Keywords
Abdominal Injuries; Pancreatectomy; Spleen
Abbreviations
SPDP: spleen preserving distal pancreatectomy
INTRODUCTION
Distal pancreatectomy for major pancreatic trauma has traditionally involved removal of the spleen as an integral part of the procedure. The main advantages of removing the spleen during a distal pancreatectomy are the ease of performing this procedure and the shortened operating time. However, recently, a spleenpreserving distal pancreatectomy (SPDP) has become the standard care for benign diseases of the distal pancreas. Currently, there are not many reports in the literature to validate the feasibility and safety of the procedure in trauma. We tried to evaluate the feasibility and safety of the procedure in patients with stable distal pancreatic injury who required surgical intervention. The procedure avoids the post-operative complications related to a splenectomy [1, 2, 3, 4, 5, 6].
METHODS
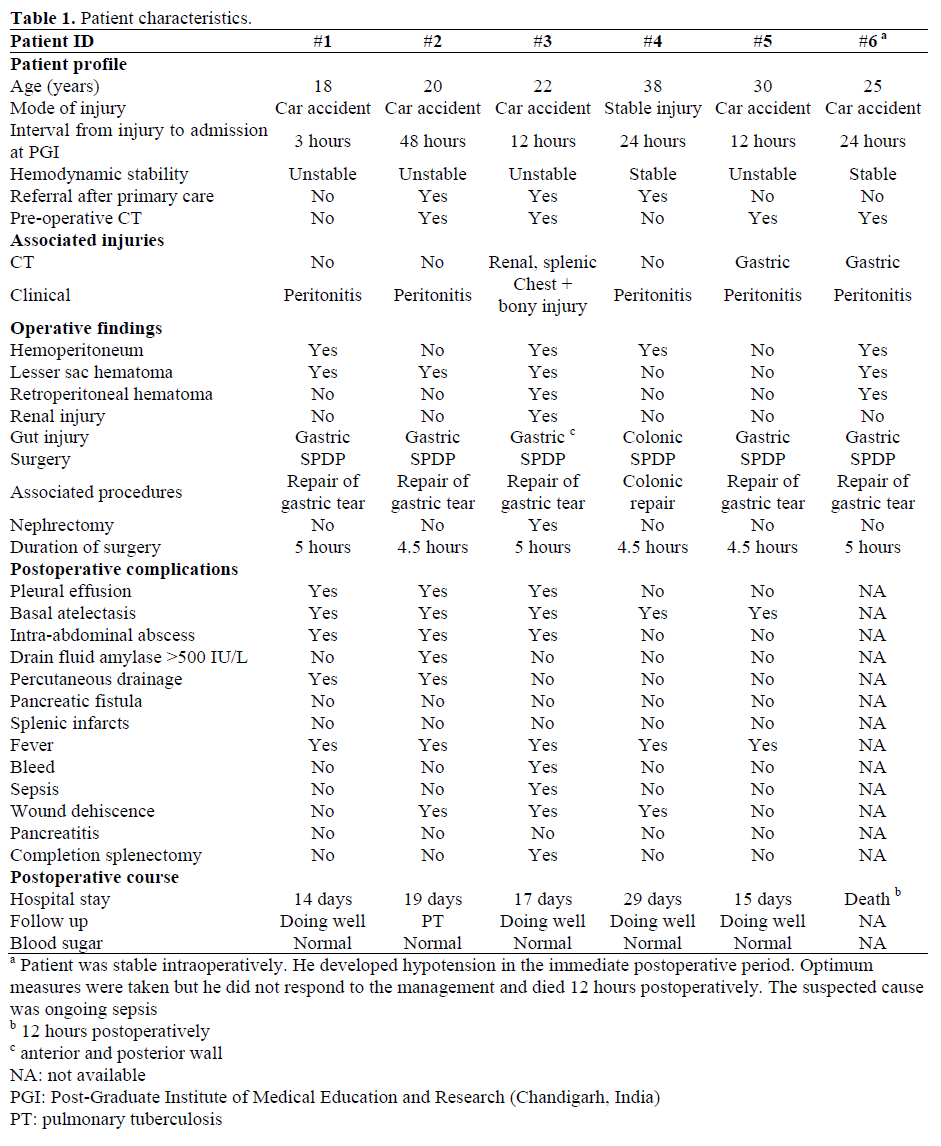
Patients admitted for pancreatic trauma to the Department of Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh between July 2001 and June 2005 were enrolled in the study. Six patients were found suitable for a spleen-preserving distal pancreatectomy based on their general conditions and a preoperative spleen contrastenhanced computerized tomography scan (CECT). Patients who were unstable even after resuscitation were excluded from the study. The preoperative characteristics, intraoperative findings and postoperative complications with follow up were studied (Table 1).
Case 1
This patient was an 18-year-old male who sustained injury in a car accident. He was hemodynamically unstable when admitted but was stabilized after resuscitation. He had clinical evidence of peritonitis. A CECT was not performed and emergency surgery was carried out.
Case 2
This patient was a 20-year-old male who sustained injury in a car accident. He responded to resuscitation. He had clinical peritonitis and a CECT was performed which showed evidence of pancreatic injury and free fluid in the peritoneum. He was taken for emergency surgery after adequate preparation.
Case 3
This patient was a 22-year-old male who sustained injury in a car accident. Clinically, he had chest and other bony injuries; there was no clinical evidence of peritonitis. A chest drain was put in and a CECT of the abdomen was performed which showed pancreatic injury with grade 2 injury to the spleen and left kidney. An SPDP was performed to repair a gastric tear, and the spleen and kidney were managed conservatively.
Case 4
This patient was a 38-year-old male with a stab injury in the abdomen who was stable when admitted to the Emergency Room. He had clinical peritonitis. He was examined and found to have colonic injury associated with pancreatic injury. An SPDP with repair of the colonic perforation was carried out.
Case 5
This patient was a 30-year-old male who sustained injury in a car accident. He was unstable when admitted and responded to resuscitation. There was clinical peritonitis. A CECT was performed which showed gastric injury in association with pancreatic injury. An SPDP to repair a gastric perforation was performed.
Case 6
This patient was a 25-year-old male who had sustained injury in a car accident. He was stable when admitted. There was clinical peritonitis. An abdominal CECT was performed which suggested gastric and pancreatic injury. An SPDP with repair of gastric perforation was carried out.
Technique of Spleen Preserving Distal Pancreatectomy
The abdomen was opened using a midline incision. A thorough examination of the peritoneal cavity was carried out. All injuries were identified. A Thorough peritoneal lavage was also done. The pancreas was lifted from the transected end, and the splenic vessels were carefully isolated by ligating the individual branches to the pancreas using a combination of cautery and suture ligation. Dissection was extended to the splenic hilum and, after exposing the splenic vessels, the distal pancreas was removed. The pancreatic duct could be identified in all our cases and was sutured with non-absorbable polypropylene suture, after which the pancreatic stump was sewn over with 3/0 Vicryl® (Ethicon Inc., Piscataway, NJ, USA) transverse mattress sutures (Figures 1-7). A No. 16 suction drain was placed in the pancreatic bed.
Figure 1. Transected neck of the pancreas
(intraoperative).
Figure 2. Distal pancreas being lifted off splenic
vessels.
Figure 3. Distal pancreas totally separated up to the
hilum.
Figure 4. Splenic vessels completely separated from
the pancreas.
Figure 5. Proximal transected end of pancreas.
Figure 6. Pancreas being separated from the splenic
hilum.
Figure 7. Healthy spleen after resection of the
pancreas.
Postoperative Monitoring
All patients were meticulously monitored during the postoperative period. Drain fluid and serum amylase were analyzed on days 1 and 4 after surgery. Monitoring for evidence of sepsis and hemorrhage was carried out.
Follow-up
Patients were specifically followed up to detect pancreatic insufficiency
ETHICS
Written informed consent was obtained from each patient and the study protocol conformed to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 (revised in Tokyo 2004), as reflected in a priori approval by the Postgraduate Institute of Medical Education and Research (Chandigarh, India) ethical committee.
STATISTICS
Mean values, standard deviations and frequencies were used to describe the data
RESULTS
Six patients were found to be suitable for SPDP based on their general condition and preoperative CECT (Figure 8). The average age of these patients was 25.5±7.4 years. Five patients had had car accidents and one had a stab injury. The average interval to admission was 20.5±15.7 hours. Four patients were unstable on arrival and two were stable. The four patients who were unstable were stabilized before surgery. Five patients had peritonitis, and one patient had renal and thoracic trauma. The average duration of surgery was 4.75±0.25 hours. All patients had associated hollow viscus injury which was repaired along with an SPDP. Five patients had a gastric tear and one had a colonic tear; all of which were primarily repaired. A nephrectomy was carried out in the patient with renal injury.
Figure 8. Preoperative CECT showing the transected
pancreas.
peritonitis, and one patient had renal and thoracic trauma. The average duration of surgery was 4.75±0.25 hours. All patients had associated hollow viscus injury which was repaired along with an SPDP. Five patients had a gastric tear and one had a colonic tear; all of which were primarily repaired. A nephrectomy was carried out in the patient with renal injury. One patient developed hypotension in the immediate postoperative period. Even after optimum management, he did not respond and died 12 hours postoperatively. One of the patients required a completion splenectomy as a result of post-operative intra-abdominal hemorrhage. The splenic vein was found to be the source and, therefore, had to be ligated. The most common postoperative complication was fever with basal atelectasis. Three of these patients developed pleural effusion. Three patients developed intraabdominal abscesses which were managed by percutaneous aspiration in one patient and drainage in the other two. One patient had an elevated drain fluid amylase level but the levels decreased with conservative management and octreotide. No patient had a splenic infarct or pancreatitis. The average postoperative hospital stay was 18.8±6.0 days. No patient developed pancreatic endocrine insufficiency.
The preoperative characteristics, intraoperative findings and postoperative complications with follow up are shown in Table 1.
DISCUSSION
Spleen preservation during distal pancreatectomy was described in the 1940s by the French surgeon Mallet-Guy [2]. It is the usual practice to remove the spleen while resecting the distal pancreas because it shortens the operating time, is technically less demanding and avoids dissection of the splenic vessels away from the pancreatic parenchyma [2, 3, 4]. However, recognition of the immunological and hematological functions of the spleen and the risk of overwhelming sepsis in splenectomized patients has lead to the concept of splenic preservation. An SPDP is, by definition, the conservation of the spleen during a distal pancreatectomy. A review of the English literature available revealed very few instances of this procedure having been performed for pancreatic trauma [2, 3, 4, 5, 6, 7, 8].
SPDP prolongs operating time and, therefore, the patient should be hemodynamically stable after resuscitation. The procedure can be performed by three different methods.
In the first method, a distal pancreatectomy can be performed without preserving the major splenic vessels as described by Warshaw et al. [9] (the short gastric and left gastroepiploic vessels are preserved). The splenic vessels are ligated at the level of transection of the pancreas. The spleen regains its normal blood supply about ten days post-operatively [10] and survives on the blood supply from the short gastric and the left gastroepiploic vessels. Therefore, avoiding injury of these vessels during surgery is recommended. It has also been observed that avoiding dissection in the splenic hilum in such a situation may help in the preservation of the short gastric vessels thereby avoiding post-operative splenic necrosis [11].
The second method includes the preservation of the splenic vessels by careful dissection of the branches to and from the pancreas as was done in our patients. In this procedure, the splenic blood supply continues to be maintained thus reducing the frequency of post-operative splenic necrosis and abscess formation. However, the operating time is longer. The dissection is time consuming and requires a meticulous approach [6]. Scott- Conner documented approximately 22 pancreatic tributaries draining into the splenic vein, and about eight arterial branches from the splenic artery supplying the pancreas [6]. Most of the pancreatic tributaries have been documented to be present near the body and tail of the pancreas. We would like to emphasize the importance of avoiding the shearing of the pancreas from the splenic vessels in this region which, if it does occur, may lead to avulsion of these tiny vessels with bleeding, thus prolonging the operating time. Some authors have suggested leaving a cuff of pancreatic tissue around these small vessels in order to avoid such a problem [12]. In the third method, all the vessels supplying the spleen (splenic, short gastric and gastroepiploic arteries) are divided during a distal pancreatectomy. Therefore, this may not be a suitable method because such surgery compromises the blood supply of the spleen [13].
Intra-abdominal abscess formation and splenic infarction have been reported to be the main complications of SPDP [3, 4]. One of our patients required a completion splenectomy as a result of post operative intra-abdominal hemorrhage. The splenic vein was found to be the source and hence had to be ligated. The possibility of post-operative hemorrhage from the splenic vein because of digestion by the pancreatic juices (from the resected end of the pancreas) and torsion of the splenic vessels remains a theoretical possibility [13]. Another patient had hypotension in the immediate postoperative period and died within first 24 hours. There was no clinical or biochemical evidence of postoperative bleeding. We suspected ongoing sepsis to be the cause, the result of a 24-hour old perforation.
CONCLUSION
SPDP with preservation of the splenic vessels, although technically demanding, can be performed safely and in an emergency procedure provided the patient is hemodynamically stable. It has the advantage of preserving the splenic blood flow and reducing post-splenectomy complications.
Conflict of interest
The authors have no potential conflicts of interest
References
- Holdsworth RJ, Irving AD, Cuschieri A.
Postsplenectomy sepsis and its mortality rate: actual
versus perceived risks. Br J Surg 1991; 78:1031-8.
[PMID 1933181]
- Aldridge MC, Williamson RCN. Distal
pancreatectomy with and without splenectomy. Br J
Surg 1991; 78:976-9. [PMID 1913121]
- Ivatury RR, Simon RJ, Guignard J, Kazigo J,
Gunduz Y, Stahl WM. The spleen at risk after
penetrating trauma. J Trauma 1993; 35:409-14. [PMID
8371300]
- Pachter HL, Hofstetter SR, Liang HG, Hoballah J.
Traumatic injuries to the pancreas: the role of splenic
preservation. J Trauma 1989; 29:1352-5. [PMID
2681807]
- Robey E, Mullen JT, Schwab CW. Blunt
transection of the pancrease treated by distal
pancreatectomy, splenic salvage and hyperalimentation.
Four cases and review of the literature. Ann Surg 1982;
196-695-9. [PMID 6816155]
- Dawson DL, Scott-Conner C. Distal
pancreatectomy with splenic preservation: the anatomic
basis for a meticulous operation. J Trauma 1986;
26:1142-5. [PMID 3795315]
- Richardson DQ, Scott-Conner CE. Distal
pancreatectomy with and without splenectomy. A
comparative study. Am Surg 1989; 55:21-5. [PMID
2913905]
- McGahren ED, Magnuson D, Schaller RT, Tapper
D. Management of transected pancreas in children.
Aust N Z J Surg 1995; 65:242-6. [PMID 7717941]
- Warshaw AL. Conservation of the spleen with
distal pancreatectomy. Arch Surg 1988;123:550-3.
[PMID 3358679]
- Sato Y, Shimoda S, Takeda N, Tanaka N,
Hatakeyama K. Evaluation of splenic circulation after
spleen-preserving distal pancreatectomy by dividing
the splenic artery and vein. Dig Surg 2000; 17:519-22.
[PMID 11124560]
- Schein M, Freinkel W, D'Egidio A. Splenic
conservation in distal pancreatic injury: stay away from
the hilum! J Trauma 1991; 31:431. [PMID 2002537]
- Govil S, Imrie CW. Value of splenic preservation
during distal pancreatectomy for chronic pancreatitis.
Br J Surg 1999; 86:895-8. [PMID 10417561]
- Kimura W, Inoue T, Futakawa N, Shinkai H, Han
I, Muto T. Spleen-preserving distal pancreatectomy
with conservation of the splenic artery and vein.
Surgery 1996; 120:885-90. [PMID 8909526]









