Jaballah Sakhri1, Chaker Ben Salem2, Houssem Harbi1, Neila Fathallah2, Rached Ltaief1
1Research Unit 02SP09, Department of Surgery, Farhat Hached Hospital;
2Department of Clinical Pharmacology, Faculty of Medicine of Sousse. Sousse, Tunisia
- *Corresponding Author:
- Jaballah Sakhri
Department of Surgery, Farhat Hached Hospital, Sousse, Tunisia
Phone : +216-98.456.816
Fax: +216-73.224.899
E-mail: jaballah.sakhri@rns.tn
Received March 10th, 2010 - Accepted April 21st, 2010
Keywords
Hypertriglyceridemia; Pancreatitis; Tamoxifen
INTRODUCTION
Tamoxifen is a non-steroidal estrogen antagonist widely used in adjuvant hormonal therapy for breast cancer. The adverse effects of tamoxifen are generally mild and do not induce serious complications even after extended periods of administration. Most of the adverse effects include hot flashes, fluid retention, nausea, gastrointestinal intolerance, vaginal bleeding or discharge, pruritus vulvae, rashes, dry skin and alopecia [1]. Imbalances in serum lipoprotein metabolism, including a decrease in low density lipoprotein cholesterol and an increasing in triglyceride and high-density lipoprotein cholesterol levels, have also been reported for tamoxifen therapy [2].
We report a case of tamoxifen-induced acute pancreatitis occurring after a disturbance of serum lipid metabolism with positive rechallenge.
CASE REPORT
A 44-year-old woman had a radical mastectomy for breast cancer followed by radio- and chemotherapy. Tamoxifen was started at a dose of 20 mg daily. Twelve months later, the patient was admitted to the intensive care unit for acute respiratory distress syndrome. Chest X-rays showed bilateral pulmonary edema. Laboratory tests revealed elevated triglyceridemia at 11.8 g/L (7 folds upper reference range: 0.3-1.4 g/L) and amylasemia at 750 IU/L (reference range: 0-100 IU/L). Hepatic tests were normal. Abdominal ultrasound did not show gallstones. A computed tomography scan showed massive fluid collection in the peripancreatic region and bilateral perirenal spaces. A diagnosis of acute pancreatitis grade E was made. Ranson’s score was 5. There was no history of alcohol consumption, recent abdominal trauma or preceding viral syndromes. The patient was intubated and underwent mechanical ventilation for 10 days. Tamoxifen was suspected as a probable cause of pancreatitis and was immediately withdrawn. The evolution was favorable and the patient returned home two months later. A few weeks later, her serum triglyceride level returned to within the normal range without anti-hyperlipidemic therapy. Amylasemia and lipasemia were also within the normal range. The patient was asymptomatic at the one-year follow-up. Ten months later, the patient was rechallenged with tamoxifen by her gynecologist. A few days later, the patient was re-hospitalized for severe acute pancreatitis. Tomodensitometry showed pancreatitis grade E. The patient had a hypertriglyceridemia level of 10.3 g/L. The patient benefited from therapy consisting of nil by mouth, nasogastric suction, parenteral hyper-alimentation and pain control. After a few days of hospitalization in the intensive care unit, the patient recovered slowly and was discharged with instructions to the patient herself and to her gynecologist to definitely avoid tamoxifen in the future. The temporal relationship between tamoxifen administration and the elevated pancreatic enzyme concentrations, the rapid improvement of values after stopping the drug, the recurrence of pancreatitis when the drug was readministered led us to classify our case as probable tamoxifen-induced pancreatitis. According to Badalov’s classification, tamoxifen is included in class I [3].
DISCUSSION
Acute pancreatitis is a severe disease with a high rate of morbidity and mortality. It is rarely due to drugs [4]. The pathogenesis of drug-induced pancreatitis has not yet been totally clarified. Some hypotheses suggest that drug-induced pancreatitis is probably due to an accumulation of toxic metabolites, and to a hypersensitivity reaction to drugs or as a consequence of drug-related metabolic effects such as hypertriglyceridemia [3, 4]. Many drugs, such as tamoxifen, may induce an increase in serum triglyceride levels. Tamoxifen is an antagonist of estrogen. It mainly induces an inhibition of estrogenic activities; however, it may induce some estrogenic effects including increased synthesis of triglycerides, very low density lipoproteins and decreased activity of lipoprotein lipase and hepatic triglyceride lipase [1]. The exact mechanism of elevated triglyceride-induced pancreatitis is unclear but it is thought to involve increased concentrations of chylomicrons in blood. When triglycerides levels are elevated, chylomicrons are almost certainly present after a period of time. These low density particles are numerous and may obstruct capillaries, leading to pancreatic ischemia. Moreover, the degradation of triglycerides to free fatty acids by pancreatic lipases may lead to further cytotoxic injuries which increase inflammatory mediators resulting in aggravation of the pancreatitis [5]. Although tamoxifen may induce only a modest increase in serum triglycerides in normolipidemic patients with an intact ability to catabolize lipoproteins, our patient had developed notable hypertriglyceridemia with consequent pancreatitis
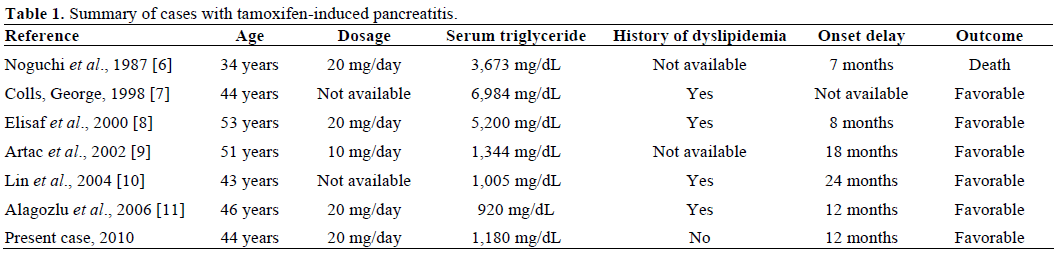
Only six cases resulting from tamoxifen therapy have been reported in the English literature until now [6, 7, 8, 9, 10, 11]. A history of hypertriglyceridemia was found in four cases and not mentioned in the other two cases. In our patient, there is no history of hypertriglyceridemia. In all of these cases, rechallenge was not performed. The features of these cases are summarized in Table 1. The outcome was favorable in all patients except one case in which the patient died. The time of onset after tamoxifen exposure and development of pancreatitis was quite long. Therefore, it is important to consider tamoxifen as a possible etiology for acute pancreatitis in patients presenting with pancreatitis after several months of tamoxifen exposure and even in patients without a history of hypertriglyceridemia.
Currently, classification systems of drug-induced pancreatitis are widely used to assess causality in pancreatotoxicity on a uniform basis. In 1980, Mallory and Kern proposed a system based on multiple criteria in which a drug was classified as having either a definite, probable or possible association with pancreatitis [12]. Since that time, authors have used this 3-group classification system. In 2005, Trivedi and Pitchumoni introduced an adapted 3-group classification system and gave more weight to the number of cases reported and positive rechallenge [13]. A classification system by Badalov et al. has recently reported a novel classification system for drug-induced pancreatitis in which less weight is given to the number of case reports and more weight is given to positive rechallenge, to the time relationship between drug use and the onset of acute pancreatitis, and to the exclusion of other causes [3].
Independently of these various classification systems, the recurrence of pancreatitis after drug rechallenge remains a strong causality parameter. However, it has been recommended that, in drug-induced pancreatitis, patients should never be rechallenged with any drug that has caused even one mild episode of pancreatitis. Rechallenge should be performed only if the benefit to the patient outweighs the risk of recurrence of the reaction. In our case, the tamoxifen-induced pancreatitis was severe and life-threatening. In the first episode of pancreatitis, the symptoms were severe and it would therefore be prudent not to rechallenge the patient with tamoxifen. Our patient was exposed a second time to a fatal outcome on rechallenging with tamoxifen. However, patients who have an absolute indication for tamoxifen treatment (e.g. those with breast cancer) should not interrupt tamoxifen after an episode of pancreatitis; treatment with tamoxifen should be continued and a fibrate should be added. Some authors have also suggested that reducing the dose of tamoxifen to 10 mg once daily may reduce the risk for hypertriglyceridemia [2]. In fact, appropriate diet and drug treatment, including dose titration, for severe hypertriglyceridemia is very effective in preventing a recurrence of hypertriglyceridemiainduced acute pancreatitis [14]. Clinicians should be aware of the risks of developing severe and even fatal acute pancreatitis with tamoxifen therapy. If tamoxifen is suspected as the probable causative agent, it should then be discontinued, and rechallenge should be avoided because of the risk of inducing severe acute pancreatitis and even a fatal outcome.
Conflict of interest
There are no conflicts of interest
References
- Shapiro CL, Recht A. Side effects of adjuvant treatment of breast cancer. N Engl J Med 2001; 344:1997-2008. [PMID 11430330]
- Liu CL, Yang TL. Sequential changes in serum triglyceride levels during adjuvant tamoxifen therapy in breast cancer patients and the effect of dose reduction. Breast Cancer Res Treat 2003; 79:11-6. [PMID 12779077]
- Badalov N, Baradarian R, Iswara K, Li J, Steinberg W, Tenner S. Drug-induced acute pancreatitis: an evidence-based review. ClinGastroenterolHepatol 2007; 5:648-61. [PMID 17395548]
- Balani AR, Grendell JH. Drug-induced pancreatitis: incidence, management and prevention. Drug Saf 2008; 31:823-37. [PMID 18759507]
- Ewald N, Hardt PD, Kloer HU. Severe hypertriglyceridemia and pancreatitis: presentation and management. CurrOpinLipidol 2009; 20:497-504. [PMID 19770656]
- Noguchi M, Taniya T, Tajiri K, Miwa K, Miyazaki I, Koshino H, et al. Fatal hyperlipaemia in a case of metastatic breast cancer treated by tamoxifen. Br J Surg 1987; 74:586-7. [PMID 3620865]
- Colls BM, George PM. Severe hypertriglyceridaemia and hypercholesterolaemia associated with tamoxifen use. ClinOncol (R CollRadiol) 1998; 10:270-1. [PMID 9764383]
- Elisaf MS, Nakou K, Liamis G, Pavlidis NA. Tamoxifeninduced severe hypertriglyceridemia and pancreatitis. Ann Oncol 2000; 11:1067-9. [PMID 11038048]
- Artac M, Sari R, Altunbas H, Karayalcin U. Asymptomatic acute pancreatitis due to tamoxifen-induced severe hypertriglyceridemia in a patient with diabetes mellitus and breast cancer. J Chemother 2002; 14:309-11. [PMID 12120888]
- Lin HH, Hsu CH, Chao YC.Tamoxifen-induced severe acute pancreatitis: a case report. Dig Dis Sci 2004; 49:997-9. [PMID 15309890]
- Alagozlu H, Cindoruk M, Unal S. Tamoxifen-induced severe hypertriglyceridaemia and acute pancreatitis. Clin Drug Investig 2006; 26:297-302. [PMID 17163263]
- Mallory A, Kern F Jr. Drug-induced pancreatitis: a critical review. Gastroenterology 1980; 78:813-20. [PMID 6986321]
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J ClinGastroenterol 2005; 39:709-16. [PMID 16082282]
- Athyros VG, Giouleme OI, Nikolaidis NL, Vasiliadis TV, Bouloukos VI, Kontopoulos AG, Eugenidis NP. Long-term followup of patients with acute hypertriglyceridemia-induced pancreatitis. J ClinGastroenterol 2002; 34:472-5. [PMID 11907366]

