Jan J De Waele*, Stijn I Blot
Intensive Care Unit, Ghent University Hospital. Ghent, Belgium
- *Corresponding Author:
- Jan J De Waele
Intensive Care Unit
Ghent University Hospital
De Pintelaan 185
9000 Ghent
Belgium
Tel +32-92.402.775
Fax +32-92.404.995
E-mail jan.dewaele@ugent.be
Received: June 1st, 2006 Accepted: June 2nd, 2006
Keywords
Diagnostic Imaging; Pancreas; Pancreatitis, Acute Necrotizing; Tomography, X-Ray Computed
Dear Sir:
We read with interest the paper by Gürleyik et al. [1] and the subsequent letter by Brestas and Dafni regarding the use of ROC curve analysis [2]. We fully agree with Dr. Brestas that ROC curve analysis should be used to report the true discriminative power of a test, and are impressed by the performance of the CT severity index in predicting severe disease which was reported in reply to this letter.
There is however another very important bias when using the CT severity index, as introduced by Balthazar et al. [3], to predict disease severity. When a test or score is used to predict a disease state, two crucial elements must be taken into account. Firstly, the disease state to be predicted is not (yet) present (otherwise it should not be a prognostic indicator), and secondly, the disease state to be predicted is not included in the score under study.
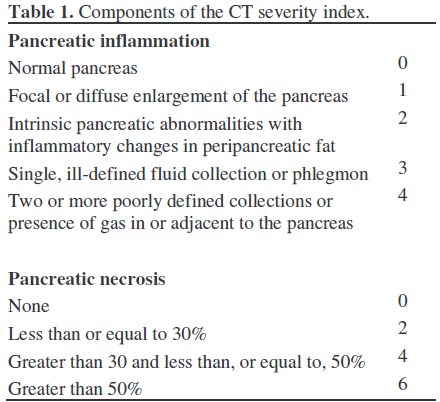
This is why the CT severity index has a critical defect. The presence of pancreatic necrosis is the most important component of the score (Table 1). But also in the Atlanta criteria, the presence of necrosis automatically puts the patients in the “severe disease” category. It is completely illogical to measure the presence of a complication on CT scan (necrosis in this case) and then state that by measuring the complication you could predict it. This is a self fulfilling prophecy, which clearly has no use in daily clinical practice.
This may explain the extremely high AUC as reported by Dr. Gürleyik et al. [1] and similar seemingly good correlations by others in the past [4, 5, 6, 7, 8].
From this, it is obvious that the CT severity index can be used to predict mortality, but as long as pancreatic necrosis is part of the criteria for disease severity, this score should not be used to predict disease severity as defined by the Atlanta criteria.
References
- Gurleyik G, Emir S, Kilicoglu G, Arman A, Saglam A. Computed tomography severity index, APACHE II score, and serum CRP concentration for predicting the severity of acute pancreatitis. JOP. J Pancreas (Online) 2005; 6:562-7. [PMID 16286706]
- Brestas PS, Dafni UG. Assessment of the severity of acute pancreatitis. the usefulness of ROC analysis in comparative studies of clinical and imaging prognostic indices. JOP. J Pancreas (Online) 2006; 7:245-6. [PMID 16525214]
- Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology 1990; 174:331-6. [PMID 2296641]
- Mortele KJ, Wiesner W, Intriere L, et al. A modified CT severity index for evaluating acute pancreatitis: improved correlation with patient outcome. AJR Am J Roentgenol 2004; 183:1261-5. [PMID 15505289]
- Vriens PW, van de Linde P, Slotema ET, Warmerdam PE, Breslau PJ. Computed tomography severity index is an early prognostic tool for acute pancreatitis. J Am Coll Surg 2005; 201:497-502. [PMID 16183486]
- Chatzicostas C, Roussomoustakaki M, Vardas E, Romanos J, Kouroumalis EA. Balthazar computed tomography severity index is superior to Ranson criteria and APACHE II and III scoring systems in predicting acute pancreatitis outcome. J Clin Gastroenterol 2003; 36:253-60. [PMID 12590238]
- van den Biezenbos AR, Kruyt PM, Bosscha K, van Leeuwen MS, Feldberg MA, van der Schouw YT, Gooszen HG. Added value of CT criteria compared to the clinical SAP score in patients with acute pancreatitis. Abdom Imaging 1998; 23:622-6. [PMID 9922198]
- Ju S, Chen F, Liu S, Zheng K, Teng G. Value of CT and clinical criteria in assessment of patients with acute pancreatitis. Eur J Radiol 2006; 57:102-7. [PMID 16112828]

