Selma Sengiz Erhan1*, Aylin Ege Gul2, Sevinc Hallac Keser2, Seyfi Acar3 and Sibel Sensu4
1Department of Pathology, Okmeydani Education and Research Hospital, Istanbul, Turkey
2Department of Pathology, Dr. Lutfi Kirdar Kartal Education and Research Hospital, Istanbul, Turkey
3Department of Surgery, Fethiye State Hospital, Mugla, Turkey
4Agonist Health Care, Istanbul, Turkey
*Corresponding Author:
Selma Sengiz Erhan
Medical Doctor, Department of Pathology, Okmeydani Education and Research Hospital, Kaptanpasa Mah. Darulaceze Cad. No: 27 34384 Okmeydani-Sisli/Istanbul, Turkey
Tel: 02122217777
Fax: 02122217800
E-mail: selmaserhan@hotmail.com
Received date: February 15, 2016 Accepted date: March 22, 2016 Published date: March 25, 2016
Keywords
Ovarian tumors, Sex-cord tumors, Sex cord tumor with annular tubules
Introduction
Sex cord tumors with annular tubules (SCTAT) are first described by Scully [1]. They are rare tumors of the ovary which account for less than 1% of all sex cord stromal tumors [2]. One third of SCTAT are accompanied by Peutz-Jeghers syndrome (PJS) [3,4]. The cases with PJS are sligthly younger (average age, 27) than isolated cases (average age, 36) [2]. The tumor is extremely rarely found in pediatric patients [3-7]. Clinical diagnosis of SCTAT is very difficult and diagnosis is mostly made with pathological examination [7].
Case Report
Twelve years old female patient was admitted to emergency clinic with a sudden severe pain localized at right lower abdomen, nausea and vomiting. At abdominal ultrasound, ascites and an appendix of 5.8 cm. diameter were observed at right lower abdomen. Clinical history and examination did not reveal any significant finding. The patient was operated with a prediagnosis of acute abdomen (acute appendicitis?). Right adnex was 8 × 3 cm, torsioned and gangrenous. An appendectomy with right salpingoo-ophorectomy were performed. Macroscopically, at the cross-sections of 7 × 5 × 3 cm, gray-purple ovarian tissue; a nearly 6 × 5 cm regular bordered mass was observed which included millimetric white nodular foci and hemorrhagic changes (Figure 1).
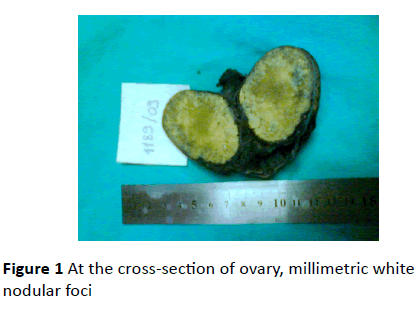
Figure 1 At the cross-section of ovary, millimetric white nodular foci
The surrounding ovarian tissue also included hemorrhagic areas. Sections of tuba and appendix did not reveal an abnormal feature. At histopathological examination; in fibrous stroma of the ovarian tissue, a tumoral area was observed which consisted of simple and complex tubular structures which had PAS positive hyaline material in the center surrounded by peripheral palisading cells (Figures 2 and 3).
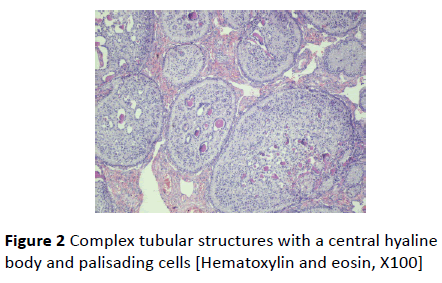
Figure 2 Complex tubular structures with a central hyaline body and palisading cells [Hematoxylin and eosin, X100]
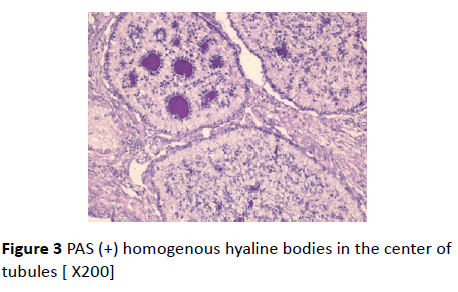
Figure 3 PAS (+) homogenous hyaline bodies in the center of tubules [ X200]
The cells had small single nuclei and wide pale cytoplasm. One mitotic figure was noted per 10 high power fields (HPF) and microc alcification was not observed. SCTAT, sertoli cell tumor, gonadoblastoma and microfollicular granulosa cell tumor were considered for differential diagnosis. Tumor cells were positively stained for inhibin, calretinin, vimentin and were negative for EMA, PLAP, laminin and CD117 (Figures 4 and 5).
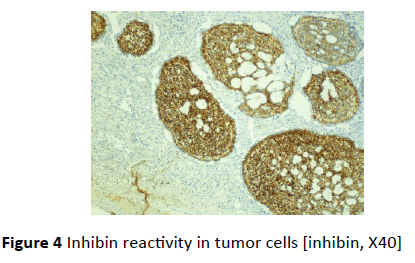
Figure 4 Inhibin reactivity in tumor cells [inhibin, X40]
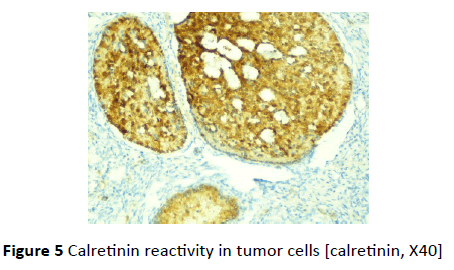
Figure 5 Calretinin reactivity in tumor cells [calretinin, X40]
It is distinguished from sertoli cell tumor because of complex tubules, from microfollicular granulosa cell tumor by dominance of hyaline bodies in tubules, and from gonadoblastoma by absence of germ cells. According to the findings, the case was diagnosed as ‘sex cord tumor with annular tubules (SCTAT)’. At postoperative period, since the patient did not come for routine follow up, a phone contact was made which revealed that she had no complaint during postop six years.
Discussion
Since SCTATs have common features with sertoli and granulosa cell tumors, they are classified as a subgroup of sex cord stromal tumors [2,3,8]. Due to hyperestrogenism, puberty precox in pediatric group, and menstrual irregularities as menometrorrhagia in reproductive age might be the clinical presentations of SCTAT. The tumor that is found incidentally in a case related with PJS may be accompanied with hyperpigmented macules in oral mucosa, gastrointestinal hamartomatous polyps and various tumors in genital system, breast and pancreas [2,3]. In preoperative examination and clinical history of our case, findings related with hyperestrogenism or PJS were not detected.
Sertoli cell tumor, gonadoblastoma and microfollicular granulosa cell tumor should be taken into account for differential diagnosis of SCTAT. Complex tubules are not seen in sertoli cell tumors. In microfollicular granulosa cell tumors, hyaline bodies in lumens of tubular structures are not very dominant, a feature important for differential diagnosis. In gonadoblastomas there are sex cord stromal elements and hyaline bodies, however a germ cell component and abnormal gonadal development (most often phenotypic females who are virilized) are seen contrary to SCTAT. In our case, in addition to histopathological findings, PLAP and CD 117 were negative and germ cells were not present [9].
Clinical behaviour and pathological features of the tumors differ according to the presence or absence of PJS. In cases with PSJ, bilateral, multiple and smaller (<3 cm) tumors with benign behaviour are observed. On the contrary, in cases without PJS, unilateral, bigger (as big as 33 cm) pelvic masses that may behave in a malignant behaviour, are detected [9]. On 20% of the cases without PJS, since malignancy and distant metastasis might be observed, these tumors are known to have low malignant potential. They may spread through pelvic, paraaortic and supraclavicular lymph nodes and metastasize to retroperitoneum, parietal and visceral peritoneum, liver, kidney and lung [9,10].
Malignant potential of the tumor may not be recognized microscopically [10]. However, in literature, there are studies reporting that more than 3-4 mitosis in 10 HPF and infiltrative growth pattern are related with aggressive behaviour [9]. In the case presented here, there wasn’t any finding in favour of malignancy. In postoperative period, the patient did not come for routine follow up, but a phone contact could be made. Accordingly, it was apperent that no complaint was present in a period of postop 6 years.
In literature search there are found reports including mostly a single case and a very few large study groups. So, currently, there are no widely accepted standard treatment protocols. In unilateral tumors, ipsilateral pelvic and paraaortic lymphadenectomy and unilateral salpingo-oophorectomy are the recommended therapy for young patients [9]. In cases with PJS, even if the tumor is present in only one ovary, wedge resection is recommended for the other ovary. Even though the effect is not clear, chemotherapy and radiotherapy are performed for local recurrence and distant metastasis [7].
Long term follow up is mandatory for SCTATs which have relatively good prognosis despite high recurrence risk [7].
Conclusion
The case presented here which is found incidentally in absence of a PJS is worth attention especially because of its pediatric age.
References
- Scully RE (1970) Sex cord tumor with annular tubules: a distinctive ovarian tumor of the Peutz-Jeghers syndrome. Cancer 25: 1107-1121.
- Zaloudek CJ, Mooney EE, Staats PN, Young RH (2014) Sex cord-stromal tumours - pure sex cord tumours. In: Kurman RJ, Carcangiu ML, Herrington CS, Young RH (Eds.). WHO classification of tumours of female reproductive organs 50-53.
- Young RH, Welch WR Dickerson GR, Scully RE (1982) Ovarian sex cord tumor with annular tubules: Review of 74 cases including 27 with P-J syndrome and four with adenoma malignum of cervix.Cancer 50: 1384-1402.
- Nosov V, Park S, Rao J, Memarzadeh S (2009) Non-Peutz-Jeghers syndrome associated ovarian sex cord tumor with annular tubules: a case report. Fertility and Sterility 92: 1497e5-1497e8.
- Ghribi A, Ben AS, Gasmi M, Sghairoun N, Sahli S, et al. (2014) Ovarian sex cord tumor with annular tubules in children. La TunisieMedicale 92: 762-763.
- Singh M, Mandal S, Majumdar K (2014) Sex cord tumor with annular tubules: An incidental finding in an endometriotic cyst-the first known cooccurrence. Biomed Res Int 2014: 1-3.
- Qian Q, You Y, Yang J, Cao D, Zhu Z, et al (2015) Management and prognosis of patients with ovarian sex cord tumor with annular tubules: a retrospective study.BMC Cancer 15: 270.
- Crissman JD, Hart WR (1981) Ovarian sex cord tumors with annular tubules: An ultrastructural study of three cases. Am J Clin Pathol 75:11-17.
- Deavers MT, Oliva E, Nucci MR (2009) Sex-cord-stromal tumors of the ovary. In: Goldblum JR editor. Gynecologic Pathology 445-500.
- Lele SM, Sawh RN, Zaharopoulos P, Adesokan A, Smith M, et al (2000) Malignant ovarian sex cord tumor with annular tubules in a patient with Peutz-Jeghers syndrome: A case report. Mod Pathol 13: 466-470.

