Key words
chronic disease, health literacy, organisational
culture, school health, sickle cell, young
children
Introduction
Sickle cell disorder (SCD) is a serious inherited
chronic illness that affects all ethnic groups, but which
in the UK is most prevalent in people of black African
and black Caribbean descent (Streetly et al, 2010). To
date, the experience of young people with SCD is
under-researched within both health and education
policy (Atkin and Anionwu, 2010). The experience of
illness within education arenas is an especially underresearched
area, given that children and young people
spend such a high proportion of their time negotiating
such settings as part of managing their long-term
health condition. Young people with SCD report negative
school events that trigger or worsen their illness
experience. Sharing knowledge of sickle cell status
with either teachers or school peers does not improve
their physical, mental and social health experiences at
school (Dyson et al, 2010a). This leads us to consider
that less tangible aspects of the school context may
constitute a plausible explanation of the varied health
experiences of young people with SCD in schools in
England. In this paper we outline SCD, review some of
the key ideas about school climate, school culture and
school ethos, and consider the application of school
ethos to empirical data drawn from a multi-methods
research programme to investigate the experiences of
young people with SCD at school.
Background
Young people with SCD exhibit diverse health needs at
school because of the variable nature of the condition
and the variation in the social reactions of others, both teachers and peers. People with SCD are susceptible to
episodes of acute and chronic pain and to severe
anaemia. Such episodes may be exacerbated by extremes
of heat, cold, dehydration, stress or strenuous
activity. These can also adversely affect the person’s
ability to concentrate and to engage in learning activities.
With this in mind, schools need to respond to
the educational needs of young people whose learning
may be compromised. Schools have a responsibility
to provide a learning environment that is integrally
responsive to all young people. As such, schools need
to foster an ethos, a way of thinking and being, that
values human rights, diversity and equity, and ultimately
facilitates successful learning for all members of
the school community (Johnson, 2003).
A positive school ethos, characterised by student
and teacher cohesion, positive teacher attitudes towards
young people, an emphasis on positive rewards, and
consistent and shared values and standards is pivotal
in shaping school experience (Rutter et al, 1979). A
positive school ethos can facilitate the kind of learning
environment that is essential for young people with
long-standing chronic conditions such as SCD if they
are to reach their potential. A negative school ethos, or
one that does not recognise consistent and shared
values and standards, and does not value the participation
of young people and parents in school life, may
prove to be a barrier to effective learning for young
people with chronic illnesses such as SCD. Changes to
school policy and practice may be regarded by some
schools as counterproductive, serving to prioritise the
rights of some young people over others. However,
young people with SCD face health challenges that are
physical (dehydration, pain and anaemia), mental
(stress associated with taunting, bullying or body
image) and social (isolation, especially in relation to
school re-entry after absence, exclusion from school activities, and being perceived as different frompeers).
Teachers should respect the rights of young people to
have their physical needs met while at the same time
ensuring their mental well-being by maintaining dignity
and privacy. When respecting young people’s
rights to protection of their physical health, schools
need to be careful not to draw attention to individuals
in ways that differentiate them from their peer group
and undermine their social health.
To more fully understand the reported school
experiences of young people with SCD in our study,
in particular why the decision to either disclose or not
disclose their SCD to a range of significant others does
not appear to be correlated with school experience, we
needed to look beyond mere reporting of health status.
Weconsider the concepts of school climate, culture and
ethos, terms that are distinct but that are often used
interchangeably (Glover and Coleman, 2005), and
draw attention to limitations of ostensibly similar
concepts such as health-promoting schools and health
literacy, before looking in detail at school ethos to
explain the reported school experiences of young
people with SCD.
School climate, culture and
ethos
School climate is defined by Moos (1979) as the social
atmosphere of the learning environment in which
young people have different experiences according
to the protocols set up by teachers and administration.
It is a term often used to describe the school environment
in the North American and Australian context. It
appears to refer to the relationship that young people
have with the school as an organisation, with its
attendant rules and procedures, as well as their relationships
with teachers and with each other. In the
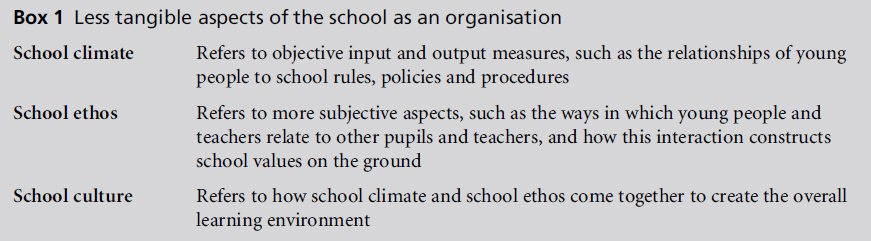
UK and Europe the term culture tends to be used. The
term school climate is used when objective data are
under consideration, whereas school ethos is used when
more subjective descriptors are involved (Glover and Coleman, 2005). Culture, on the other hand, is used
when ethos and climate are brought together as an
integrative force in investigation or debate. In this
context, culture refers to indicators that are measurable
yet also capable of subjective evaluation (Glover
and Coleman, 2005). Culture is viewed, therefore, as
an amalgam of the way things are done, reconciled
with descriptors of how things are done, and is arguably
a more complex and dynamic set of relationships
within the school environment than is covered by
either climate or ethos (Bolman and Deal, 1984; Peterson
and Deal, 1998) (see Box 1).
Ethos appears in all contexts as a descriptor of social
dynamics either in place or as a broad component of
the term culture. Ethos, unlike climate, is less concerned
with the measurement of environmental factors
and outcomes for young people, and is more
concerned with the way in which people interact in
developing and then attaining a set of values (Glover
and Coleman, 2005). Ethos has been viewed fromboth
positivist and anti-positivist perspectives (Donnelly,
2000). From a positivist perspective, it is a top-down
prescription of social reality, an objective phenomenon,
and exists independently of the people and
social events in an organisation. School ethos in this
sense would necessarily require the authorities within
the organisation to commit to the types of behaviour
expected throughout the school, formally expressed in
the school’s aims and objectives. An anti-positivist
view of school ethos is seen as less formal, being more
to do with social interaction and processes emanating
from individual and group interaction. In this sense,
school ethos need not be stated or documented in any
formal way, being more akin to the concept of culture,
which emerges from social interaction and is part of,
not independent of, the organisation and its members
(Donnelly, 2000). Irrespective of philosophical position,
the notion of school ethos has, since Rutter et al
(1979) published their findings, become firmly associated
with school effectiveness and improvement
(Smith, 2003). This preoccupation with school effectiveness
and improvement and subsequent target
setting may lead schools to formally espouse a particular
ethos on the one hand, while on the other engaging in interactional practices that negate the
official message. For example, schools that are preoccupied
with attainment may fail to respond to the
individual health and learning needs of the young
person.
The holistic emphasis of school climate, ethos or
environment has superficial parallels with concepts
such as the health-promoting school (Lee, 2009), but
although such concepts may end with recommendations
to adjust the school environment, the starting
point seems to be the health and lifestyle behaviours of
the general school population (McLellan et al 1999),
rather than consideration of specific reasonable adjustments
to support the health and learning of a
young person living with a chronic condition such
as SCD. Moreover, the irony is that an ostensibly
collectivist framework remains individualistic in its
conception of the mechanisms through which differential
health statuses are effected, and outwith the
social determinants of health such as material deprivation
and racism (Karlsen and Nazroo, 2002; Williams
et al, 2003). Furthermore, related concepts such as
health literacy reinforce this individualising of social
problems (Paasche-Orlow and Wolf, 2010), and ignore
the fact that at least part of the social reproduction
of racism may itself be through the workings
of the educational system (Gillborn, 2008), and that
for a young person living with chronic illness at
school, a strong health literacy may itself be in tension
with the procedures of a school (Dyson et al, 2011).
In summary, school climate concerns the measurable
input and outcome features of the school experience,
whereas ethos is concerned with the subjective
values and principles underpinning policy and practice.
Culture is said to integrate the environmental, organisational
and experiential features of school existence
to offer a context for teaching and learning, and its
subsequent improvement. In the absence of data relating
to overall school aims and objectives, we are reliant in
this study on the reported and therefore subjective
accounts given by the young people with SCD and
their carers. We have therefore chosen to frame our
discussion within the concept of school ethos, rather
than climate or culture, as, of the three, this is the
concept commensurate with the subjective reported
accounts that form the basis of our investigation of
school experience.
The study
Design
The overall aim of the research programme was to
provide an understanding of the experiences of young
people with SCD at school. Within this overall aim, the purpose of this paper was to provide a plausible
explanation of variation in school experience, when
evidence suggests that SCD disclosure to teachers is
not associated with reported improvement in experience.
A mixed methods approach was selected to
facilitate collection of a range of data from a variety
of sources. The first of these was a questionnaire developed
to ascertain the experiences of young people at
school, asking about school absence, support provided,
and whether their SCD status was disclosed to
teachers and/or other young people. Secondly, taperecorded
1-hour interviews, in the form of ‘guided
conversations’ (Fielding, 1993, p. 144), also asked about
experiences at school that could improve or worsen
their symptoms, and focused further on reasons for
and against disclosing SCD status to teachers and/or
peers. Thirdly, case studies were conducted with 10
young people, selected for diversity in terms of gender
and ethnicity, and encompassing a 1-hour tape-recorded
interview with the young person, a 1-hour recorded
interview with their main carer, and a 2-week diary of
their school experiences, captured by speaking about
their experiences into a digital recorder at the end of
the school day. The case studies covered all of the issues
mentioned above, but also asked the carers about
perceived racism. The diaries also elicited, without
specific questioning of the young people, accounts of
bullying at school.
Ethical issues
The study was approved by De Montfort University
Human Research Ethics Committee, a multi-centre
health services (NHS) ethics committee and six health
services research and development offices in different
English localities. In each case potential respondents
were offered age-appropriate information sheets. Completion
and return of questionnaires was assumed to
imply consent. Those invited to take part in interviews
and case studies were asked for their signed written
assent (if under 16 years of age) and the written
consent of their carers. Those who were older were
able to give their own consent.
Participants and data collected from
questionnaires
Young people with SCD aged 4–25 years were
recruited from three London outpatient clinics, three
primary care settings (London and Birmingham) and
12 local sickle cell support groups (covering London,
the South West, the West Midlands and the East
Midlands). There were equal numbers of male and
female participants. Although our recruitment age
range was 4–25 years, the majority of the respondents
were within the age range for compulsory schooling in England (5–16 years). SCD can affect any ethnic group,
but the largest groups in our sample were young black
people of either African or Caribbean descent (Dyson
et al, 2010b), reflecting the current prevalence of SCD
in different socially defined ethnic groups (Streetly
et al, 2010). A total of 569 questionnaires, administered
face to face, were completed by the young
people or their main carers. Only five potential respondents
declined to complete a questionnaire. Data
were entered and analysed using SPSS 16.0 (Dyson
et al, 2010a).
Participants and data collected from
interviews
A total of 40 audio-recorded interviews were conducted
with young people aged 6–25 years (average age 16
years). There were 21 female and 19 male participants,
and 24 black Africans, 15 black Caribbeans and one
British Asian, purposively selected to reflect diversity
in both level of school attainment and level of perceived
school support. The interviews were transcribed
in full and analysed using a broadly thematic approach
within a Bourdieusian theoretical framework (Dyson
et al, 2011).
Participants and data collection from
case studies
A total of 10 case studies were conducted with male
and female participants of both black African and
black Caribbean descent. These consisted of taped
interviews with the 10 young people with SCD, interviews
with their main carer, and 2-week diaries kept by
the young people with SCD. These were analysed by
grouping young person interviews, carer interviews
and diaries covering the same ‘case’ together, and
identifying recurrent themes in the data.
Field notes were also kept by the research team on
events and informal meetings. We draw on all of these
sources of data in presenting our arguments in this
paper.
Findings
Young people with SCD faced challenges to their
physical health at school. These reported negative
experiences included being prevented from using
the toilet (people with SCD cannot concentrate their
urine and need to pass dilute urine frequently), being
denied access to water (remaining hydrated is a key
measure in the prevention of illness), being compelled
to take strenuous exercise (triggering episodes of ill
health) and being labelled as ‘lazy’ by teachers (ongoing severe anaemia in SCD leads to tiredness,
lethargy and lack of concentration). There was no
statistical association between the extent of reported
disclosure of the participants’ sickle cell status to school
staff and reported exposure to these health-damaging
events at school. Equally there was no statistical link
between declaring their SCD status to school peers and
reporting having had these negative experiences (Dyson
et al, 2010a). Positive and negative experiences were
equally in evidence when teachers and classmates knew
and when they did not know that the young person
had SCD. The severity of the SCD symptoms did not
appear to explain levels of exposure to negative responses
in school. We therefore need to look beyond
the apparently plausible, but actually incorrect, notion
that school experiences can be improved by informing
teachers and peers that the young person has SCD.
The possible explanation that we put forward here is
school ethos.
School ethos and the reported
experiences of young people
with SCD
As we have seen, the ethos of an institution is generally
taken to refer to the distinguishing character, beliefs
and moral nature of the organisation concerned. Thus
school ethos has to do with the spirit or fundamental
values of a school. In the UK, the government ministry
provided guidance to schools encouraging them to
think about their school ethos, and suggested areas of
concern that might inform such an ethos (Department
for Children, Schools and Families, 2010). These indicators
include the attitudes expected of young people
and teachers, how young people relate to each other
and to staff, how the school relates to the community
in which it is situated, and how the school ensures the
spiritual, moral, cultural and social development of
the young people attending the school. We shall look
at each of these areas in turn.
Attitudes expected of young people
If we take as a starting point the issue of the attitudes
expected of young people, we can see that a school
ethos cannot simply be a case of attending to these
factors in isolation. For example, one might argue that
a positive school ethos will attempt to inculcate good
behaviours (e.g. to attend school regularly, to be attentive,
not to be disruptive, and to push oneself to one’s
limits). However, people with SCD may miss considerable
amounts of schooling and so not attend
regularly. Their anaemia may leave them feeling tired,
unable to concentrate, and vulnerable to the charge of being ‘lazy.’ They may want to take care when exercising
and resist attempts to push themselves. Requests
for water or for toilet breaks may be interpreted
as disruptive of classroom routines, as the following
young person suggests:
‘... whenever I needed to go toilet I couldn’t. So yeah that is
when I said that if I wet myself she would dry clean it, she
would pay for the dry cleaning. She was being ridiculous,
I told her. ... The next time I asked she was like ‘No wet
yourself.’ I didn’t actually wet myself but I was so close one
time, so I just walked out. ... When I needed to go toilet I
would say, I would ask, can I go toilet please? She would
say no, so I would ask again. Can I go toilet please? No.
Third time I am going toilet now, get my stuff go toilet,
come back and sit down. She was like ‘(name), here, now’
and have a go at me, then my mum went to see the head
teacher, it is like so uncalled for.’
(Interview 10, black African female, 18 years of age)
It could be argued that a school can only be said to
have a positive ethos if that ethos is holistic and
informs all aspects of school life. If it is reduced to a
programmatic or mechanistic application of procedures
that take no account of, or do not make
reasonable adjustments for, young people with longterm
health problems or disability, the young person
with SCD is positioned as deviant, transgressing
school values. The Equality Act 2010 permits a school
to undertake positive action provisions that entail
allowing schools to develop measures that are
designed to alleviate disadvantages experienced by,
or to meet the particular needs of, young people with
particular protected characteristics. This could, for
example, include those living with SCD.
Attitudes expected of teachers
One key aspect of enabling young people to be high
achievers in gaining educational qualifications is the
extent to which teachers do not limit their expectations
of young people from low-income backgrounds
or young black people with regard to achievement.
This could plausibly be the case from either end of the
political spectrum, that is, a racist belief in genetic or
cultural inadequacies of certain categories of young
people, or a belief in the enduring capacity of poverty
and racism to erode educational performance. A
positive school ethos is arguably one that does not
place limits on expectations, and instead expects high
standards from its young people. Even in mixedability
groups this could take the form of an institutional
commitment that all young people will leave
the school with at least one publicly recognised qualification.
A poor school ethos would be one in which
teachers make assumptions about the abilities and
potential of certain young people and restrict their
opportunities in ways that could become self-fulfilling. For example, one young person in our study gave the
following account of the effects of anaemia on her
learning, and the teachers’ expectations of her:
‘Right, teachers some of them are understanding because
they [think that] I would do the work if I could, but they
understand that I do get tired. Some teachers will think
I’m lazy, and I’m thinking if you give me the work, I’ll take
it home and do it when I can, when I [have] a burst of
energy, but some teachers really think I’m lazy, and that
like, I’m not, like/I’ll get the grades for you, but they think
I’m lazy, so they’re like, ‘How do you/Are you cheating
duhduh’, and like I do know the material, I get tired so I
won’t like get notes from someone else, or something like
that just to keep up with the rest of the class.’
(Interview 1, black African female, 16 years of age)
The attitude of the teacher in this account is to suggest
that the young person with SCD has limited ability,
such that success in school work is attributed to cheating,
rather than to ability or hard work. It is not clear
whether this is based on the teacher’s assumptions
about the lack of potential of young people with
chronic illnesses and/or of young black people. However,
the net result is to communicate to the young
person a low teacher expectation of her potential, a
negative ethos that the young woman has to struggle
against.
How young people relate to each
other
School ethos also has to do with how the young people
in the school are expected to behave towards one
another. In our interviews, three young men and
one young woman reported being physically abused
in relation to their SCD. Others reported being teased
and taunted about having ‘yellow eyes’, being skinny,
being ‘a slowcoach’, being constantly unwell and away
from school, or being a ‘drama queen’ for expressing
their pain. One young person described the experience
as follows:
‘... oh, sickle cell, he is like, he is like one, one who cannot
afford to run who cannot afford to do things, one who can
die anytime ... people with sickle cell are better off dead
when they are young, rather than living and suffering, you
know, so you got to hear all that rubbish, so you know. ...
[A friend] believes in like checking the genes and like and
if they have sickle cell, it is like no, no, no, you should not
have them. They should be terminated or something like
that.’
(Interview 32, black African male, 25 years of age)
In this case the young person is upset by the pervasive
negative discourse around SCD as a chronic illness, to
the extent that even someone she regards as a friend is
prepared to say to her that the birth of people with SCD should be prevented, presumably by termination.
Bullying by young people and discriminatory discourses
that go unchallenged suggest a negative school
ethos. Another young person (Interview 33, British
Asian male, 21 years of age) recounted a severe painful
sickle cell episode that was triggered when he was
assaulted by another young person at school. The head
of the school year went to the home of the perpetrator
and challenged the parents about their young person’s
bullying. In not tolerating a single instance of such
antisocial behaviour, in engaging the parents as well
as the young person, in using outreach rather than
assuming that responsibility stops at the school gates,
and in carrying through remedial actions consistently,
the school arguably demonstrated a positive ethos.
How young people relate to staff
One possible indicator of school ethos is the relationship
between young people and staff, and in particular
the degree of inclusiveness within the school, and
support or lack of it in relation to school re-entry after
illness.The followingfield noteswere taken during a visit
to a local sickle cell support group to give feedback on
the results of the questionnaire phase of the study.
‘The mother was distraught because her 16-year-old son
had been excluded from school a few weeks before his
GCSE examinations. ... Her son has had a great deal of
time off school with illness. He has not been achieving
very well in his studies. Last week he got into a fight with
other students around the issue of his frequent absences.
The mother says this is the first time he has been in such
trouble at school. However, the school have responded by
excluding him for four weeks. The mother has asked the
school why the length of exclusion has been so long for a
first offence, and has twice asked the school to produce
any evidence that this incident is in any way a culmination
of poor behaviour at school.The school hasnot responded ...
when challenged about the exclusion the school had
backtracked and suggested that the exclusion was not
formal but asked the boy to take ‘study leave’ covering two
weeks before the Easter vacation and four weeks after.
This was said to be to help him revise better for his GCSEs.
... the letter said that excluding the boy from school would
take him away from the influence of a ‘‘negative peer
group’’.’
(Field notes, 25 March 2009)
In this example the school apparently failed to challenge
a group which it acknowledged to be a negative
influence. Instead, having reportedly offered no support
to the victim, it imposed a four-week exclusion
for a first offence and compounded it by making the
illegal suggestion that it should be construed as study
leave, possibly to get a low-achieving young person off
the books before exams that would influence leaguetable
results.
How the school relates to the
community
Carers of people with SCD described having to repeatedly
go into school to educate teachers about SCD
and their child’s specific requirements. The notion of
parent or carer as expert is one that some schools
appeared to be reluctant to acknowledge. School ethos
is in part about how the school positions itself in
relation to the community. By implication, a school
that refuses or is reluctant to acknowledge that parents
or carers may be experts on their own children’s health
exhibits a poor school ethos. The majority of the
parents reported a perception that, for their children,
a school where there was a significant proportion or
a majority of young black people helped with the
acceptance of SCD as a legitimate issue, presumably
because of the manner in which sickle cell has traditionally
been constructed as a black issue rather than
as a health issue (Dyson and Atkin, 2011). The following
extract highlights how one parent was persuaded to
talk to teachers about the condition of sickle cell, not
only on behalf of her own child, but also on behalf of
others with the condition:
‘They persuaded me to give a talk to the school, and they
bought some sickle cell videos for the library. So I worked
with the school to empower them and also realised there
were other children in the school which the school didn’t
recognise neither.’
(Case Study 1, black Caribbean mother)
Willingness to acknowledge a community of experts
on whom schools can draw as a resource is fundamental
to a school ethoswhich claims to recognise and
value the relationship that the school has with the
community. According to one respondent, preparedness
to engage with the community can be readily
demonstrated by a school through, for example, the
simple act of inviting into the school members of
voluntary organisations who can provide an opportunity
to raise awareness among teachers, young people
and parents of the implications of SCD in educational
settings (Case Study 2, black Caribbean health professional).
Spiritual development
Integral to school ethos is the spiritual development of
the child. Stuart (1999) argues that schools have to pay
attention to the world in which young people live, all
the elements of which contribute to spiritual development.
People make choices as to whether or not
spirituality is an important aspect of their daily life.
Consequently, no individual, including teachers, can
presume on behalf of another, including young people,
the role that spirituality should or could play. Schools
whose ethos includes the spiritual development of young people should acknowledge their right to determine
those aspects of self that they wish to share with or
withhold from others. This is integral to the development
of self-awareness, which is a key aspect of
spirituality. A young person with SCD has the right
to choose to disclose (or not) their disorder, and to
whom (or not) they wish to disclose this aspect of
themselves.
Classroom studies that are relevant and contribute
to spiritual development may include sessions about
personal and social issues. However, the extent to
which classroom-based discussion is successful in
assisting such development is dependent on the skills,
attitudes, attributes and knowledge of the teachers. A
school ethos that respects an individual’s right to
determine which aspects of the self to reveal to others
may incur a tension between spiritual development
and the need to keep others informed about an individual’s
SCD. The account provided by the following
respondent mirrors this tension by highlighting the
need for schools on the one hand to understand the
disorder, while on the other respecting the right of
parents and children to withhold information.
‘It’s very difficult, because I think you have to start from a
process where, you know, people understand that this is a
really serious condition, that can have serious effects, er,
and you know end in a very serious way, and you will
never get people to understand that unless people with it
impact on society, put themselves out to say we’ve got the
condition. Unfortunately some mothers or parents don’t
even make the school aware their children have SCD,
because they still look at it as something to be ashamed of,
and to be hidden, you know, they are worried about how
people are going to, you know, deal with their child once
they know their child has it.’
(Case Study 6, black Caribbean mother)
Moral development
A further aspect of school ethos is the attitude of the
school towards the moral development of the young
person. Moral development is more than the level of
cognitive development, and more than teachers illustrating
a set of values by their own behaviour and
hoping that young people will emulate them (Kohlberg
and Turiel, 1971). Moral behaviour has been said to
necessitate a sense that young people can progress
through stages of moral development. Each stage of
this moral development represents a further de-centring
of the egocentric viewpoint. Initially it starts with
recognising that there are other interests. Subsequently
this moral development entails accommodating one’s
views to the circumstances of, progressively, immediate
others, wider society and a sense of good beyond
immediate social norms. Moral education becomes
less about promoting good behaviour through example, and more about structuring learning to enable young
people to progress, for example, through examination
of moral dilemmas that challenge their world view.
Others have distinguished between morality and convention,
noting that intrinsic fairness and conventions
that permit the smooth running of social groups are in
different domains (Turiel, 1983), and that foregrounding
concerns about justice and caring, respectively,
may be gendered (Gilligan, 1982).
In the transcripts of the young people whom we
interviewed, we identified evidence of moral considerations
and reasoning. In the following example, the
young person with SCD reflects on another student’s
reaction to his being granted time out from a school
sports activity:
‘There was this certain boy, and he, erm, he doesn’t listen.
He was just like, he knew I’ve got sickle cell, but he doesn’t
take it in. Erm, and sometimes I’m really, really tired and
he was just like, erm, just like the teacher like when he was
pushing and pushing to do that and (do you know like
playing cricket) and I felt really tired and so I went to lie
down, and he would like throw, like keep on throwing the
ball at me like when I’m trying to rest.’
(Interview 31, black Caribbean male, 15 years of age)
When asked if the boy knew whether the young person
had SCD, our respondent replied that he did, and
when probed further about why the boy then behaved
so badly towards him, our respondent replied:
‘Because he, I think that, he just like thought it was a game,
so, like, this wasn’t the first time it happened, it had
happened before this.’
In this extract the young person with SCD indicated
that the other boy lacked a sense of decent behaviour
towards himas someonewith sickle cell. Ultimately he
was not able to work out why the other boy behaved
like this towards him, but added that ‘I would just like
something to happen so that people do take notice.’
This suggests that different domains within the overall
school ethos are intimately linked. The young person
appeared to question his own sense of moral development
because bullying (the domain of attitudes of
young people to one another) wasweakly addressed by
the school.
In the following extract another young person with
SCD reflected on the moral behaviour of a teacher:
‘I had a really bad sickle cell inmylegs, and I didn’t want to
leave the lesson, because I wanted to still stay, that’s why.
And I also asked the teacher if I could go and get water.
And he’s telling me, erm, no you can’t, you can’t have
water in the lab. And I said, can I have it outside the class? I
kept asking him and he just wouldn’t listen so I just stayed
and I sat there. And then another time with the same
teacher that I has a really bad pain in my arm, and I
thought like I’m going to go and get it [a drink of water],
I’m going to get it and I went and got it. And he was like ‘Where did you go?’ And I said I needed to go and get
water and you wouldn’t let me. And then he just left it,
because he knew that he was being unfair.’
(Interview 26, black African female, 15 years of age)
This young woman indicated that she experienced
sickle cell pain in class on more than one occasion, and
asked permission to leave the classroom to have a
drink of water in order to maintain her hydration.
Permission was denied, but after the second request
she left the classroom anyway. Upon her return she
was challenged by the teacher, but when she provided a
reasonable explanation for her absence, she suggested
that a sense of fairness prevented the teacher from
making negative comments or issuing any form of
punishment.
In the following final example, a young man sets out
the advice that he would give to teachers on dealing
with a young person with sickle cell in their class:
‘I wouldn’t tell them to treat them differently or like
telling them or treating them like children as if they’re
disabled, but allowing them to go to the toilet and to get a
drink and things like that. I think they should do that for
the whole of the school. But I think I know why they don’t
do that, because they’re trying to prevent truancy in the
school. Probably that’s probably one of the reasons. But
they need to consider both sides, I won’t say argument,
because it’s not an argument, but both sides of the story
from the different point of view, instead of just thinking
for the school’s benefit and less for the pupils’ benefit,
because the pupils’ benefit is the same as the school’s.’
(Interview 25, black African male, 15 years of age)
This young person would not like the school to treat
young people with SCD any differently from others,
for instance, as children, as less mature than their age,
or as disabled. In his view anyone, not only those with
SCD, should be allowed to go to the toilet during class.
However, he could accept that this might cause the
school authorities to worry about loss of control, make
it easier for some people to truant and more difficult
for the school to monitor everyone’s whereabouts.
He concluded by arguing that the school ought to be
organised around the needs of the students because
young people were the essential component of the
school.
In each of the three examples cited above the young
person with SCD showed an acute appreciation of
moral issues. They were at the receiving end of immoral
behaviour from others and inconsiderate behaviour
from teachers. They also showed a mature
awareness of the possible tension facing the school
staff between maintaining the conventions necessary
to the smooth running of the school and what might
constitute ethical behaviour towards the young person
living with SCD.
However, what did not appear anywhere in our
interview transcripts was a reference to any specific
moral curriculum, framework or ethos that informed
all social relationships within the school. This may be
because, at the time of devising questions for the
young people, we had not conceptualised school ethos
as important, and so did not ask direct questions
about this. It may be that none of the schools attended
by our interviewees had a fully articulated moral
education as part of their overall school ethos. This
may partially explain the recurrence of negative experiences
for young people with SCD even when the
school had been told about their condition. In the
absence of clear guidance on how moral education will
be covered, any attempt to evaluate its efficacy is at
best limited and at worst impossible. In contrast, a
positivist approach to school ethos through formal
expression of where, when and how moral development
might be incorporated in the curriculum has
the potential to be evaluated in terms of the young
person’s experience of school.
Cultural development
In the UK there has been concern for some time about
racism in schools (Tomlinson, 2008; Gillborn, 2008),
and the potential of those with long-standing chronic
illness to be disadvantaged in educational settings has
been highlighted (Lightfoot et al, 2001). Young people
with SCD may be at the centre of both of these
scenarios. The black parents in our case studies were
acutely aware of the possibility that their children
might not achieve their full potential because of the
negative expectations of their teachers regarding their
academic potential and/or poor behaviour or attendance.
The parents themselves might have experienced
racism in British schools where, in the past, young
black people were disproportionately represented in
special schools:
‘We were embarrassed as children because what they
showed us was negative. Africans with bones in their
nose, women in the jungle, because that is the message
that I was taught as a child in school.’
(Case Study 1)
Black parents may therefore be motivated to take an
especially close interest in what happens to their
children at school, quite apart from the usual parental
concern. Even in primary school where, overall, smaller
schools and more personal networks may make it
easier to sustain a positive ethos, lack of cultural
competency had a negative impact on the experience
of the child and carer:
‘The first school he went to, a primary school, we had
some problems with the teachers. That was really based on
the relationship between my husband and the teachers. It was a very white middle-class school, and as a black child
moving into the area we don’t feel ... I think they felt quite
threatened if I’m going to be blunt, about my husband, a
black man. They didn’t know how to deal with him; he
was asking a lot of questions, taking an interest – they
didn’t want to know. Yes? Which caused a lot of [friction]
in the school and we had to withdraw [name] out of the
school and found another school, erm, primary school
where he started to settle down.’
(Case Study 1, black Caribbean mother)
In this example, the predominantly white school did
not have the cultural competency to read the close
interest taken by the father in the context of the history
of discrimination in British schools, and instead it was
reported to have reacted negatively to his attentiveness,
choosing to view it as aggressive behaviour
Social development
The most straightforward element of social development
could be said to take place through extracurricular
activities, especially those that take young people
outside their immediate social environment and the
presence of their parents or usual carers. School ethos
can be judged by the extent to which all young people
are included in such activities. One of the main
vehicles for such social development is through the
school trip, which was described by our respondents
in both positive and negative terms. Some were
included in all school trips:
‘School trips, what about school trips, yeah, I went in
school trips. I remember I went to France in a school trip,
it was with my school and that was good. It was really
nice.’
(Interview 40, black African male, 21 years of age)
On the other hand, a number of young people with
SCD were excluded from certain school activities:
‘Anything outside I was not, I was not allowed to take part
in. I just have to stay back behind in the class. ... It makes
me feel sad you know, everybody is doing something, and
you are just looking out of the window seeing them
enjoying themselves, laughing and running around. And
then I amthere, pretending to read a book. And I think to
myself why I cannot be like them, why, why. And I think
why me with sickle cell.’
(Interview 32, black African male, 25 years of age)
This type of exclusion can have other consequences,
too, as the following extract suggests:
‘Once I wanted to go to a school trip, you know. And they
said, no, you cannot, and that the teacher would not allow
me to go. The teacher at that time, she is like well, no, I
cannot let you go because if something happened to you I
don’t know what to do with it, she would not like anything
to happen to me. So, I was upset for not going and participating in that trip. I really wanted to go, but what
can I do, she said no.’
(Interview 35, black African male, 17 years of age)
According to these accounts, preventing young people
with SCD from attending school trips or school sports
days caused feelings of social isolation, and led to
young people questioning the value of sharing information
about their SCD if it resulted in further
exclusion and discrimination. Even if specific activities
were unsuitable for young people with SCD, some
form of participation could be made possible, for
instance through helping with timing, videotaping
or reporting on events. Equality legislation requires
schools to facilitate the inclusion of young disabled
people, and could be used to develop a positive school
ethos for those with SCD.
Conclusion
Young people with SCD report that they undergo
negative experiences at school in relation to self-care.
An examination of the relationship between reported
exposure to negative experiences and the extent to
which teachers and/or other young people reputedly
know that a young person has SCD does not explain
the patterns observed. This paper attempted to explain
the diverse range of school experiences in other ways,
particularly in relation to school ethos. We suggest
that the relative experiences of young people with SCD
at school depend on such factors as whether or not the
school has coherent values that inform all aspects of
school life (including the attitudes of young people
and teachers to themselves and to each other), the
nature of the links between school and community,
and the extent to which spiritual, moral, cultural and
social development forms an integral part of the
school environment. Schools whose approach to behaviour
management makes it impossible for young
people to achieve their full potential contrast strongly
with those in which young people, parents and teachers
are deemed equal partners in achieving a positive
school experience. Thus the school’s approach to a
range of whole-school policies is a determinant of
school ethos, and may shed light on how an individual
experiences school, irrespective of whether or not they
disclose their SCD status. Schools that involve the
community in activities relating to the welfare and
education of children are shown to have a positive
impact on parents, for if a child with SCD is to experience
school positively, the school must also be experienced
positively by parents.
Further research might assess the transferability of
our ideas to other long-term conditions, examining
the possible role of school ethos in supporting young people with asthma, epilepsy and diabetes. Our work
also demonstrates the importance of thinking about
the school environment when talking about young
people and their health or illness, and of broadening
debates about diversity and health to include consideration
of the interaction of the school environment
and health.
ACKNOWLEDGEMENTS
This paper was funded by the Economic and Social
Research Council (Grant RES-000–23–1486). We are
grateful to all the young people and their families for
the interviews. We thank Hala Evans and Eileen
Buchanan for help with the data collection. We thank
all the healthcare and voluntary group staff for their
help in contacting research participants, especially
David Rees, Moira Dick, Susan Height, Sandra
O’Driscoll, Shirley Samuel, Baba Inusa, Jo Howard,
Helen Appleby, Neil Westerdale, Lola Oni, Elizabeth
Okuyiga, Vesna Graham, Beatrice Barbola, Gavin
Cho, Michele Afif, Lurieteen Miller, Susan Crawford,
Maureen Williams, Janet Lawrence, Paulette Gaskin,
Wendy Mills, Sekai Tangay, Bernice Burton, Comfort
Okolo, Evelyn Chibambo, Beverley Smalling, Anthony
Akhidenor, Mary Opare-Ababio, Joanne McLoughlin,
Iyamide Thomas, Comfort Ndive, Blanche McCalla,
Anthony Mason, Carol Nwosu, Cecilia Shoetan, Tito
Idowu, Eileen Bowen, Susan Mew, Beverley Bell-
Jessop, Maureen Scarlet, Monica Noel, Carol King,
Winston Nurse, Melita Dixon, Angela Dias, the late
Sonia Lindsay, Sharon Wilson, Anndeloris Chacon
and Marjorie Ritchie.
CONFLICTS OF INTEREST
None.
References
- Atkin K and Anionwu EN (2010) The Social Consequences of Sickle Cell and Thalassaemia: improving the quality of support. Better Health Briefing Paper 17. London: Race Equality Foundation.
- Bolman L and Deal T (1984) Modern Approaches to Understanding and Managing Organizations. San Francisco, CA: Jossey-Bass.
- Department for Children, Schools and Families (2010) Parental Involvement: the ethos of the school. www.standards.dfes.gov.uk/parentalinvolvement/hsa/ hsa_guidance/hsa_guidance_should2 (no longer available, last accessed 12 October 2010).
- Donnelly C (2000) In pursuit of school ethos. British Journal of Educational Studies 48:134ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â54.
- Dyson SM and Atkin K (2011) Sickle cell and thalassaemia: global public health issues come of age. Ethnicity and Health 16:299ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â311.
- Dyson SM, Atkin K, Culley LA et al (2010a) Disclosure and sickle cell disorder: a mixed methods study of the young person with sickle cell at school. Social Science and Medicine 70:2036ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â44.
- Dyson SM, Abuateya H, Atkin K et al (2010b) Reported school experiences of young people living with sickle cell disorder in England. British Educational Research Journal 36:125ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â42.
- Dyson SM, Atkin K, Culley LA et al (2011) Sickle cell, habitual dispositions and fragile dispositions: young people with sickle cell at school. Sociology of Health and Illness 33:465ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â83.
- Fielding N (1993) Qualitative interviewing. In: Gilbert N (ed.) Researching Social Life. London: Sage Publications. pp. 135ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â53.
- Gillborn D (2008) Racism and Education: coincidence or conspiracy? London: Routledge.
- Gilligan C (1982) In a Different Voice: psychological theory and womenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s development. Cambridge, MA: Harvard University Press.
- GloverDandColemanM(2005) School culture, climate and ethos: interchangeable or distinctive concepts? Journal of In- Service Education 31:251ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â71.
- Johnson LS (2003) The diversity imperative: building a culturally responsive school ethos. Intercultural Education 14:17ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â30.
- Karlsen S and Nazroo JY (2002) Agency and structure: the impact of ethnic identity and racism on the health of ethnic minority people. Sociology of Health and Illness 24:1ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â20.
- Kohlberg L and Turiel E (1971) Moral development and moral education. In: Lesser G (ed.) Psychology and Educational Practice. New York: Scott Foresman. pp. 530ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â50.
- Lee A (2009) Health-promoting schools: evidence for a holistic approach to promoting health and improving health literacy. Applied Health Economics and Health Policy 7:11ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â17.
- Lightfoot J, Muhkerjee S and Sloper P (2001) Supporting pupils with special health needs in mainstream schools: policy and practice. Children and Society 15:57ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â69.
- McLellan L, Rissel C, Donnelly N et al (1999) Health behaviour and the school environment in New South Wales, Australia. Social Science and Medicine 49:611ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â19.
- Moos RH (1979) Evaluating Educational Environments: procedures, measures, findings, and policy implications. San Francisco, CA: Jossey-Bass.
- Paasche-Orlow MK and Wolf MS (2010) Promoting health literacy research to reduce health disparities. Journal of Health Communication 15:34ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â41.
- Peterson KD and Deal T (1998) How leaders influence the culture of schools. Educational Leadership 56:28ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â30.
- Rutter M, Maughan B, Mortimore P et al (1979) Fifteen Thousand Hours: secondary school and their effects on children. Cambridge, MA: Harvard University Press.
- Smith E (2003) Ethos, habitus, and situation for learning. British Journal of Sociology of Education 24:463ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â71.
- Streetly A, Latinovic R and Henthorn J (2010) Implementation of universal newborn bloodspot screening for sickle cell disease and other clinically significant haemoglobinopathies in England: screening results for 2005ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â7. Journal of Clinical Pathology 62(1):26ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â30.
- Stuart B (1999) Spirituality and the secondary school curriculum. LACE Magazine Archive Issue 12. www.delasalle. org.uk/lace/LACE%20Magazine%20Archive.htm (accessed 8 July 2011). 44
- SE Dyson, K Atkin, L Culley et al Tomlinson S (2008) Race and Education: policy and politics in Britain. Maidenhead: Open University Press.
- Turiel E (1983) The Development of Social Knowledge: morality and convention. New York: Cambridge University Press.
- Williams DR, Neighbors HW and Jackson JS (2003) Racial/ ethnic discrimination and health: findings from community studies. American Journal of Public Health 93:200ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â 208.

