What is known on this subject
• Most appearance-related research is conducted in western cultures with individuals who have a good
command of the English language.
• Stigma and shame may be experienced by the individual affected and by their family as a result of culturally
specific expectations of physical appearance.
• Religion exerts powerful influences on personal perceptions, attitudes and beliefs with regard to healthcare.
What this paper adds
• Generational differences in South Asian community views about disfigurement appear to emerge from
westernisation and the influence of the media.
• There is a change in the orientation of younger members of the South Asian community away from
traditional religiously framed perceptions of acceptable appearance.
• Educational interventions are needed to highlight the support services available and also to dispel myths.
Introduction
This paper discusses the findings of an exploratory
study of South Asian community attitudes towards
individuals with a disfigurement. In the UK, people of
South Asian descent (i.e. those ethnic groups originating
from the Indian subcontinent) constitute one
of the largest ethnic minority groups, representing 4%
of the total population. This is a heterogeneous group
that includes people of diverse cultural heritage, who
have different religious beliefs, speak different languages
and possess varying levels of literacy.
There has not been adequate research into the way
in which different cultural and ethnic groups view
the cause and consequences of disfigurements, and the
socially constructed representations of differences within
their groups. Few standardised appearance measures
have been translated, so most appearance-related research
is conducted in western cultures, mainly in the
USA and the UK, with individuals who have a good
command of the English language (Rumsey and
Harcourt, 2004). Therefore it was considered a priority
to conduct a pilot study designed to explore
attitudes and perceptions towards appearance and
disfigurement among selected minority ethnic groups.
The current research is an extension of a larger multicentre
research programme in the majority population
supported by the Healing Foundation and led
by the Centre for Appearance Research at the University
of the West of England. The knowledge generated
by the research programme will inform the development
of a comprehensive range of health policy
recommendations and interventions designed to promote
positive adjustment in those affected by disfigurement.
It will also facilitate the possibility of
comparing the views of the South Asian sample, as
observed in the present study, with white British
perspectives.
Background
Cultural variations in ideas about attractiveness or
unattractiveness and the reasons for our preferences
have intrigued scientists and philosophers for centuries
(Adamson and Doud Galli, 2009). An attractive appearance
informs others of our ancestral value, whether we
are potentially fertile and healthy, and whether our
geneswill create desirable progeny (Adamson and Doud
Galli, 2009). Ubiquitous media artefacts may play a
role in shaping our preferences with regard to appearance,
and these ideal media representations of beauty
may contribute to greater dissatisfaction with our
bodies (Langlois et al, 1991).
Etcoff (1994) has argued that beauty may not be an
arbitrary cultural convention, and it has been shown
that concepts of facial beauty do not tend to vary much
among races or over time (Marquardt, 2002). Research
therefore suggests that our concepts of attractiveness
are primal and innate.
Yet other scholars maintain that the concept of
beauty is prescribed by cultural constructs and myths
of all cultures, and that every civilisation studied seems
to revere and pursue it (Schjedahl, 1998). Our preferencesmay
reflect cultural and social standards of beauty
which can vary with time and place, and may be
specific to cultures and faiths (Haiken, 2000; Poran,
2002; Swami and Tove´e, 2007). Furthermore, cultural
beliefs and practices shared by specific groups of
people may exert a strong influence on an individual’s
behaviour by defining behavioural norms, assumptions,
rules and relationships (Adamson and Doud
Galli, 2009). These norms give meaning to their world
and govern family life, childrearing, the recognition of
illness and health-seeking practices.
Indeed, the family has an important function in
enforcing cultural norms and values, and thus in
shaping views and perceptions (Rex, 1991). This has particular significance for South Asian families living
in the UK, in that family-based socialisation serves
the twin functions of imparting religious and cultural
values and countering what may be seen as the conflicting
or corrupting influences of the wider society
(Afshar, 1994; Anwar, 1998). The older generation of
South Asian people have strong perceptions of new
freedoms and views as threatening to the continuation
of traditional cultural values, such as parental authority
and obligations, possible changes in marriage
choices, and concerns about appearance (Modood et al,
1994). Young people adopt their own views, seeking
sources from different and often conflicting value
systems. Changes to familial value systems may not
result solely from a rejection (a relatively rare phenomenon)
of these values (Drury, 1991), but also from
partial acceptance and reinterpretation of some of them,
thereby constructing hybrid identities (Papastergiadis,
1998). Alternatively, it may be that if they encounter
rejection or hostility from the majority society, young
people may immerse themselves in more traditional
aspects of their parental culture (Cashmore, 1979).
Stigma and shame may be experienced as a result of
culturally specific expectations of physical appearance.
Early research found that, in initial encounters,
people with a disfigurement are more likely to be
negatively evaluated than physically attractive people.
They may be judged to be less intelligent, less sociable,
less morally upright, less likely to hold high-status
jobs, and less likely to have good marriages (Rumsey
et al, 1982, 1986). A study of interpersonal distance
while waiting at the kerbside and the effects of facial
appearance on seat occupancy on a suburban railway
showed that facial disfigurement can lead to negative
or avoidance reactions (Rumsey et al, 1982; Houston
and Bull, 1994). Stigmatisation may also lead to social
unacceptability and have an impact on the marriage
prospects of those living with neurofibromatosis (NF1)
among the British Bangladeshi community (Rozario,
2007). Explanations for the behaviour of others have
been explored, and have included beliefs about a just
world, an evolutionary aversion to anything other
than perfect, and the desire to avoid anything that
might be contagious (Rumsey and Harcourt, 2004).
In any society, religion exerts powerful influences
on personal perceptions, attitudes and beliefs with
regard to healthcare, and shapes the models of care
that patients receive (McAuley et al, 2000; Rassool,
2000). Concepts of God play a major role in health
belief systems, which constitute a holistic framework
that meets the physical, spiritual and psychosocial
needs of individuals and communities (Ypinazar and
Margolis, 2006). For example, concepts of the origins,
nature, cause and consequences of health and disease
appear to be heavily influenced by strong connections
to Islam and its traditional culture (Atiyeh et al, 2008). Strauss (1985) noted that, in Israel, western Jews,
oriental Jews and Arabs differ in their explanations
of the origins of birth defects, and their approaches to
rehabilitation and community integration.
Therefore a disfigurement, whether congenital, present
at birth or acquired later in life, may have a
profound impact upon the individual and their family
(Rumsey and Harcourt, 2004). The psychological and
social consequences of living with a disfigurement,
and the individual’s experience of being visibly different,
are well documented (Lansdown et al, 1997; Rumsey
and Harcourt, 2005). For the individual concerned, it
may adversely affect body image, quality of life and
self-esteem, as well as social interaction (Bull and
Rumsey, 1988). There is some evidence to suggest that
those of ‘non-white’ ethnic origin worry more about
the appearance of their condition and report that their
appearance affects their lifestyle more than similar
white counterparts (Rumsey et al, 2004). However, it
is unclear whether South Asian communities in the
UK respond and react to individuals with a disfigurement
in the same way as themajority white community.
Research and observations from clinical practice
have shown that the severity of a disfigurement is not
an accurate predictor of distress or psychological
adjustment, but is more likely to be influenced by a
complex mix of physical, psychosocial and cultural
factors (Clarke and Cooper, 2001). Although many
people find it difficult to cope with a disfigurement,
others appear to be relatively unaffected and seek little
or no psychosocial support. Anecdotal evidence from
the NHS strongly suggests that the uptake of support
for people who have a disfigurement differs between
cultural groups, and is very low among Asian and
minority groups. Although most Muslims appreciate
modern medicine and seek healthcare, the belief in
predestination and that illness is a test from God may
mean that some patients do not seek treatment (Lawrence
and Rozmus, 2001). However, a recent ruling has made
it clear that surgery to reshape a deformed part of the
body is generally recommended in Islam (Al Jazeera
Publishing, 2009). Notably, there is evidence to suggest
that, as in the western world, aesthetic surgery is spreading
fast in Muslim countries (Atiyeh et al, 2008).
Scholars argue that surgery for the purpose of beautification
is the result of the materialistic pattern followed
by western civilisation and of standards set by
Hollywood (Atiyeh et al, 2008).
However, the nuances of cultural and social differences
in responses to visible birth anomalies and acquired
differences remain largely under-researched (Rumsey
and Harcourt, 2004). The aim of the present study was
to explore South Asian community attitudes towards
beauty and disfigurement as well as the acceptance of
medical intervention and access to support for individuals
with a disfigurement.
Methods
The research was undertaken between 2007 and 2008.
Ethical approval was obtained from the Biomedical
Research Ethics Committee at the University of
Warwick. The aim of this exploratory research project
was to elicit the views of selected British South Asian
communities about issues of appearance and disfigurement,
and perceptions of and the relevance of
medical treatments. While it was acknowledged that
achieving a fully representative sample of all South
Asian sub-groupings was problematic, attempts were
made to include people from distinct South Asian
communities characterised by their religious, linguistic
and ethnic attributes, in particular Bangladeshi (Bengalispeaking
Muslim), Indian (Gujarati-speaking Hindu
and Punjabi-speaking Sikh) and Pakistani (Urduspeaking
Muslim).
The research methodology drew upon the Social
Action Research Model, which has been extensively
used to explore the perceptions and understandings of
ethnic minority communities, particularly in relation
to South Asian health beliefs (see, for example, Culley
et al, 2007; Lloyd et al, 2008; Johnson and Borde,
2009). Volunteers from within the South Asian communities
were provided with quality training in aspects
of social research facilitation and the issue of
concern (i.e. concepts of appearance and disfigurement).
In order to maximise participation and enhance
linguistic and cultural sensitivity, two male and
two female bilingual South Asian facilitators were
recruited from the West Midlands region. The facilitators
recruited natural groupings from within their
specific South Asian communities, and led the focus
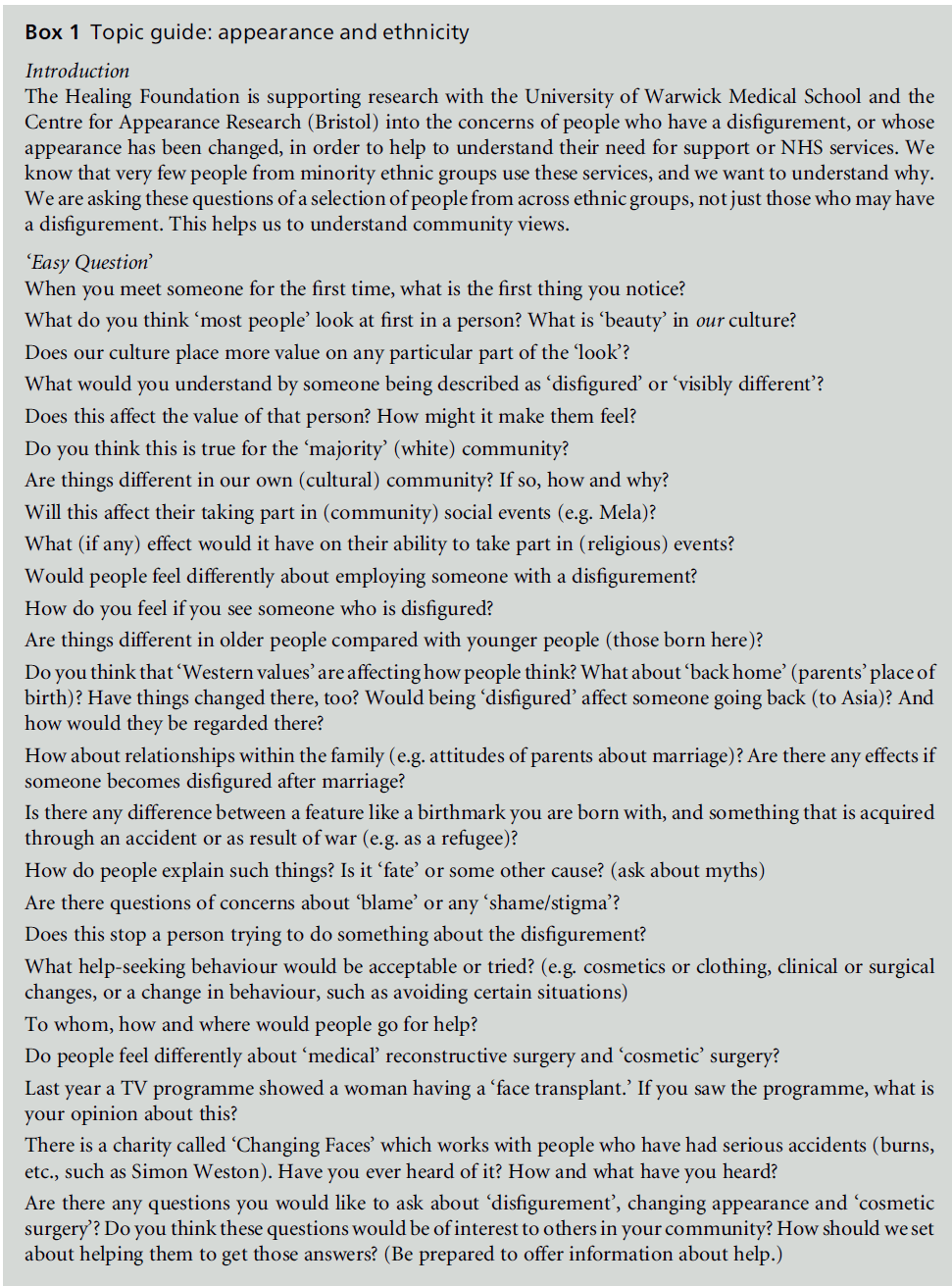
group discussions, following an agreed semi-structured
topic guide, which they helped to develop in consultation
with the research team (see Box 1).
Data were collected in the West Midlands region of
England. Nine single-sex focus groups were established
with South Asian community members (n = 63). The
facilitators approached participants opportunistically
in community settings, including places of worship
and community groups. They were allocated to groupings
according to their religious and ethnic identities,
gender and age. Five focus groups were conducted
with women (n = 34) and four with men (n = 29), and
the age range of participants was 18–70 years (see
Table 1). In total, 16 participants self-ascribed their
ethnicity as Bangladeshi, 35 as Indian and 12 as
Pakistani. The Bangladeshi and Pakistani groups were
all Muslim, and the Indian groups described their
religion as Hindu (n = 18) or Sikh (n = 17). The focus
groups were conducted in the preferred languages of
the participants (English, Bengali, Gujarati, Punjabi or
Urdu). Five discussions were tape-recorded and fully
transcribed by the facilitators. Four discussions were recorded in notes compiled by the facilitators during
the focus group sessions. These were translated into
English by the bilingual facilitators. The facilitators
were asked to use their discretion and judge whether
or not it would be acceptable to the participants to
tape record the discussion.
The data were analysed by a team of four analysts
using a process of template analysis (Kent, 2000). A
priori themes were initially defined. Initial coding of
the data was then carried out, identifying those parts
of the transcripts that were relevant to the research
aims. If encompassed by one of the a priori themes, a
code was allocated to the identified section. If there
was no relevant theme, an existing theme was modified
or a new one was created. The identified themes
in the selected transcripts were then grouped into a
smaller number of higher-order codes which described
broader themes in the data. This template was then
applied to the full data set. A group session with all
study teammembers, including the bilingual facilitators,
provided a forum in which the themes were discussed
before the final analysis was accepted and completed.
In the findings section that follows, key themes that
emerged from the data are presented together with a
discussion of the interrelated sub-themes that they
encompass.
Findings
The analysis identified eight key themes relating to
South Asian community views about disfigurement,
namely definitions and meanings, causation, family,
social and emotional reactions, social exposure, cultural
differences, medical interventions, and social
support.
Definitions and meanings
Arange of descriptions and definitions associated with
disfigurements were offered by the groups when the
topic of disfigurement was introduced. These ranged
from ‘ugly’ to any abnormality or unevenness in the
colour, shape or features of the face, including scarring
and birthmarks. Older male participants discussed
nicknames given to people with a disfigurement, and
mentioned amputation and problems with the eyes as
disfigurements. Some definitions related to what was
regarded as beautiful in Asian culture, and also to what
God had created. Clear, fair skin, a nice nose and eyes
were features that were prized and valued by many
respondents. For example:
‘In our culture beauty depends on how beautiful
someone’s face is.’
(older Bengali man)
‘Perfect nose, eyes, slim.’
(older Pakistani woman)
‘Beauty can be a number of things: beard, moustache, hat,
clothes.’
(young Bengali man)
‘Allah makes so many things which are beautiful.’
(older Bengali man)
Although the emphasis was on facial features such as
symmetry, it was acknowledged by both men and
women that beauty is subjective and can come from within. Several respondents associated a disfigurement
with a physical disability such as being deaf or
wheelchair bound. Other respondents linked an external
disfigurement with an individual’s intellectual
capabilities, or used it to make a judgement about a
person’s character (the latter was particularly likely if
the disfigurement looked as if it might have resulted
from an accident or fight). For example:
Table 1: Focus group composition
‘You always make the assumption that they are not as
capable as normal people.’
(young Bengali woman)
‘If their appearance is not normal you can surmise that
they are not well.’
(older Sikh man)
‘If some have [a] disfigured face, this person is not normal
mentally.’
(older Bengali man)
‘If it is due to an accident or fight, people may blame him
for his bad character.’
(young Bengali man)
It is interesting to note the absence of any discussion
of body shape, height or size, which tends to be an
important aspect of the framing of meaning and the
definition of beauty in white British culture. However,
there is some indication that this situation is changing
among young South Asian women and girls, particularly
in relation to the impact of contemporary media
representations of beauty in both UK and Asian
cultures.
Causation
The participants offered a number of explanations for
the origins of disfigurement, and in most cases these explanations were based on religious belief or cultural
myth. There was a sense of fatalistic acceptance, with
disfigurement being described as thewill of the creator
and sustainer of the world, and a belief that it should
be accepted as such. This was the predominant causal
explanation across the different religious groups,
although some respondents regarded a disfigurement
as one’s destiny or a test, and others regarded it as the
result of sin. For example:
‘I feel sad, but what can we do, this is Allah’s wish.’
(young Bengali man)
‘First we would have to accept it as God’s will ... I would
accept it as my fate and destiny.’
(older Sikh man)
‘Some people would say it’s a test from God to see how
that person copes with it.’
(young Pakistani woman)
‘This was God’s way of punishing you.’
(young Bengali woman)
Respondents mentioned that some people in their
culture may attribute the origins of a disfigurement to
cultural myths. Participants talked of a disfigurement
being attributed to engaging in sexual activity during
pregnancy, or the result of making fun of someone
with a disfigurement. The superstitious avoidance of
people with a disfigurement, just in case the condition
was infectious, was also mentioned. Examples of such
beliefs included the following:
‘There is a common superstition about pregnant women
during the lunar eclipse.’
(older Bengali woman)
‘You made fun of someone with a disfigurement many
years ago, and now it’s come back on to you.’
(young Pakistani woman)
‘There are stories in our religion about these (MEATH)
too. Therefore we are scared of these people. Do not go to
these people.’
(older Bengali man)
The notion of individual culpability was discussed, as
it was thought that the individual’s past or present
actions could be the reason for their difference. For
example, they could have been involved in a fight or an
accident, and some respondents spoke of this as the
result of karma (an action or attitude in their previous
life). Alternatively, others mentioned that a mother
could be to blame for her past or present actions, which
resulted in her bearing a visibly different child. For
example:
‘[if he is] disfigured due to an accident or fighting, people
may blame him.’
(young Bengali man)
‘People are so suspicious of how come all of a sudden this
has happened to your child or what were they doing so
bad that this has happened to them.’
(older Pakistani woman)
‘That child is paying for their karma.’
(older Sikh man)
‘The fathers along with the in-laws blame the mother.’
(older Bengali woman)
Some respondents articulated a more medical interpretation
of disfigurement. It was acknowledged that
genetics sometimes played a role, and that disfigurements
could be inherited. This suggests that the influence
of religious explanations might be weakening, although
traditional beliefs still dominated the discussion.
Family
The groups spoke of an overall sense of burden and
shame that would be felt by the family of someone
with a visible difference. The family would wish to
limit the amount of public exposure of the affected
person, who would be regarded as a source of embarrassment
and perhaps even suspicion. For example:
‘They tend to hide them away because they see it as kind of
a shameful and embarrassing thing.’
(young Bengali woman)
However, there was some indication that the South Asian
community is becoming more tolerant. For example:
‘A friend I know has a disabled sibling and they are not as
ashamed. People are becoming more tolerant.’
(young Bengali woman)
In addition, relatives would feel a sense of responsibility
to care for an individual with a disfigurement,
although this would be seen as a burden, especially if
the person affected was a girl. For example:
‘The disfigured female in the family is terribly embarrassing.’
(older Bengali woman)
Families would be more accepting of a disfigured boy
who could earn money. The importance of gender was
also apparent when the groups discussed marriage. It
was believed, especially by younger participants, that
having a disfigurement had a negative impact on marriage
prospects, especially those of a girl. For example:
‘I think parents would be worried about their child’s
marriage if their child was disfigured.’
(young Pakistani woman)
‘You are choosing the father or mother of your child ...
they will not go for personality, they go for looks first.’
(young Bengali woman)
‘It would affect their chances of getting married.’
(young Pakistani man)
The family is still a key social unit that replicates
behaviours which are based upon feelings of shame.
Therefore the individual who has a disfigurement is
hidden from everyday social interaction. The interesting
consequence of this restricted public exposure is
the reduced opportunity for the affected person to
explore alternative and more accepting cultural settings
or support mechanisms. As another theme below
suggests, the only outlet tends to be within a context of
religious practice. Thus the individual is isolated from
more tolerant communities, and may be unable to
ameliorate their negative experiences as a result of
what may be a form of collective collusion to avoid
embarrassment.
Social and emotional reactions
Several participants discussed how they would react
upon seeing an individual with a disfigurement. Some
respondents said that they would feel shocked or
frightened. For example:
‘You might get a shock and it can make you jump.’
(young Pakistani man)
Older participants spoke of myths and religious tales.
For example:
‘There are stories in our religion about these people.
Therefore we are scared of these people.’
(older Bengali man)
In addition, a few respondents mentioned stigmatising
language used in their culture to refer to individuals
with a disfigurement. For example:
‘Even I feel scared sitting next to a disfigured person on the
bus.’
(older Bengali woman)
However, the majority of the respondents spoke of a
sense of sorrow and sympathy, and expressed the view
that they would not wish to make the person feel
uncomfortable. Acts of over-compensation were discussed,
as it was felt that individuals with visible
differences should be protected from harm and so
the community would be nicer to them. The concept
of Sewa, or selfless service, the notion of doing something
resulting in benefit to others, was also mentioned.
For example:
‘Sometimes we feel sorry for these people.’
(older Bengali man)
‘If I see such a person I feel very sad. I want these people to
be treated the same as others.’
(young Bengali man)
It was widely believed that a disfigurement could have
a negative impact on the psychological well-being of
an individual. It was thought that the person may feel
marginalised and lonely, or suffer from low self-esteem.
This could be as a result of keeping themselves out of
the public eye, or due to the actions of others in the
community. For example:
‘They will lack confidence. They might be isolated by
others but they will also isolate themselves.’
(young Pakistani woman)
‘They would probably lose the will to live.’
(young Pakistani man)
‘When he looks in the mirror he might feel different,
weak.’
(young Bengali man)
The social and emotional reactions of participants
offered some amelioration of the strong sense of
shame and stigmatisation associated with disfigurement.
A willingness to advocate medical intervention
was also evident. The responses reflected the expectation
that individuals with a disfigurement would
react to community attitudes towards them, experiencing
low self-esteem and self-imposed isolation.
This was thought to lead to subsequent marginalisation
bothwithin their owncommunity and in relation
to the wider UK social environment where support is
available.
Social exposure
Participants thought that the community or family
would try to limit the public exposure of an individual
with a disfigurement in several ways. The family might
attempt to do this as a form of protection as well as in
response to a sense of shame. For example:
‘We would not take them out much because people would
stare.’
(older Sikh man)
‘They are considered a social outcast.’
(older Bengali woman)
‘I think other people would make it difficult for them to
socialise.’
(young Pakistani woman)
There was a clear differentiation between an individual
with a disfigurement being accepted in a religious
gathering, and attitudes towards them in situations
outside this context. When attending religious ceremonies,
people would be more open minded because
everyone should be able to come to worship. For
example:
‘Religious events will not affect them as much, in places
like that people would be more sympathetic.’
(young Bengali woman)
‘We tend to be soft hearted in religious events. So people
are more broad minded.’
(older Bengali woman)
It was also felt that an individual with a disfigurement
would have reduced employment opportunities, and
might feel pressured by society to keep him- or herself
out of the public eye. For example:
‘[An] employer will not employ someone who will make
the children or customer afraid.’
(older Bengali woman)
‘You will find you are stuck in the corner somewhere.’
(young Bengali woman)
Participants thought that an individual with a disfigurement
would find it difficult to socialise and to
take part in events outside the religious context. Some
participants also discussed the use of traditional clothing
and make-up to conceal a disfigurement. For example:
‘Some disguise them with clothing. ... Some would hide
themselves from social gatherings.’
(older Bengali woman)
The comments expressed here are, once again, culturally
bounded and self-referential, since they do not
encompass the possibility of alternative experiences for the affected individual outside their immediate
community setting. Despite greater religious tolerance
in specific contexts, the dominant view was that the
appropriate treatment of disfigured individuals is
concealment. This raises questions about community
awareness of both the well-being of the individual and
the issues to be considered when developing interventions.
Cultural differences
A number of differences between South Asian and
western white cultures were observed. It was widely
felt that the western media dictates what is beautiful,
and does not show images of people with a disfigurement
unless the context is medical, or in order to sell
products. However, several participants remarked
that white western families were better educated and
more accepting of disfigurements than Asian families.
This supports other themes discussed above which
indicate that gradual cultural shifts may be occurring
within the South Asian community as they become
more aware of the wider UK socio-cultural environment
and consider alternative views of disfigurement.
For example:
‘Their community [white] is more aware, exposed and
educated about differences.’
(young Pakistani woman)
‘They [white people] are more accepting ... they even
encourage disfigured people to blend in with the mainstream
society.’
(older Bengali woman)
‘As the lifestyle of both Bangladeshi and English is
different, this issue is different too. They [English] treat
the disabled people with respect.’
(young Bengali man)
The differences noted between the cultures were also
influenced by age. Younger participants commented
that elders are considered to be narrow-minded and
less understanding. This was evidenced by the fact that
skin colour is particularly important to elders, but less
so to younger people. For example:
‘We [young people] understand how things work now,
how society is, whereas they [older people] are stuck in
their own times.’
(young Pakistani man)
It was also mentioned that attitudes in communities
back home differed, and that people there would be
more tolerant of disfigurements than communities in
the UK.
The influence of Bollywood, the Indian film industry,
which is largely based in Bombay, was raised, and
the belief was expressed that South Asian attitudes are
becoming more aligned with western culture in terms of the importance attached to physical beauty. For
example:
‘With the influence of Bollywood, girls want to look more
glamorous and I don’t think it matters any more if they
got a good personality or what sort of person you are.’
(older Pakistani woman)
‘People are more conscious about the way they look these
days ... so imagine having a disability – that is a huge thing
now.’
(young Bengali woman)
‘The media puts too much on people to look a certain way.
You never see a disfigured person on TV.’
(young Pakistani woman)
These comments suggest that the definition and
framing of beauty are changing under the influence
of British and Bollywood cultural artefacts, especially
in the media. In this respect, the concept of beauty is
becoming broader. Glamour is the focus, rather than
just the face. However, it also places greater emphasis
on appearance, and compounds the issue of conformity
to a contemporary stereotype for those with a
disfigurement.
Medical intervention
Medical intervention was considered acceptable by all
groups if it was necessary for a medical reason and it
was considered important to follow the advice of a
doctor. It was widely thought that an individual should
pursue treatment for a disfigurement, as it would
improve their quality of life. However, non-essential
or cosmetic surgery, pursued out of vanity, was not
condoned. Numerous participants deemed cosmetic
surgery to be playing God and going against God’s
will. A few participants stated that a person’s character
was linked to their physical appearance, and so one
should not try to change the way that one looks. For
example:
‘It is a great sin to try to change the way of looks. Allah will
punish them.’
(older Bengali woman)
‘Some people would say it’s playing God.’
(young Pakistani woman)
‘Medical is necessary, and cosmetic, that is a luxury.’
(young Bengali woman)
The medically acknowledged need for intervention
was still qualified by traditionally held beliefs about
divine retribution, although this was more likely to be
asserted by elders in the community. However, it was
widely articulated that remedies that can be rationalised
as medically necessary could also affect mental
health and quality of life in the community through increased opportunities for social exposure and betterquality
social interaction. For example:
‘If someone’s life is being drastically affected because of a
disfigurement, such as marriage proposals, then they
should take whatever reasonable means necessary.’
(young Pakistani woman)
Social support
The participants agreed that the immediate family
is the main source of support, and that shame or
embarrassment may prevent families from seeking
support from external sources. Families may be reluctant
to ask their extended family or their community
for help with a relative with a disfigurement. Therewas
a general lack of awareness of the support services
available to individuals with a disfigurement. For
example, none of the participants had heard of the
charity Changing Faces.
‘The extended family stay uninvolved either due to lack of
awareness, shame, or ‘just can’t be bothered’ attitude.’
(young Pakistani man)
‘They would definitely not go to the community ... they
might go to the doctors rather than ask family.’
(young Bengali woman)
In several ways, this theme provides a canvas for many
of the findings. The extended family is the major
element of the social and cultural infrastructure that
both embodies the beliefs, myths and stereotypes
about disfigurement and dictates behaviours towards
visibly different relatives. The family mediates a range
of culturally significant attitudes towards disfigurement
that comprise, among other things, shame and
the process of stigmatisation, the concept of acceptable
appearance, concealment of visible difference,
and burden and suffering due to divine retribution.
The gradual shift in cultural orientation by younger
members of the South Asian community, especially
women, does indicate that family dynamics may be
changing. However, the lack of awareness of support
opportunities and the limitation of public exposure
imposed upon, and self-imposed, by those affected
prevents them from seeking external social support.
Discussion
The focus group discussions revealed the value attributed
to physical appearance in South Asian culture.
Furthermore, it emerged that people with a disfigurement
are more likely to be negatively evaluated than
those who do not have a visible difference. Some respondents linked an external visible difference with
an individual’s intellectual capabilities, or used it to
make a judgement about a person’s character. Those
who have a disfigurement may be judged as ‘second
class’, and may perhaps be perceived as having ‘some
form of psychological disorder’ (Rumsey and Harcourt,
2005, p. 12). The participants also thought that a sense
of stigma and shame would be felt by an individual
with a disfigurement, and that they might feel obliged
to limit their presence in the community, as reported
in previous studies (Gaff and Clarke, 2007). This would
also limit their opportunities to access an alternative
cultural referent from a wider social group, or for the
affected person to be pro-active in seeking support.
Discussions also focused on the ways in which
appearance played a central role in a person’s life
chances as well as their general well-being and levels
of participation in the community. The findings
support earlier research which found that attractive
and non-disfigured people are favoured in a wide
variety of situations, including dating, marriage, education
and employment (Bull and Rumsey, 1988). The
continuing custom whereby the parents arrange the
marriage of their child introduces a further dimension
in relation to restricted opportunitieswithin and beyond
the community. The view was widely expressed that a
disfigurement would have a negative impact on an
individual’smarriage prospects, particularly for females.
This finding supports the results of previous research
that explored social acceptance and marriage in nonwhite
communities (Rozario, 2007).
Faith and spirituality are increasingly recognised as
playing an important role in people’s understanding
of illness, in support and coping, and in clinical care
(Lambert and Sevak, 1996; Koenig et al, 2001). The
findings of the present study show that religious and
cultural beliefs cut across the majority of the themes
that emerged, and were particularly implicated in
beliefs about the causation and consequences of disfigurement.
Some older participants felt that it was the
result of a sin or that it was a test by God, and so the
individual must accept it as their destiny. The findings
add to the literature which shows that God plays a
major role in health belief systems (McAuley et al,
2000; Rassool, 2000). However, it was widely thought
that an individual should seek medical help for a
disfigurement so long as this was not motivated by
vanity (as this would be regarded as against the will of
God). The findings support evidence from Muslim
communities that medical intervention is accepted in
Islam so long as it is undertaken for the benefit of the
patient (Atiyeh et al, 2008).
Most of the participants felt that white western
people appeared to be more educated about and
accommodating towards individuals with a disfigurement.
This was also the perception of the treatment of
a Bangladeshi woman with NF1 in the UK (Rozario, 2007). In addition, a number of groups felt that there
was cultural and generational disparity in beliefs in
relation to understanding and accepting disfigurements.
Younger South Asians regarded their elders as having
outdated views and as being more narrow-minded
than themselves (see, for example, Papastergiadis,
1998). There was also a sense that South Asian community
views were becoming more aligned with western
values, due to high levels of social interaction. The
influence of Bollywood and changes in society back
home were also considered to be significant influences
on the attitudes of communities in the UK. Therefore
it may be that South Asian communities will become
progressively more accepting of visible disfigurement,
while at the same time being influenced by the pervasive
images of beauty and physical perfection promoted by
the media.
In the light of these findings, an important next step
is to develop appropriate information about the causes
and consequences of disfigurement, and to devise
effective dissemination strategies. The participants
identified a number of foci for information and interventions
that might reduce the negative consequences
of disfigurement. These included education to dispel
myths, raising awareness of sources of support, and
the provision of authoritative medical explanations
for disfigurements.Members of the Bengali community
were particularly keen to express their suggestions for
interventions to improve the experiences of those with
visible differences. They identified the need to dispel
myths about fetal disorders, and suggested that women’s
groups could be useful platforms for educating the
community. They also felt that community-specific
health sessions should be arranged to raise awareness,
and that local government agencies could become
more involved in this.
Limitations of the study
Focus groups are an invaluable research method for
working in a diverse linguistic and cultural environment,
and can provide rich data (Culley et al, 2007).
We have highlighted community responses to disfigurement,
and how people collectively construct meanings
which may have been more difficult to discern via
individual interviews (Waterton and Wynne, 1999).
However, the use of focus groups has limitations and
methodological implications, such as the possibility of
group effects (Carey and Smith, 1994). We were also
keen to collaborate with our facilitators when designing
the study, in order to facilitate research with as
opposed to research on minority ethnic communities
(Johnson, 2006). The facilitators were given the freedom
to interpret the topic guide to suit their focus
group characteristics, and some of them made detailed
notes throughout the group session as opposed to recording the discussion and transcribing it verbatim,
although all of them had, and used, tape recorders to
provide them with an aide-memoire of the discussion.
This may be seen as a lack of rigour, but this approach
was advised by the facilitators as they regarded it as a
culturally sensitive approach in view of the characteristics
of their focus group participants. Since all of the
discussions were at least partly conducted in languages
other than English, and language switching was common,
we had to rely on the skill and interpretation
of these bilingual colleagues to understand the data.
Equally, it was proposed that this enabled the facilitators
to contextualise the data and to provide a richer
insight into the groups’ response to what might be
regarded as a contentious topic of discussion. Finally,
there are variations in the belief systems of South
Asian communities that place different emphases on
the role of fate and retribution ascribed to their
preferred deity. It was not possible to explore these
more subtle aspects of the participating communities
to inform the intervention strategies indicated.
Conclusion
This study offers a unique insight into the views held
by South Asian communities in the UK in relation to
how disfigurement and beauty are perceived, and it
adds to the growing body of literature on disfigurement
and the psychology of appearance. The findings
suggest that there is a change in the orientation of
younger members of the community from traditional
religiously framed perceptions of acceptable appearance,
to advocating a more informed and aware
attitude to the causes and consequences of disfigurement.
Evidence of generational differences in South
Asian community views appears to emerge from
westernisation and the influence of the media. The
findings provide a basis from which to develop educational
interventions to highlight the support services
available, and also to dispel myths which may
pose barriers to communities accepting and supporting
individuals with a disfigurement.
Acknowledgment
This paper is presented on behalf of the Appearance
Research Collaboration. This research was supported
by a grant to the Appearance Research Collaboration
from the Healing Foundation and the Welton Foundation.
CONFLICTS OF INTEREST
None.
References
- Adamson P and Doud Galli S (2009) Modern concepts of beauty. Plastic Surgical Nursing 29:5ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â9.
- AfsharH(1994) Muslim women in West Yorkshire: growing up with real and imaginary values amidst conflicting views of self and society. In: Afshar H and Maynard M (eds) The Dynamics of ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âRaceÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ and Gender. London: Taylor and Francis, pp. 127ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â47.
- Al Jazeera Publishing. Ruling on Cosmetic Surgery; www. islamonline.com (accessed 10 August 2009).
- Anwar M (1998) Between Cultures: continuity and change in the lives of young Asians. London: Routledge.
- Atiyeh B, Kadry M, Hayek SN et al (2008) Aesthetic surgery and religion: Islamic law perspective. Aesthetic Plastic Surgery 32:1ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â10.
- Bull R and Rumsey N (1988) The Social Psychology of Facial Appearance. New York: Springer-Verlag.
- CareyMAand SmithMW(1994) Capturing the group effect in focus groups: a special concern analysis. Qualitative Health Research 4:123ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â7.
- Cashmore E (1979) Rastaman: Rastafarian Movement in England. London: Allen & Unwin.
- Clarke A and Cooper C (2001) Psychological rehabilitation after disfiguring injury or disease: investigating the training needs of specialist nurses. Journal of Advanced Nursing 34:18ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â26.
- Culley L, Hudson N and Rapport F (2007) Using focus groups with minority ethnic communities: researching infertility in British South Asian communities. Qualitative Health Research 17:102ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â12.
- Drury B (1991) Sikh girls and the maintenance of ethnic culture. New Community 17: 387ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â99.
- Etcoff NL (1994) Psychology. Beauty and the beholder. Nature 368:186ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â7.
- Gaff C and Clarke A (2007) Stigmatization, culture and counseling. A commentary on growing up and living with NF1: a UKÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
âBangladeshi case study by Santi Rozario. Journal of Genetic Counseling 16:561ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â5.
- Haiken E (2000) The making of the modern face: cosmetic surgery. Social Research 67:81ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â98.
- Houston Vand Bull R (1994) Do people avoid sitting next to someone who is facially disfigured? European Journal of Social Psychology 24:279ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â84.
- Johnson MRD (2006) Engaging communities and users: health and social care research with ethnic minority communities. In: Nazroo JY (ed) Health and Social Research in Multiethnic Societies. London: Routledge, pp. 48ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â64.
- Johnson MRD and Borde T (2009) Representation of ethnic minorities in research ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â necessity, opportunity and adverse effects. In: Culley L, HudsonNand van Rooij F (eds) Marginalized Reproduction: ethnicity, infertility and reproductive technologies. London: Earthscan, pp. 64ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â80.
- KentG(2000) Understanding the experiences of people with disfigurements: an integration of four models of social and psychological functioning. Psychology, Health and Medicine 5:117ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â29.
- Koenig HG, McCullough ME and Larson DB (2001) Handbook of Religion and Health. New York: Oxford University Press.
- Lambert H and Sevak L (1996) Is ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âcultural differenceÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ a useful concept? Perceptions of health and the sources of ill health among Londoners of South Asian origin. In: Kelleher D and Hiller S (eds) Researching Cultural Differences in Health. London: Routledge, pp. 358ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â61.
- Langlois JH, Ritter JM, Roggman LA et al (1991) Facial diversity and infant preferences for attractive faces. Developmental Psychology 27:79ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â84.
- Lansdown R, Rumsey N, Bradbury E et al (1997) Visibly Different: coping with disfigurement. London: Butterworth- Heinemann.
- Lawrence P and RozmusC(2001) Culturally sensitive care of the Muslim patient. Journal of Transcultural Nursing 12:228ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â33.
- Lloyd C, Johnson M, Stuart J et al (2008) Hearing the voices of service users: reflections on researching the views of people from South Asian backgrounds. In: Williamson A and DeSouza R (eds) Researching with Communities: grounded perspectives on engaging communities in research. Auckland, New Zealand: Muddy Creek Press, pp. 178ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â99.
- McAuley J, Pecchioni L and Grant J (2000) Personal accounts of the role of God in health and illness among older rural African American and White residents. Journal of Cross-Cultural Gerontology 15:13ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â35.
- Marquardt SR (2002) Dr Stephen Marquardt on the Golden Decagon and human facial beauty. Journal of Clinical Orthodontics 36:339ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â47.
- Modood T, Beishon S and Virdee S (1994) Changing Ethnic Identities. London: Policy Studies Institute.
- Papadopoulos L, Bor R and Legg C (1999) Coping with the effects of vitiligo: a preliminary investigation into the effects of cognitiveÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
âbehavioural therapy. British Journal of Medical Psychology 72:385ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â96.
- PapastergiadisN(1998) Dialogues in the Diaspora: essays and conversations on cultural identity. London: Rivers Oram Press.
- Poran MA (2002) Denying diversity: perceptions of beauty and social comparison processes among Latina, Black, and White women. Sex Roles 47:65ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â81.
- Rassool GH (2000) The crescent and Islam: healing, nursing and the spiritual dimension: some considerations towards an understanding of the Islamic perspectives on caring. Journal of Advanced Nursing 32:1476ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â84.
- Rex J (1991) Ethnic Identity and Ethnic Mobilisation in Britain. Coventry: Warwick Centre for Research in Ethnic Relations.
- Rhodes G (2006) The evolutionary psychology of facial beauty. Annual Review of Psychology 57:199ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â205.
- Rozario S (2007) Growing up and living with neurofibromatosis 1 (NF1): a British Bangladeshi case study. Journal of Genetic Counselling 16:551ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â9.
- Rumsey and Harcourt (2004) Body image and disfigurement: issues and interventions. Body Image 1:83ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â97.
- Rumsey N and Harcourt D (2005) The Psychology of Appearance. Buckingham: Open University Press.
- Rumsey N, Bull R and Gahagen D (1982) The effect of facial disfigurement on the proxemic behaviour of the general public. Journal of Applied Social Psychology 12:137ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â50.
- Rumsey N, Bull R and Gahagen D (1986) A preliminary study of the potential of social skills for improving the quality of social interaction of the facially disfigured. Social Behaviour 1:143ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â6.
- Rumsey N, Clarke A, White P et al (2004) Altered body image: appearance-related concerns of people with visible disfigurement. Journal of Advanced Nursing 48:443ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â53.
- Schjedhal P (1998) Notes on beauty. In: Beckley B and Shapiro D (eds) Uncontrollable Beauty: toward a new aesthetic. New York: Allworth Press. pp. 53ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â61.
- Strauss RP (1985) Culture, rehabilitation and facial birth defects: international case studies. Cleft Palate Journal 22:56ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â62.
- Swami V and ToveÃÆÃââââ¬Ã
¡ÃÆââ¬Å¡Ãâôe MJ (2007) Perceptions of female body weight and shape among indigenous and urban Europeans. Scandinavian Journal of Psychology 48:43ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â50.
- Waterton C and Wynne B (1999) Can focus groups access community views? In: Barbour R and Kitzinger J (eds) Developing Focus Group Research: politics, theory and practice. London: Sage, pp. 127ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â43.
- Ypinazar VA and Margolis SA (2006) Delivering culturally sensitive care: the perceptions of older Arabian Gulf Arabs concerning religion, health, and disease. Qualitative Health Research 16:773ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â87.


