Keywords
Carcinoma; Carcinoma, Pancreatic Ductal; Early Detection
of Cancer; Endosonography; Neoplasms; Neoplasm Metastasis;
Pancreas; Pancreatic Neoplasms; Therapeutics
Abbreviations
EUS endoscopic ultrasound; MDCT multidetector
computed tomography; MRCP magnetic resonance
cholangiopancreatography; MRI magnetic resonance imaging; ERCP
endoscopic retrograde cholangiopancreatography
Pancreatic cancer is the fourth leading cause of mortality
related to cancer among both genders in the United
States [1]. Unfortunately, the majority of the patients are
diagnosed at an advanced stage. Moreover, poor prognosis
even after complete surgical resection further justifies
the urgency and need to detect pancreatic cancer earlier,
especially in those individuals with identified high-risk
factors [2]. Though, pancreatic cancer is a rare disease
before the age of 45, however, the incidence rises sharply
in the younger patients over the last decade.
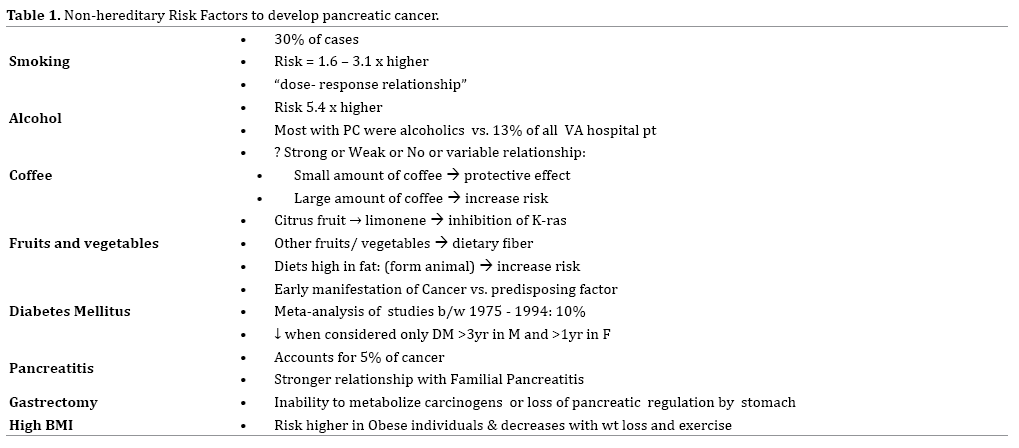
Risk factors to develop pancreatic cancer include
hereditary diseases, environmental and social conditions (Table 1 and 2). Familial aggregation and genetic
susceptibility account for approximately 10% of all
pancreatic cancer cases [3]. Nonhereditary/environmental
risk factors for pancreatic cancer include chronic
pancreatitis, diabetes mellitus, cigarette smoking, obesity
and Helicobacter pylori infection [4, 5] (Table 1).
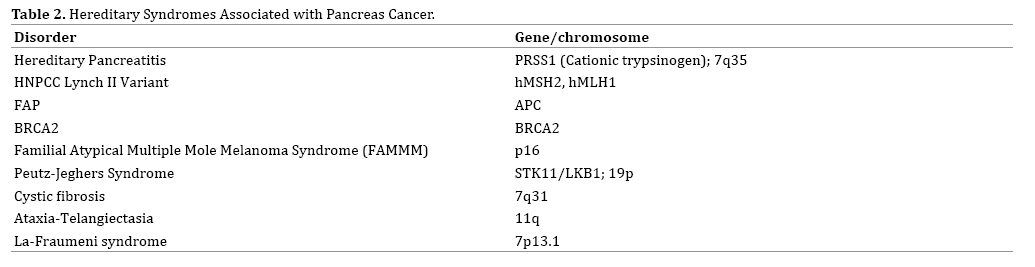
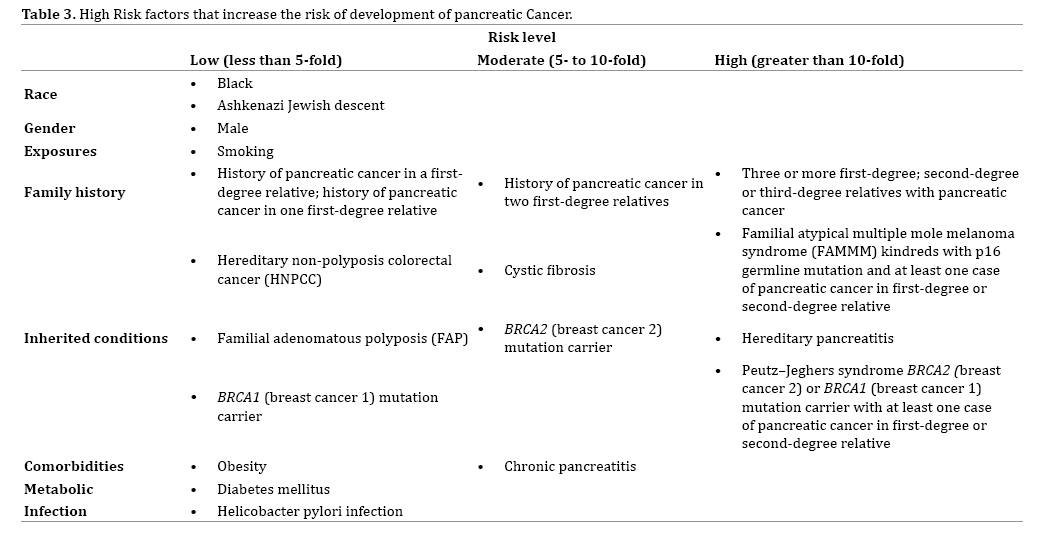
However, with better understanding of human genetics
we can now identify those at high risk for developing
pancreatic cancer [3, 4, 5, 6, 7, 8, 9] (Table 3).
Despite we have established many risk factors that
predispose pancreatic cancer in large studies; data
pertaining to its early detection remains undetermined
and inadequate. Carbohydrate Antigen 19-9 (CA 19-9)
is usually elevated in patients with pancreatic cancer;
however, its role in early detection marker in pancreatic
cancer has been discouraging in many studies [10]. One
meta-analysis, that included 2, 316 individuals, showed that the pooled sensitivity of CA 19-9 was 0.80 (95% CI
0.77-0.82) and specificity of 0.80 (95% CI 0.77-0.82), in
detection of pancreatic cancer [11]. On the other hand,
imaging techniques might be helpful in early detection of
pancreatic cancer, but of limited utility for mass screening
purposes, primarily due to cost.
In high risk asymptomatic individuals or those with
family history of pancreatic cancer, investigators evaluated
the utility of one time screening with MRI, CT scan and
EUS, or EUS and/or MRI with CA19-9 and genetic testing
respectively [5, 6, 7, 8, 9]. The yield of these screening
modalities was not being uniformly high and did not show
a cost effective benefit in detection of pancreatic cancer.
The U.S. Preventive Services Task Force (USPSTF) found no
evidence that screening for pancreatic cancer is effective
in reducing mortality; however, there is a potential
for significant harm due to the very low prevalence of
pancreatic cancer, limited accuracy of available screening
tests, the invasive nature of diagnostic tests, and the poor
outcomes of treatment [12]. At present, the USPSTF has not
addressed the effectiveness of screening in individuals with
hereditary pancreatitis or other hereditary conditions that
predispose to develop pancreatic cancer [13]. Similarly,
no society or national practice guidelines recommend
screening for pancreatic cancer in the general population.
One could argue that diet prevention and life style
modification should at least be adopted. Currently, there
were no clear guidelines regarding diet-based prevention,
however, a balanced diet with good fruit and vegetable
intake, abstaining from tobacco products along with
lifestyle modifications that can help in to reduce the risk of
pancreatic cancer [6, 7, 14].
With the identification of the above factors and
development of new diagnostic tools, the experts have
suggested screening for individuals with high risk for
pancreatic cancer. One such guidelines were devised by
the participants of the Fourth International Symposium of
Inherited Diseases of the Pancreas, held in Chicago, IL, USA
on November 7-9, 2009 [15], who recommend screening
only for those at high risk (more than 10-fold relative risk (Figure 1) for pancreatic cancer.
Figure 1. Screening in patients at risk of pancreatic cancer.
Diagnostic imaging tools used in high-risk individuals
may include endoscopic ultrasound (EUS), multidetector
computed tomography (MDCT), magnetic resonance cholangiopancreatography (MRCP), magnetic
resonance imaging (MRI), and endoscopic retrograde
cholangiopancreatography (ERCP). It is important to
borne in mind that the application of these diagnostic tests
for pancreatic cancer detection screening is very limited
for the general adult population.
Medical literature suggests that micoRNAs (miRNA)
are related to many different cancers including pancreatic
cancers [16, 17] Ding et al. conducted a meta-analysis
including 2, 036 patients and 1, 444 controls to assess
the use of miRNAs as possible biomarkers to be used
a s as a screening tool for pancreatic cancer [18]. This
meta-analysis showed that the use of multiple miRNA
for discriminating pancreatic cancer patients from healthy
individuals had a pooled sensitivity of 82% (95% CI, 78–
86%) and specificity of 77% (95% CI, 73–81%), suggesting
a potential diagnostic value of miRNAs for pancreatic cancer.
Other biological markers, such as PAM4-enzyme
Macrophage inhibitory cytokine, carcinoembryonic
antigen cell adhesion molecule, DNA methylase transferase,
osteopontin, mucin, S100A6 and others are undergoing
testing but none of them have been validated up to date
[19, 20, 21].
In summary, many efforts have been undertaken to find
effective ways to detect pancreatic cancer earlier as the
majority of the patients are diagnosed at an advanced stage
and bears grave prognosis. Despite all previous attempts at
finding a reliable screening modality for pancreatic cancer,
no study to date has shown improved survival. CA19-9 is
not a screening test. However, a multidisciplinary group
of experts should be involved in detecting noninvasive
precursor lesions to pancreatic cancers at a curative stage
in high risk patients, such as those with inherited cancer
susceptibility syndromes and patients with hereditary
pancreatitis.
Funding Sources
The project described was supported by the National
Institutes of Health through grant numbers UL1 TR001064.
Conflict of Interest
The author has no potential conflicts of interest.
References
- American Cancer Society: Cancer Facts and Figures 2018. Atlanta, Ga: American Cancer Society, 2018. Available online. Exit Disclaimer. Last accessed January 5, 2018.
- Bussom S, Saif MW. Methods and rationale for the early detection of pancreatic cancer. Highlights from the “2010 ASCO Gastrointestinal Cancers Symposium”. Orlando, FL, USA. JOP 2010;11:128–130. [PMID: 20208319]
- Tersmette AC, Petersen GM, Offerhaus GJ, Falatko FC, Brune KA, Goggins M, et al. Increased risk of incident pancreatic cancer among first-degree relatives of patients with familial pancreatic cancer. Clin Cancer Res 2001; 7: 738-44. [PMID: 11297271]
- Nöthlings U, Wilkens LR, Murphy SP, Hankin JH, Henderson BE, Kolonel LN. Meat and fat intake as risk factors for pancreatic cancer: the multiethnic cohort study. J Natl Cancer Inst 2005; 97:1458-65. [PMID: 16204695]
- Canto MI, Hruban RH, Fishman EK, Kamel IR, Schulick R, Zhang Z, et al. Frequent detection of pancreatic lesions in asymptomatic high-risk individuals. Gastroenterology 2012; 142:796. [PMID: 22245846]
- Verna EC, Hwang C, Stevens PD, Rotterdam H, Stavropoulos SN, Sy CD, et al. Pancreatic cancer screening in a prospective cohort of high-risk patients: a comprehensive strategy of imaging and genetics. Clin Cancer Res 2010; 16:5028. [PMID: 20876795]
- Langer P, Kann PH, Fendrich V, Habbe N, Schneider M, Sina M, et al. Five years of prospective screening of high-risk individuals from families with familial pancreatic cancer. Gut 2009; 58:1410. [PMID: 19470496]
- Lowenfels AB, Maisonneuve P, DiMagno EP, Elitsur Y, Gates LK Jr, Perrault J, et al. Hereditary pancreatitis and the risk of pancreatic cancer. International Hereditary Pancreatitis Study Group. J Natl Cancer Inst 1997; 89:442-6. [PMID: 9091646]
- Canto MI, Goggins M, Hruban RH, Petersen GM, Giardiello FM, Yeo C, et al. Screening for early pancreatic neoplasia in high-risk individuals: a prospective controlled study. Clin Gastroenterol Hepatol 2006; 4:766. [PMID: 16682259]
- Canto MI, Harinck F, Hruban RH, Offerhaus GJ, Poley JW, Kamel I, et al. International Cancer of the Pancreas Screening (CAPS) Consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut 2013; 62:339. [PMID: 23135763]
- Huang Z, Liu F. Diagnostic value of serum carbohydrate antigen 19-9 in pancreatic cancer: a meta-analysis. Tumour Biol 2014;35:7459-65. [PMID: 24789274]
- U.S. Preventive Services Task Force; Guide to Clinical Preventive Services. 2nd ed. Washington, DC: Office of Disease Prevention and Health Promotion; 1996.
- Harris RP, Helfand M, Woolf SH, Lohr KN, Mulrow CD, Teutsch SM, et al. Preventive Services Task Force: a review of the process. Am J Prev Med 2001;20:21-35. [PMID: 11306229]
- Abdelrehim MG, Mahfouz EM, Ewis AA, Seedhom AE, Afifi HM, Shebl FM. Dietary Factors Associated with Pancreatic Cancer Risk in Minia, Egypt: Principal Component Analysis. Asian Pac J Cancer Prev 2018;19:449-455. [PMID: 29480075]
- Brand RE, Lerch MM, Rubinstein WS, Neoptolemos JP, Whitcomb DC, Hruban RH, et al. Advances in counselling and surveillance of patients at risk for pancreatic cancer. Gut 2007; 56: 1460. [PMID: 17872573]
- Calin GA, Dumitru CD, Shimizu M, Bichi R, Zupo S, Noch E, et al. Frequent deletions and down-regulation of micro-RNA genes miR15 and miR16 at 13q14 in chronic lymphocytic leukemia. Proc Natl Acad Sci U S A. 2002; 99: 15524-9. [PMID: 12434020]
- Navon R, Wang H, Steinfeld I, Tsalenko A, Ben-Dor A, Yakhini Z. Novel rank-based statistical methods reveal microRNAs with differential expression in multiple cancer types. PLoS One 2009; 4: e8003. [PMID: 19946373]
- Ding Z, Wu H, Zhang J, Huang G, Ji D. MicroRNAs as novel biomarkers for pancreatic cancer diagnosis: a meta-analysis based on 18 articles. Tumour Biol 2014; 35:8837-48. [PMID: 24880590]
- El-Jurdi NH, Saif MW. Pancreatic cancer: new hopes for early detection and a future screening tool? JOP. J Pancreas (Online) 2014; 15:358-359. [PMID: 25076343]
- Shah UA, Saif MW. Tumor markers in pancreatic cancer: 2013. JOP 2013;14:318-21. [PMID: 23846917]
- Eguia V, Gonda TA, Saif MW. Early detection of pancreatic cancer. JOP 2012;13:131-4. [PMID: 22406583]


