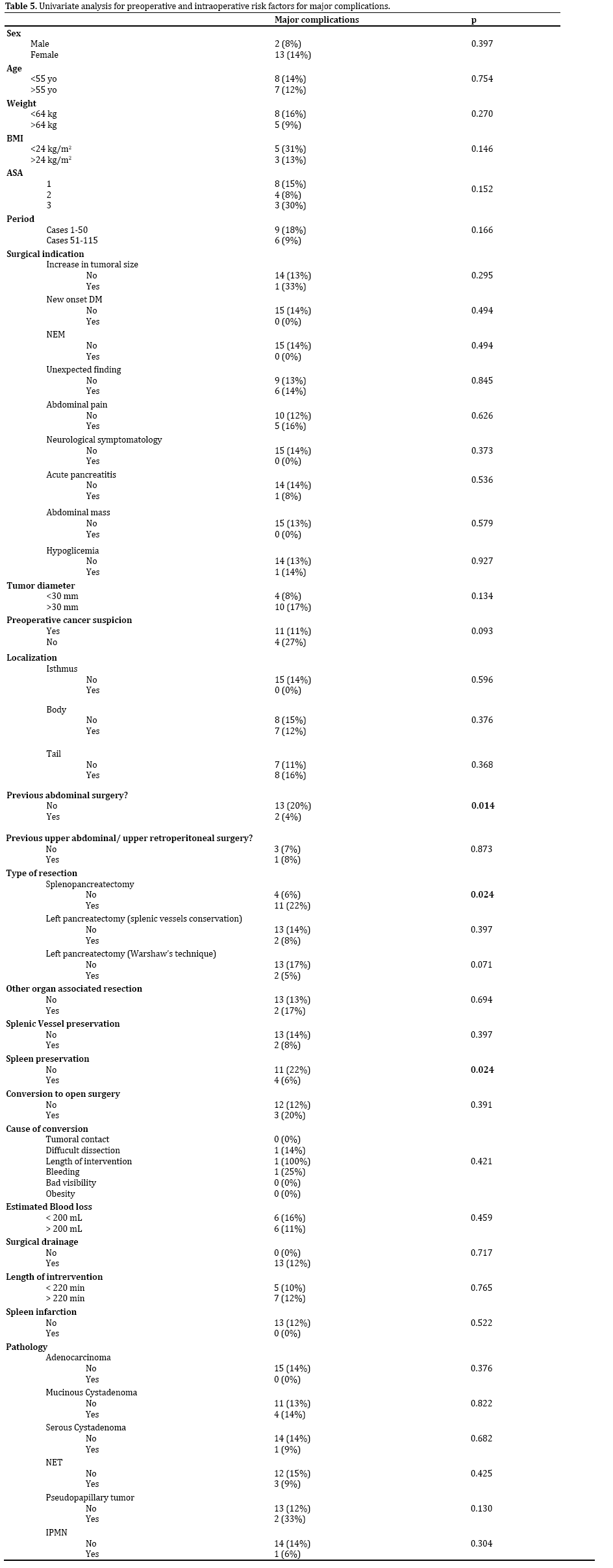
Amongst the preoperative and intraoperative risk factors, only two statistically significant risk factors were identified: previous abdominal surgeries and LLSP.
About the first (preoperative risk factor), patients without previous abdominal surgeries were found to be at higher risk for developing postoperative major complications (20% vs. 4%, p=0.014) which were predominantly represented by appendiceal or gynecological procedures. Indeed considering the patients with previous upper abdominal intraperitoneal or retroperitoneal surgeries, such as cholecystectomy (n=5), nephrectomy (n=7) and liver transplantation (n=1), an increased risk for major complications was not found (7% vs. 8%, p=ns).
About the second intraoperative risk factor, LLSP was associated with an increased risk for postoperative major complications (22% vs. 6%, p=0.024) or, in other words, spleen preservation was found to be a protective factor.
Multivariate Analysis of Risk Factors for Major Complications
Multivariate analysis (Table 6) identified only the performance of an LLSP as an independent risk factor for postoperative major complications (p=0.019, HR (95% CI): 4.617 (1.292-16.497)).

DISCUSSION
Despite all the advances both in the knowledge and technical field, the appearance of complications after major abdominal surgery is a fact. Pancreatic surgery, being a specific type of surgery, is often associated with important morbi-mortality for many reasons (such as its anatomical location) and with specific complications, mainly pancreatic fistula. Therefore it has already been specifically demonstrated in pancreatic surgery as well as in laparoscopic surgery that high volume centers and experienced surgeons play an important role to reduce the incidence of postoperative complications.
The laparoscopic approach in pancreatic surgery was first introduced approximately 20 years ago [18], and since then it has been progressively adopted by previously experienced laparoscopic and pancreatic surgeons. Many studies have compared patient outcomes between open and laparoscopic left pancreatectomy. Although a randomized controlled trial is still lacking, results from many of these well-designed observational studies and meta-analysis show that both techniques are equivalent in terms of overall postoperative complications, being the laparoscopic approach superior in terms of intraoperative blood loss, postoperative hospital stay [2, 4, 6, 8-12, 19, 21, 22], and even more cost-effective [7, 8, 21] than its open counterpart. However, data from these studies also indicates that the overall length of the surgical procedure is increased when the laparoscopic approach is utilized. Nevertheless, at least to our knowledge, risk factors for developing postoperative major complications after LLP have never been explicitly studied. In this study we have investigated preoperative or intraoperative factors that could have an impact on postoperative complications after LLP, in a large consecutive cohort of patients treated by surgeons with previous extensive pancreatic and laparoscopic experience.
After the univariate analysis of all preoperative and intraoperative factors, only 2 were statistically associated with an increase of major postoperative complications, as shown in Table 5: previous abdominal surgery and splenopancreatectomy (LLSP). We are going to analyze each factor separately.
The first factor associated with increased postoperative complications is the presence of previous abdominal surgery (20% vs. 4%, p=0.014) and we analyzed what kind of previous surgeries the patients underwent. Surprisingly the vast majority of patients underwent lower abdominal/ pelvic surgeries, such as appendectomy, gynecological or prostatic procedures. Despite the presence of postoperative adhesions could make difficult the LLP (especially in case of appendicular peritonitis), we didn't expect that lower abdominal/pelvic surgeries should really be accounted as a potential risk factor for postoperative complications. A further analysis conducted on patients who underwent upper abdominal surgery (both intra or retroperitoneal), didn't show an increased incidence of postoperative complications (14% vs. 8%, p=ns).
The second factor found to be associated to postoperative complications in our group of patients was splenopancreatectomy (22% vs. 6%, p=0.024), that was the only significant independent factor in the multivariate analysis (p=0.019; HR (95% CI) 4.617 (1.292-16.497). Moreover it’s worthy to note, as shown in Table 5, that LLP-SVP or LP-WT were not associated to an increased risk of postoperative complications. Obviously, splenectomy is formally indicated in case of malignant lesions of the pancreatic body-tail, in order to accomplish an oncological resection. But when a not malignant pancreatic lesion is placed to the extremity of pancreatic tail, this situation prompts the surgeon to perform the splenectomy as well. Although we know from long time that splenectomy is connected to long-term infectious complications, which are rare but with significant morbidity, now we should claim, according to the results of this study, that splenectomy may also lead to an increased risk of shortterm complications. As a result, the findings of this study suggest that, whenever possible, efforts must be done in order to preserve the spleen during LLP. However, we look forward in the future to confirm the data of this study; overall surgical complications graded by Clavien- Dindo classification are not different between the three surgical techniques as shown in Table 3, and what it seems to be more important, there is not an evident cause related to splenectomy for the presence of a significantly higher number of major complications after LLSP. If we analyze what kind of major complications did the patients experience, as depicted in Table 4, most complications in the LLSP group, such as a clinically relevant PF or intestinal perforation, are not directly explained by the removal of the spleen alone.
Interestingly, we didn't also found any differences in major complications between LLP-SVP and LLP-WT (8% vs. 5.1%, p=0.64). In fact, although this is not the topic of this study, the comparison of both techniques shows no differences in blood loss or length of intervention (data not shown in results). The critic issue of LLP-WT is the splenic ischemia that was observed in only 3 patients (7.6%), one of which had to undergo a splenectomy due to septic complications from the ischemic spleen (2.5% of all LLPWT patients).
Contrary to what could be expected, the learning curve and conversion to open surgery were not significant risk factors for major complications in our experience. As reported in Table 5, the "learning curve effect" was not quite evident in this series, since there was not a significant increase of major complications in the first period compared to the second one.
There are mainly two factors that could potentially explain this phenomenon: first, the surgical team had experience both in laparoscopic and in pancreatic surgery. Second, since careful cases selection, the patients were probably less complicated at the beginning of the experience than in the second period.
Similarly, conversion to open surgery did not mean an increase in major postoperative complications, probably because we adopted a low threshold to conversion, avoiding surgical mistakes and related postoperative unfavorable outcomes.
Finally we should as well note that some major complications that arose in our series, such as accidental intestinal perforation, happened almost exclusively under the laparoscopic approach but we are not able to compare their incidence in open surgery. This underlines the fact that the laparoscopic approach may have a specific morbidity.
In conclusion, LLP is a surgical procedure associated to a low morbidity and mortality rate, when performed by an experienced surgical team. Our results suggest that spleen must be preserved, whenever possible and that LLP-SVP and LLP-WT have equivalent results in terms of major morbidity and mortality, paying close attention to splenic ischemia.
Acknowledgements
Authors would like to thank Pr. Bernard Masson for his work regarding this paper.
Conflict of Interests
Authors declare no conflict of interests for this article.
References
- Stutchfield BM, Joseph S, Duckworth AD, Garden OJ, Parks RW. Distal pancreatectomy: what is the standard for laparoscopic surgery? HPB (Oxford) 2009; 11:210–4. [PMID: 19590649]
- Eom BW, Jang JY, Lee SE, Han HS, Yoon YS, Kim SW. Clinical outcomes compared between laparoscopic and open distal pancreatectomy. Surg Endosc 2008; 22:1334–8. [PMID: 18027035]
- Kooby DA, Gillespie T, Bentrem D, Nakeeb A, Schmidt MC, Merchant NB, Parikh AA, et al. Left-sided pancreatectomy: a multicenter comparison of laparoscopic and open approaches. Ann Surg 2008; 248:438–46. [PMID: 18791364]
- Farnell, M. B. & Kendrick, M. L. Laparoscopic vs. open distal pancreatectomy. a single-institution comparative study. Arch Surg2010; 145:616–621. [PMID: 20644122]
- Butturini G, Partelli S, Crippa S, Malleo G, Rossini R, Casetti L, Melotti GL, et al. Perioperative and long-term results after left pancreatectomy: a single-institution, non-randomized, comparative study between open and laparoscopic approach. Surg Endosc 2011; 25:2871–8. [PMID: 21424200]
- Nigri GR1, Rosman AS, Petrucciani N, Fancellu A, Pisano M, Zorcolo L, Ramacciato G, et al. Metaanalysis of trials comparing minimally invasive and open distal pancreatectomies. Surg Endosc 2011; 25:1642–51. [PMID: 21184115]
- Abu Hilal M, Hamdan M, Di Fabio F, Pearce NW, Johnson CD. Laparoscopic versus open distal pancreatectomy: a clinical and cost-effectiveness study. Surg Endosc 2012; 26:1670–4. [PMID: 22179475]
- Limongelli P, Belli A, Russo G, Cioffi L, D'Agostino A, Fantini C, Belli G. Laparoscopic and open surgical treatment of left-sided pancreatic lesions: clinical outcomes and cost-effectiveness analysis. Surg Endosc 2012; 26:1830–6. [PMID: 22258300]
- Mehta SS, Doumane G, Mura T, Nocca D, Fabre JM. Laparoscopic versus open distal pancreatectomy: a single-institution case-control study. Surg Endosc 2012; 26:402–7. [PMID: 21909859]
- Pericleous S, Middleton N, McKay SC, Bowers KA, Hutchins RR.Systematic review and meta-analysis of case-matched studies comparing open and laparoscopic distal pancreatectomy: is it a safe procedure? Pancreas 2012; 41:993–1000. [PMID: 22836858]
- Soh YF, Kow AW, Wong KY, Wang B, Chan CY, Liau KH, Ho CK. Perioperative outcomes of laparoscopic and open distal pancreatectomy: our institution’s 5-year experience. Asian J Surg2012; 35:29–36. [PMID: 22726561]
- Sui CJ, Li B, Yang JM, Wang SJ, Zhou YM. Laparoscopic versus open distal pancreatectomy: a meta-analysis. Asian J Surg2012; 35:1–8. [PMID: 22726557]
- Limongelli P, Belli A, Belli G. Laparoscopic versus open left pancreatectomy: do risk factors for pancreatic fistula differ between the 2 techniques? Ann Surg 2014; 259:e39. [PMID: 24253145]
- Mardin WA1, Schleicher C, Senninger N, Mees ST.Laparoscopic versus open left pancreatectomy: can preoperative factors indicate the safer technique? Ann Surg 2014; 259:e60. [PMID: 24263306]
- Warshaw AL. Conservation of the spleen with distal pancreatectomy. Arch Surg1988; 123:550–3. [PMID: 3358679]
- Jean-Philippe A, Alexandre J, Christophe L, Denis C, Masson B, Fernández-Cruz L, Sa-Cunha A.Laparoscopic spleen-preserving distal pancreatectomy: splenic vessel preservation compared with the warshaw technique. JAMA Surg 2013;148:246-52. [PMID: 23682365]
- Dindo D, Demartines N, Clavien PA.Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. AnnSurg 2004; 240:205–213. [PMID: 15273542]
- Gagner M, Pomp A. Laparoscopic pylorus-preserving pancreatoduodenectomy. Surg Endosc 1994; 8:408–10. [PMID: 7915434]
- DiNorcia J, Schrope BA, Lee MK, Reavey PL, Rosen SJ, Lee JA, Chabot JA, et al. Laparoscopic distal pancreatectomy offers shorter hospital stays with fewer complications. J Gastrointest Surg 2010; 14, 1804–12. [PMID: 20589446]
- Iacobone M, Citton M, Nitti D. Laparoscopic distal pancreatectomy: up-to-date and literature review. World J Gastroenterol 2012; 18:5329–37. [PMID: 23082049]
- Braga M, Pecorelli N, Ferrari D, Balzano G, Zuliani W, Castoldi R. Results of 100 consecutive laparoscopic distal pancreatectomies: postoperative outcome, cost-benefit analysis, and quality of life assessment. Surg Endosc 2015; 29:1871-8. [PMID: 25294551]
- Venkat R, Edil BH, Schulick RD, Lidor AO, Makary MA, Wolfgang CL. Laparoscopic distal pancreatectomy is associated with significantly less overall morbidity compared to the open technique: a systematic review and meta-analysis. Ann Surg 2012; 255:1048–59. [PMID: 22511003]

