Emma L Edghill1, Jayne AL Minton1, Christopher J Groves3, Sarah E Flanagan1, Ann-Marie Patch1, Oscar Rubio-Cabezas1,4,5, Maggie Shepherd2, Sigurd Lenzen6, Mark I McCarthy3, Sian Ellard1 and Andrew T Hattersley1
Institutes of 1Biomedical and Clinical Science and 2Health and Social Care, Peninsula Medical
School. Exeter, United Kingdom.
3Oxford Centre for Diabetes, Endocrinology and Metabolism,
University of Oxford. Oxford, United Kingdom.
4Department of Endocrinology, Hospital Infantil
Universitario Niño Jesús;
5Department of Pediatrics, Universidad Autónoma de Madrid. Madrid
Spain.
6Institute of Clinical Biochemistry, Medizinische Hochschule. Hannover, Germany
- *Corresponding Author:
- Andrew T Hattersley
Institute of Biomedical and Clinical Science, Peninsula Medical
School, Barrack Road, Exeter EX2 5DW, United Kingdom
Phone: +44-1392.406.806
Fax: +44-1392.406.767
E-mail: andrew.hattersley@pms.ac.uk
Received June 29th, 2009 - Accepted October 13th, 2009
Keywords
Diabetes Mellitus, Type 2; Genetics, Insulin-Secreting Cells
Abbreviations
MODY: maturity onset diabetes of the young; OMIM: Online Mendelian Inheritance in Man; PNDM: permanent neonatal diabetes
INTRODUCTION
Monogenic diabetes is a heterogeneous group of disorders characterised most often by pancreatic beta cell dysfunction [1]. Two subtypes of monogenic diabetes include permanent neonatal diabetes (PNDM) and maturity onset diabetes of the young (MODY) [2]. Patients with PNDM present in the first 6 months of life and are often sporadic, whilst MODY presents within families with a strong history of diabetes and at least one subject diagnosed before the age of 25 years. To date there are ten genetic subtypes for PNDM; KCNJ11, ABCC8, INS, GCK, IPF1, FOXP3, EIF2AK3, PTF1A, SLC19A2 and GLIS3 [2]. In MODY there are ten causal genes; HNF1A, GCK, HNF4A, IPF1, HNF1B, NEUROD1, CEL, KLF11, PAX4 and INS [2]. There remains about 37% of cases with PNDM and about 11% with MODY with an unknown genetic aetiology [3]. Many of the known monogenic diabetes genes were identified as biological candidates involved in beta cell development, maintenance and function, such as GCK, KCNJ11, IPF1 and PTF1A [4, 5, 6, 7, 8]. There are many other genes involved in pancreatic development or insulin secretion demonstrated by in vitro studies, animal models, as well as recent type 2 diabetes mellitus genetic studies [9, 10]. It is reasonable to hypothesise that genes for other proteins that are critical for beta cell function could be involved in the pathogenesis of monogenic diabetes. We aimed to sequence candidate genes, selected by international experts in the functioning of beta cells (EURODIA consortium; https://www.eurodia.info/), in patients with monogenic diabetes in whom the major known causes had been excluded.
METHODS
Subjects
Seventeen cases with PNDM were selected if insulin treated at time of referral and diagnosed at less than 6 months of life. The median age of diabetes onset for the cohort was 8 weeks (range: 0-26 weeks), the median birth weight was 2.83 kg (range: 0.97-3.68) born at a median delivery of 37.5 weeks (range: 36-40 weeks). Two subjects had an affected father. The median age at time of testing was 11 years (range 5-54 years). Mutations in KCNJ11, ABCC8, INS and GCK were excluded.
Eight cases with MODY were selected that were diagnosed within 25 years of age, non-obese and at least two generations affected with diabetes. The median age of onset was 20 years (range: 15-24 years), the median BMI was 24 kg/m2, (range: 23-30 kg/m2) three subjects had an affected mother and five had an affected father. Mutations and deletions in the HNF1A, HNF4A and GCK genes had been excluded.
Candidate Gene Selection
The beta cell experts within the European beta cell consortium EURODIA were asked to nominate 3 “gold”, 3 “silver” and 4 “bronze” genes based on biological or genetic grounds. There were 107 genes (40 gold, 35 silver, 32 bronze) nominated with surprisingly little overlap in the suggestions made, with only one gene attracting three nominations (UCP2). We chose twelve genes from the list to investigate in monogenic diabetes, based on evidence for candidacy. Eight were from the “gold” category (MAFA, NGN3, NKX2.2, PAX4, PAX6, SREBF1, SYT9, UCP2), one from “silver” (LMX1A), and three from “bronze” (ISL1, NKX6.1, SOX2).
Molecular Genetics
Genomic DNA was extracted from peripheral leukocytes using standard procedures. Standard PCR and sequencing techniques amplified each of the coding exons of the 12 candidate genes; ISL1, LMX1A, MAFA, NGN3, NKX2.2, NKX6.1, PAX4, PAX6, SOX2, SREBF1, SYT9 and UCP2 (primers available on request). Changes in the sequence were checked against published polymorphisms. Variants identified were tested for co-segregation or sequenced in control chromosomes.
ETHICS
This work was done with informed consent from the participants on a study protocol which conforms to the ethical guidelines of the declaration of Helsinki and was approved by the local ethics committee.
STATISTICS
Frequency, median and range were evaluated as descriptive statistics.
RESULTS
We sequenced twelve candidate genes in 25 cases with PNDM or MODY. No pathological variants were identified.
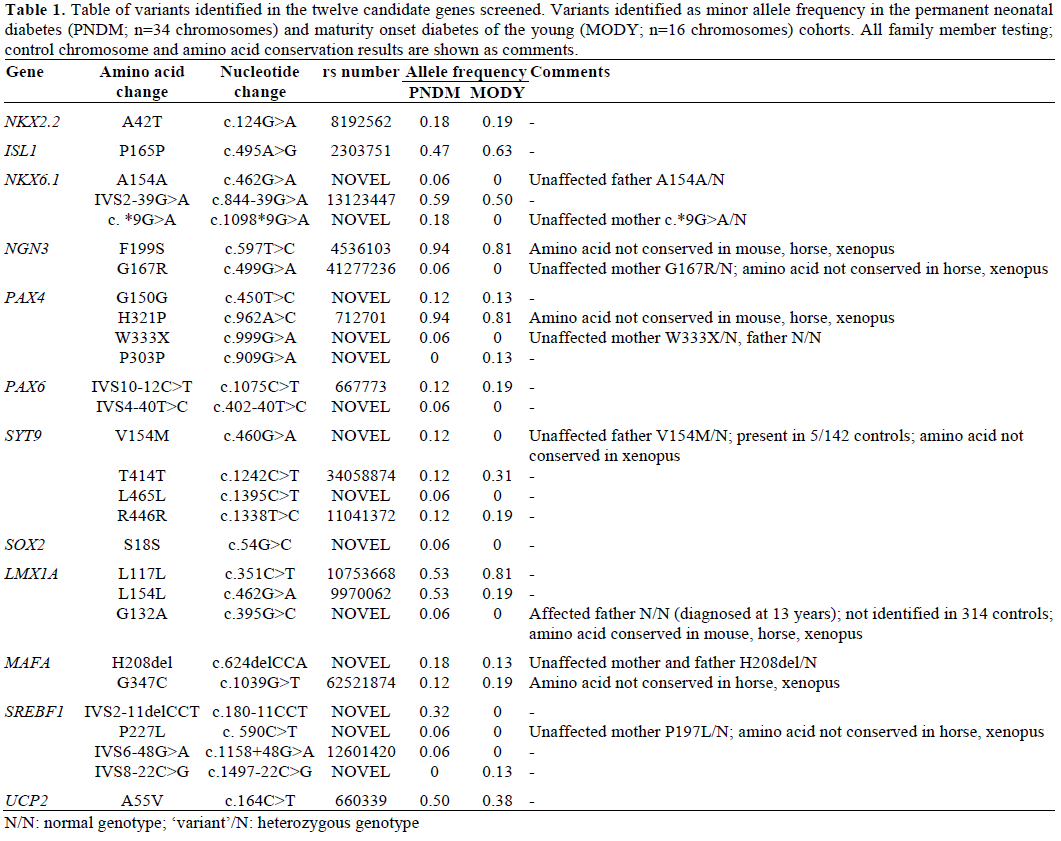
We did identify novel rare variants in these candidate genes (Table 1). A total of 5 novel non-synonymous variants were identified in PAX4, SYT9, LMX1A, MAFA and SREBF1 genes. None of these 5 variants co-segregated with diabetes within the immediate family (Table 1). In 4 cases the variant was inherited from an unaffected parent. In one patient with PNDM we identified a novel heterozygous G132A variant in LMX1A, this variant was not present in the affected father, diagnosed at 13 years, but the mother was unavailable for testing so a spontaneous mutation cannot be excluded. We also identified 13 previously described common polymorphisms (Table 1).
DISCUSSION
We failed to find mutations in twelve key beta cell genes in patients likely to have monogenic diabetes in whom a genetic aetiology had not been identified. To identify the strongest candidate genes for beta cell function we asked for nominations by internationally acknowledged experts in beta cell function who were partners in the European sponsored EURODIA project. The twelve candidate genes we investigated had sufficient biological and, for some, prior genetic evidence for candidacy. For example the transcription factor genes ngn3, nkx2.2, pax4, pax6, isl1, and mafa are critical for endocrine cell development in rodents [11, 12, 13, 14, 15, 16]. Null mouse models of nkx2.2, ngn3, and mafa result in neonatal hyperglycaemia and in some premature death in the neonatal period [12, 17, 18]. In addition to our study, Nocerino et al. [19] has recently shown that mutations in NGN3 are not a common cause of isolated diabetes, however we have since identified that recessive NGN3 mutations can cause neonatal diabetes and severe diarrhea [20]. Whilst nkx6.1, sox2, lmx1a, syt9 and srebf1 are crucial in maintaining adult beta cell function, insulin release and insulin activity [21, 22, 23, 24, 25]. In man heterozygous SOX2 mutations cause the microphthalmia and esophageal atresia syndrome (Online Mendelian Inheritance in Man; OMIM #206900; https://www.ncbi.nlm.nih.gov/omim), however these subjects have no reported beta cell dysfunction. Moreover, common variation close to PAX4, NGN3 and SREBF1 are associated with type 2 diabetes [26, 27, 28, 29, 30], whilst monogenic mutations in PAX6 result in aniridia and early onset diabetes (OMIM #106210).
We have shown that mutations in these genes are not a common cause of monogenic diabetes in our cohorts. Our sample size means we cannot exclude mutations in these genes being rare causes of PNDM or MODY and these genes remain good candidates for these conditions. We investigated patients with isolated diabetes; therefore some of these genes may be causal in patients with diabetes and other features. The screening strategy used was not designed to detect all types of mutations: the presence of large genomic deletions, mutations in deep intronic or regulatory regions cannot be excluded.
There remains a significant percentage of cases with PNDM or MODY with an unknown genetic aetiology.
There are many more biological candidates involved in pancreatic development, maintenance and function. History will show if the best strategy is to continue with a candidate gene approach or to rely on a genetic approach. There are limited numbers of PNDM or MODY families with multiple affected subjects who do not have one of the known genetic aetiologies. Ultimately novel sequencing approaches may allow the sequencing of large number of genes in a single study.
In conclusion we have shown that a selection of twelve candidate genes, nominated by experts in beta cell function, are not a common cause of isolated monogenic diabetes. Thus other genes, without a presently evident prominent role in beta cell development or maintenance may cause the diabetic metabolic state in these patients.
Acknowledgements
The authors would like to thank the EURODIA partners for nominating candidate genes and Chris Boustred, Andrew Parrish, and Amna Khamis for technical support. This work was funded by the European Union (Integrated Project EURODIA LSHM-CT-2006-518153 in the Framework Programme 6 of the European-Community). ATH is a Wellcome Trust Research leave fellow.
References
- Hattersley AT. Molecular genetics goes to the diabetes clinic. Clin Med 2005; 5:476-81. [PMID 16268330]
- Murphy R, Ellard S, Hattersley AT. Clinical implications of a molecular genetic classification of monogenic beta-cell diabetes. Nat ClinPractEndocrinolMetab 2008; 4:200-13. [PMID 18301398]
- McCarthy MI, Hattersley AT. Learning from molecular genetics: novel insights arising from the definition of genes for monogenic and type 2 diabetes. Diabetes 2008; 57:2889-98. [PMID 18971436]
- Froguel P, Vaxillaire M, Sun F, Velho G, Zouali H, Butel MO, et al. Close linkage of glucokinase locus on chromosome 7p to earlyonset non-insulin-dependent diabetes mellitus. Nature 1992; 356:162-4. [PMID 1545870]
- Hattersley AT, Turner RC, Permutt MA, Patel P, Tanizawa Y, Chiu KC, et al. Linkage of type 2 diabetes to the glucokinase gene. Lancet 1992; 339:1307-10. [PMID 1349989]
- Gloyn AL, Pearson ER, Antcliff JF, Proks P, Bruining GJ, Slingerland AS, et al. Activating mutations in the gene encoding the ATP-sensitive potassium-channel subunit Kir6.2 and permanent neonatal diabetes. N Engl J Med 2004; 350:1838-49. [PMID 15115830]
- Stoffers DA, Ferrer J, Clarke WL, Habener JF. Early-onset type- II diabetes mellitus (MODY4) linked to IPF1. Nat Genet 1997; 17:138-9. [PMID 9326926]
- Sellick GS, Barker KT, Stolte-Dijkstra I, Fleischmann C, Coleman RJ, Garrett C, et al. Mutations in PTF1A cause pancreatic and cerebellar agenesis. Nat Genet 2004; 36:1301-5. [PMID 15543146]
- Habener JF, Kemp DM, Thomas MK. Minireview: transcriptional regulation in pancreatic development. Endocrinology 2005; 146:1025-34. [PMID 15604203]
- Perry JR, Frayling TM. New gene variants alter type 2 diabetes risk predominantly through reduced beta-cell function. CurrOpinClinNutrMetab Care 2008; 11:371-7. [PMID 18541994]
- Jensen J, Heller RS, Funder-Nielsen T, Pedersen EE, Lindsell C, Weinmaster G, et al Independent development of pancreatic alphaand beta-cells from neurogenin3-expressing precursors: a role for the notch pathway in repression of premature differentiation. Diabetes 2000; 49:163-76. [PMID 10868931]
- Sussel L, Kalamaras J, Hartigan-O'Connor DJ, Meneses JJ, Pedersen RA, Rubenstein JL, German MS. Mice lacking the homeodomain transcription factor Nkx2.2 have diabetes due to arrested differentiation of pancreatic beta cells. Development 1998; 125:2213-21. [PMID 9584121]
- Sosa-Pineda B, Chowdhury K, Torres M, Oliver G, Gruss P. The Pax4 gene is essential for differentiation of insulin-producing beta cells in the mammalian pancreas. Nature 1997; 386:399-402. [PMID 9121556]
- St-Onge L, Sosa-Pineda B, Chowdhury K, Mansouri A, Gruss P. Pax6 is required for differentiation of glucagon-producing alpha-cells in mouse pancreas. Nature 1997; 387:406-9. [PMID 9163426]
- Ahlgren U, Pfaff SL, Jessell TM, Edlund T, Edlund H. Independent requirement for ISL1 in formation of pancreatic mesenchyme and islet cells. Nature 1997; 385:257-60. [PMID 9000074]
- Olbrot M, Rud J, Moss LG, Sharma A. Identification of betacell- specific insulin gene transcription factor RIPE3b1 as mammalian MafA. ProcNatlAcadSci U S A 2002; 99:6737-42. [PMID 12011435]
- Gradwohl G, Dierich A, LeMeur M, Guillemot F. neurogenin3 is required for the development of the four endocrine cell lineages of the pancreas. ProcNatlAcadSci U S A 2000; 97:1607-11. [PMID 10677506]
- Zhang C, Moriguchi T, Kajihara M, Esaki R, Harada A, Shimohata H, et al. MafA is a key regulator of glucose-stimulated insulin secretion. Mol Cell Biol 2005; 25:4969-76. [PMID 15923615]
- Nocerino V, Colombo C, Bonfanti R, Iafusco D, Barbetti F. Mutations in IAPP and NEUROG3 genes are not a common cause of permanent neonatal/infancy/childhood-onset diabetes. Diabet Med 2009; 26:660-1. [PMID 19538245]
- Rubio-Cabezas O, Codner E, Jensen JN, Hodgson MI, Serup P, Ellard S, et al. Neurogenin 3 deficiency is a novel cause of permanent neonatal diabetes and severe congenital diarrhea. Horm Res 2009; 72:61.
- Rudnick A, Ling TY, Odagiri H, Rutter WJ, German MS. Pancreatic beta cells express a diverse set of homeobox genes. ProcNatlAcadSci U S A 1994; 91:12203-7. [PMID 7991607]
- Zhao M, Amiel SA, Christie MR, Muiesan P, Srinivasan P, Littlejohn W, et al. Evidence for the presence of stem cell-like progenitor cells in human adult pancreas. J Endocrinol 2007; 195:407-14. [PMID 18000303]
- German MS, Wang J, Fernald AA, Espinosa R 3rd, Le Beau MM, Bell GI. Localization of the genes encoding two transcription factors, LMX1 and CDX3, regulating insulin gene expression to human chromosomes 1 and 13. Genomics 1994; 24:403-4. [PMID 7698771]
- Iezzi M, Eliasson L, Fukuda M, Wollheim CB. Adenovirusmediated silencing of synaptotagmin 9 inhibits Ca2+-dependent insulin secretion in islets. FEBS Lett 2005; 579:5241-6. [PMID 16165130]
- Foufelle F, Ferr? P. New perspectives in the regulation of hepatic glycolytic and lipogenic genes by insulin and glucose: a role for the transcription factor sterol regulatory element binding protein- 1c. Biochem J 2002; 366:377-91. [PMID 12061893]
- Shimajiri Y, Sanke T, Furuta H, Hanabusa T, Nakagawa T, Fujitani Y, et al. A missense mutation of Pax4 gene (R121W) is associated with type 2 diabetes in Japanese. Diabetes 2001; 50:2864- 9. [PMID 11723072]
- Plengvidhya N, Kooptiwut S, Songtawee N, Doi A, Furuta H, Nishi M, et al. PAX4 mutations in Thais with maturity onset diabetes of the young. J ClinEndocrinolMetab 2007; 92:2821-6. [PMID 17426099]
- Eberle D, Clement K, Meyre D, Sahbatou M, Vaxillaire M, Le Gall A, et al. SREBF-1 gene polymorphisms are associated with obesity and type 2 diabetes in French obese and diabetic cohorts. Diabetes 2004; 53:2153-7. [PMID 15277400]
- Grarup N, Stender-Petersen KL, Andersson EA, J?rgensen T, Borch-Johnsen K, Sandbaek A, et al. Association of variants in the sterol regulatory element-binding factor 1 (SREBF1) gene with type 2 diabetes, glycemia, and insulin resistance: a study of 15,734 Danish subjects. Diabetes 2008; 57:1136-42. [PMID 18192539]
- Li J, Bergmann A, Reimann M, Schulze J, Bornstein SR, Schwarz PE. Genetic variation of Neurogenin 3 is slightly associated with hyperproinsulinaemia and progression toward type 2 diabetes. ExpClinEndocrinol Diabetes 2008; 116:178-83. [PMID 18072012]

