Keywords
Liver Neoplasms; Neoplasm Metastasis; Neuroendocrine Tumors; Pancreatectomy
Abbreviations
ENETS: European Neuroendocrine Tumor Society; PPPD: pylorus-preserving pancreaticoduodenectomy; TACE: trans-catheter arterial chemoembolization; TAE: transcatheter arterial embolization
INTRODUCTION
Pancreatic neuroendocrine tumors (pNETs) have been known as a rare subgroup of pancreatic tumors, though the increasing detection of incidental pNETs during imaging procedures is recently expected [1, 2]. All pNETs are regarded to have malignant potential. Once distant metastases occur, cure is highly unlikely, although the progression of tumor is usually slow [3]. Unfortunately, most of the pNETs have already metastatic lesions by the time they are diagnosed [4] and liver is the most common site of metastasis [5, 6]. The presence of liver metastasis is suggested to be one of the major prognostic factors in the patients with pNETs [7]. In prognostic studies, the data of digestive endocrine tumors are more available than those of pNETs only, and it has been demonstrated that the patients with liver metastasis have a significantly worse survival rate when compared to those without liver metastasis [8, 9, 10].
According to the National Comprehensive Cancer Network (NCCN) guideline for neuroendocrine tumors of the pancreas, trans-catheter arterial embolization (TAE), trans-catheter arterial chemoembolization (TACE), radioembolization, cytoreductive surgery, ablative therapy, systemic chemotherapy and/or molecular-targeted therapies with everolimus or sunitinib are recommended as the management of unresectable disease and/or distant metastases [11]. In the European Neuroendocrine Tumor Society (ENETS) consensus guidelines for unresectable liver metastases from digestive neuroendocrine tumors, chemotherapy, biotherapy with somatostatin analogues/ interferon-alpha, molecular-targeted therapies, peptide receptor radionuclide therapy, TAE and/or TACE are recommended as well [12]. Both of these guidelines have made no mention about surgery to the primary tumor. In ENETS consensus guidelines for well-differentiated pancreatic non-functioning tumors, recommendation of resection of primary pancreatic tumor for the selected patients is described without any reference evidences [13]. The efficacy of aggressive surgery to primary tumor has been still controversial in pNETs with unresectable metastasis [14], although resection of primary tumor is recommended in metastatic neuroendocrine tumors of the jejunum/ileum [15, 16].
Recently, molecular-targeted therapy with sunitinib, a multitargeted tyrosine kinase inhibitor, or everolimus, an oral inhibitor of mammalian target of rapamysin (mTOR), has been established in the treatment for the patients with unresectable pNETs [17, 18]. It should be known that most of the patients had previous surgical treatment including resection of primary pancreatic tumor in the studies of these novel agents [18, 19]. It may be important to consider a potential benefit of resection of primary pancreatic tumor in the multidisciplinary treatment of metastatic pNETs.
This paper presents four patients who had pNETs with unresectable synchronous liver metastases. We treated the patients with surgical resection of primary pancreatic tumors, intervention to the liver and systemic therapies. We would review literatures and discuss about a role of resection of primary pancreatic tumor in the patients of pNETs with unresectable synchronous liver metastases.
MATERIAL AND METHODS
We retrieved medical records and imaging studies of patients who had been histopathologically diagnosed as pNETs at National Hospital Organization Kyushu Cancer Center, Fukuoka City, Japan between April 2000 and March 2006. They included demographic data, pathology, treatment, short- and long-term outcome. The imaging data included computed tomography (CT) scans, magnetic resonance imaging (MRI), or ultrasonography (US). Then, we extracted the patients who had pNETs with unresectable synchronous liver metastases. Hepatic biopsy was performed in all patients, and liver metastases of pNETs was confirmed via immunohistochemical staining of chromogranin A and/or synaptophysin in biopsy samples. Immunohistochemical examinations of synaptophysin, somatostatin receptor type 2A and Ki67 were performed in surgical resected specimens later on the purpose of research. Somatostatin receptor type 2A staining was evaluated by using Volante’s scoring system [20]. Ki67 labeling index was countered.
We resected primary pancreatic tumors in the patients with unresectable synchronous liver metastases. Excluded criteria of pancreatectomy were the presence of unresectable primary tumor or extrahepatic metastases except for regional lymph node metastases. Then, TAE, TACE and/or hepatic arterial infusion were performed as hepatic regional treatments preoperatively. Postoperative trans-arterial hepatic treatments and/or systemic therapies were started as soon as possible. In patients who were treated with TAE, the hepatic artery was catheterized, and embolic agent was injected until substantial slowing of the blood flow was achieved. In patients who underwent TACE, the chemotherapeutic agent was administered followed by the embolic material. The treatments with TAE, TACE and/or hepatic arterial infusion were performed sequentially every 1-3 months. From the second treatment onward, the treatment agents were mainly injected via a reservoir which was connected with a catheter placed into the hepatic artery. The interval of trans-arterial treatment was based on the patient’s condition. The trans-arterial treatment was continued until when the arterial flow was changed because of arteritis rendering vascular reconstruction and the effects of treatment could not been expected. Follow-up examinations based on imaging studies were generally obtained every 3-6 months after the beginning of treatment.
ETHICS
Patients were managed according to the ethical guidelines of the “World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008. The written informed consent was obtained from each patient.
RESULTS
There were seven patients who were diagnosed to have histopathological pNETs in our institution between April 2000 and March 2006. Four patients (57.1%) had unresectable liver metastases at the time of initial diagnosis. All 4 patients were not excluded and received pancreatectomy. Three females and one male were included. The mean age was 54.0 years (range from 31 to 72 years). Primary pancreatic tumor located in the tail in three cases and in the head in one. The initial symptoms were abdominal discomfort in three cases and uncontrollable diabetes mellitus in one (Table 1).

In three patients, the diagnosis was made by staff pathologists from our institution based on histological and immunohistochemical examination of pathologic specimens. In one patient, histological examination of liver metastases was performed at an outside institution. The histopathological and immunohistochemical results were shown in Figure and Table 2. All cases showed the positive staining of chromogranin A and synaptophisin. Ki67 labeling index were smaller than 2% in Cases #1 and #2, that corresponded to grade 1 (G1) of the ENETS grading. Cases #3 and #4 were categorized in grade 2 (G2).
Figure 1. Microscopic images of three patients of pNETs (Cases #1, #2 and #3) who were diagnosed to have synchronous liver metastases at
our institution. 1a., 2a., and 3a. Atypical small round cells arranged in nests or sheets in a fibrous tissue containing residual liver
parenchyma in the liver specimens. 1b., 2b., and 3b. Diffuse immunoreactivity for chromogranin A in the tumor cells of liver biopsy
specimens. 1c., 2c., and 3c. Uniform cells proliferating in trabecular or solid pattern in the surgical resected specimens in the pancreas.
(Original magnifications 20x).

The surgical procedures performed were distal pancreatectomy with simultaneous splenectomy in three patients for tumors located in the tail of the pancreas, and pylorus-preserving pancreaticoduodenectomy (PPPD) in one for tumor located in the head. There were no operative deaths. Case #4, the patient who received PPPD, developed delayed gastric emptying that corresponded to grade C of the definition by International Study Group of Pancreatic Surgery (ISGPS) [21]. She discharged from hospital 38 days after surgery. The other patients had no significant postoperative complication (Table 3).
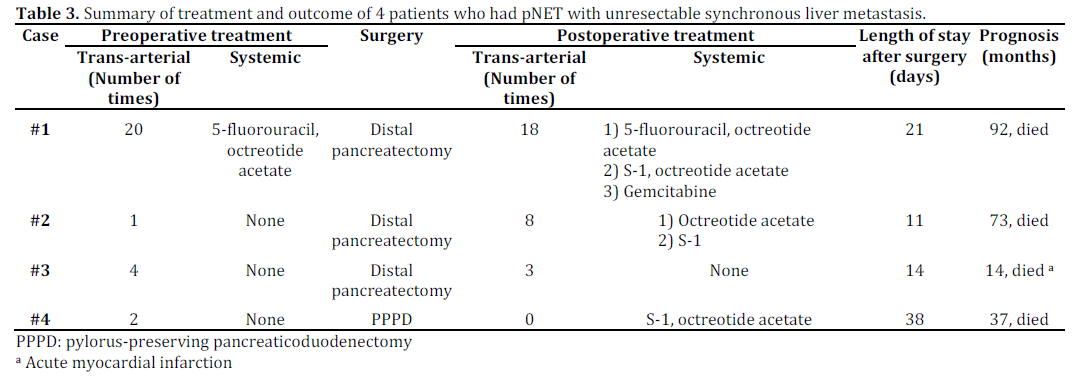
Timing of surgery was based on an evaluation of effect of trans-arterial treatments on liver metastases by the referring physicians. The maximum number of repetitions of preoperative trans-arterial treatment was 20 times in Case #1. Although the effect was evaluated as partially response, but generally insufficient until the 12th treatment because most of the hepatic tumors could not retain embolic agents due to the fast arterial flow through the tumors, the overall effect of embolization was recognized gradually after the subsequent sequential treatments. The patient received oral administration of 5-fluorouracil in addition to the trans-arterial treatment for the first two months in the beginning of treatment course. Postoperative trans-arterial treatments following the resection of primary pancreatic tumor were performed 18 times until arterial flow was changed. The change of arterial flow allowed trans-arterial agents flow into the thorax and resulted in forming an abscess of the thorax. The abscess could be treated by antibiotic agents for 4 weeks. Although the patient received systemic chemotherapy and biological therapy with octreotide acetate followed by regional hepatic treatment, she had progressive disease of multiple metastases and died 92 months after the first treatment. Case #2 had preoperative trans-arterial treatment one time and postoperative treatment 8 times. She received systemic chemotherapy with S-1 after the arterial flow was changed. She died 73 months after the first treatment. The patient of Case #3 who received preoperative trans-arterial treatment four times because the general condition was precarious, although the trans-arterial treatment seemed to be effective soon after the first treatment. Distal pancreatectomy was performed when the general condition was recovered. He had stable disease with postoperative trans-arterial treatments but died suddenly from acute myocardial infarction 14 months after the first treatment. In Case #4, the patient had PPPD following two times of transarterial treatment. She rejected postoperative transarterial treatment and received systemic chemotherapy and biological therapy with octreotide acetate. She died 37 months after the first treatment (Table 3). Three patients who were diagnosed to have localized pNETs in the same period have been still alive without recurrence more than 7 years after resection of pancreatic tumors.
DISCUSSION
Recently in Japan, a large epidemiological study using a nationwide stratified random sampling method has been reported by Ito et al. [22]. The study revealed that the prevalence of pNETs was estimated as 2.23 per 100,000 (95% CI: 1.93-2.76) and an annual onset incidence was 1.01 per 100,000 (95% CI: 0.88-1.25) in the year 2005. On the other hand, the annual incidences of pNETs in United States and Europe have been reported 0.12 and 0.4 per 100,000, respectively [1, 23]. It has been discussed that the results may be affected by prevalence of imaging studies for screening in Japan rather than racial difference [24]. The study also revealed that the incident rate of distant metastases including liver metastasis is 21% at the time of diagnosis [22]. The incident rate of synchronous liver metastasis from pNETs has been reported 27% in Korea [7] and 29% in Italy [25]. In the present study, the incidence of liver metastasis was 57% that is higher than the previous reported rates. However, we experienced other 5 cases of pNETs for recent two years and resectable synchronous liver metastasis was present in one case (20.0%). We excluded these 5 cases from the present study because of short follow-up periods (the median follow-up period was 9 months, range from 3 to 17). More accumulation of cases is needed to evaluate the incidence rate of synchronous liver metastases.
It has been clarified that surgical resection of localized pNETs is associated with improved survival [26]. In our series, 3 patients who were diagnosed to have localized pNETs and received surgical resection between 2000 and 2006 are still alive without recurrence. In the management of patients who had neuroendocrine tumors with resectable synchronous liver metastases and the absence of extrahepatic metastases, hepatectomy is acceptable because that patients with liver metastases from neuroendocrine tumors who underwent curative hepatic resection had a significantly longer survival than unresected patients [4, 27]. Even when recurrence of hepatic disease progresses in patients who initially underwent surgical extirpation of liver metastasis from neuroendocrine tumors, liver-directed therapy for hepatic metastasis prolongs survival [28]. Moreover, in the patients with hormonal and pain symptoms, surgical resection provide excellent palliation [29].
Resection of primary neuroendocrine tumor may provide patients with unresectable liver metastases with some benefits. First, resection of primary pancreatic tumor may prevent from some complications which are developed on disease progression [30]. For example, biliary obstruction, gastric outlet obstruction or gastrointestinal hemorrhage sometimes occur when tumors are located in the pancreatic head, and left-sided portal hypertension in the pancreatic tail [31, 32]. Therefore, we could manage with trans-arterial treatment and/or systemic treatment safer after resection of primary pancreatic tumors. Second, resection of primary tumor may be associated with improved the response to radiologic therapy in the treatment course. Gupta et al. investigated the predictive factor of radiologic response in the patients who had islet cell carcinomas with liver metastases and were treated with TAE or TACE. They demonstrated that patients with primary tumor resection had a higher radiologic response rate than patients without primary tumor resection. They also studied prognostic factor in patients with metastatic carcinoid tumors and pancreatic islet cell carcinomas who were treated with TAE or TACE. They demonstrated that resection of primary tumor was associated with improved overall survival [33]. Thus, there seems to be potential benefits of resection of primary pancreatic tumor in the process of multidisciplinary approach. However, Capurso et al. reviewed three cohort studies that compared resection with unresection of the primary pancreatic tumor in the patients who had pNETs with unresectable liver metastases, and suggested that there was a bias towards resection primary pancreatic tumor in patients with a better performance status or less advanced disease seems likely [34]. There are some risks in pancreatic resection. However, mortality rate of pancreatectomy has been decreased recently [35]. The Japanese Society of Gastroenterological Surgery reported on the internet that hospital mortality rates of pancreaticoduodenectomy and distal pancreatectomy for malignant diseases were 2.11% (127/6,027) and 0.99% (18/1,813) from 1,466 Japanese institutions in the year 2009. Gordon et al. showed hospital mortality rate of pancreaticoduodenectomy was 2.2% [36], and Brennan et al. reported operative mortality rate of distal pancreatectomy was 0% [37], respectively. Indication of pancreatectomy for the patients who had pNETs should be discussed under consideration of both their benefits and risks.
Once unresectable metastatic disease has occurred, it would become life-threatening sooner or later and cure would be unlikely. The mean survival of the patients who had pNETs with distant metastasis is 24 months [26]. As our strategies, we performed trans-arterial treatment prior to surgery in the patients who had pNETs with unresectable synchronous liver metastases and confirmed that the effect would be expected. Hung et al. reported a patient who had pNET with unresectable liver metastases, received pancreatectomy and died 84 months after the surgery [38]. The patient received TAE 6 and 12 months after the surgery and chemotherapy with streptozotocin and 5- fluorouracil after the 2-year follow-up. To our knowledge, this is the longest survivor with unresectable synchronous liver metastases that was described in detail in the literature. The patient of Case #1 received preoperative trans-arterial treatments for 18 months and died 74 months after surgery, so it was 92 months after the first TACE. The patient of Case #2 had preoperative transarterial treatments for 2 months and died 71 months after surgery, equally to 73 months after the first TACE. The long-term outcome of these two cases suggested that a combination of pre- and postoperative intervention to the liver with resection of primary pancreatic tumor has a potential to improve the survival. However, further studies will be needed to clarify the prognostic efficacy of perioperative trans-arterial treatment. Since neuroendocrine tumors usually are abundant in arterial flow, TACE seems to be more effective than TAE theoretically. However, there is no evidence that TACE is superior to TAE. Timing of sequential TACE and choice of treatment agents have still remained unclear [12]. Hepatobiliary complications of trans-arterial treatment are not seldom fatal but sometimes serious, for instances, liver abscess, gallbladder infarction or perforation, cholangitis and bile duct necrosis. Liver abscess may be likely to develop in association with bacterial infections following gastrectomy [39] or pancreaticoduodenectomy [40]. Systemic treatment rather than trans-arterial hepatic treatment following surgery might be recommended for the patients who had pNETs in the head of the pancreas.
Several systemic treatments such as somatostatin analogues/interferon-alpha, chemotherapy, molecular-targeted therapies with sunitinib or everolimus, and peptide receptor radionuclide therapy are commonly used to treat unresectable neuroendocrine tumors. Somatostatin analogues/interferon may be of value in patients with well-differentiated NET expressing somatostatin receptor type 2 subtypes, but data is not available in cases of liver metastases [12]. Since immunohistochemical examination of somatostatin receptor was not available routinely at our institution, strong expressions of somatostatin receptor type 2A in Cases #1 and #3 were confirmed even later. In the present series, the selection of patients might be inadequate in the respect of expression of somatostatin receptor, although we performed somatostatin analogue treatment besides trans-arterial treatment in Cases #1, #2 and #4.
In patients with advanced pNETs, moleculartargeted therapy with sunitinib or everolimus is associated with improved progression-free survival [17, 18]. Based on these studies, these agents may have not been considered as first-line therapeutic options. Because the efficacy and safety of these agents have been proven [41, 42] and new trails testing logical combinations of agents have been going on [43, 44], therapeutic strategies for the management of patients with advanced pNETs will be updated in sequence. On updating the management of patients with advanced pNETs, clinicians must be aware of the variety of treatments included surgical treatment. In a phase III trial of sunitinib in patients with advanced welldifferentiated pancreatic neuroendocrine tumors, 88% of patients who were treated with sunitinib had received previous surgical treatment [18].
Although there are no data about previous treatment in a phase III study of everolimus [17], 72% of patients in a phase II study received surgery as a prior treatment [19]. Surgical details were not available in these articles. Most of patients of these studies maybe received resection of primary pancreatic tumors. Role of resection of the primary pancreatic tumor in the multidisciplinary treatment of patients with unresectable synchronous liver metastases should be considered in future therapeutic strategies. Further studies will likely define the role of resection of primary pancreatic tumor.
CONCLUSION
Surgical resection of primary pancreatic neuroendocrine tumor would be considered as an optional treatment in the patients who had unresectable synchronous liver metastases with the absence of other distant metastases, because of a potential of slow progression of hepatic metastases under trans-arterial treatment and other systemic treatment. However, it should be offered for selected patients while more studies are made.
Conflict of interest
The authors have no potential conflict of interest
References
- Yao JC, Eisner MP, Leary C, Dagohoy C, Phan A, Rashid A, etal. Population-based study of islet cell carcinoma. Ann Surg Oncol2007; 14(12): 3492-500. [PMID 17896148]
- Cheema A, Weber J, Strosberg JR. Incidental detection ofpancreatic neuroendocrine tumors: an analysis of incidence andoutcomes. Ann Surg Oncol. 2012; 19(9):2932-6. [PMID22350605]
- Bosman FT, Carneiro Fatima, Hruban RH, Theise ND (Eds):WHO classification of tumours of the digestive system. (4thedition). IARC Press: Lyon 2010:322-6.
- Chen H, Hardacre JM, Uzar A, Cameron JL, Choti MA. Isolatedliver metastases from neuroendocrine tumors: does resectionprolong survival? J Am Coll Surg. 1998; 187(1):88-92. [PMID9660030]
- Chamberlain RS, Canes D, Brown KT, Saltz L, Jarnagin W,Fong Y, et al. Hepatic neuroendocrine metastases: doesintervention alter outcomes? J Am Coll Surg 2000; 190(4): 432-445. [PMID 10757381]
- Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715carcinoid tumors. Cancer 2003; 97(4): 934-9. [PMID 12569593]
- Oh TG, Chung MJ, Park JY, Bang SM, Park SW, Chung JB, et al.Prognostic factors and characteristics of pancreaticneuroendocrine tumors: single center experience. Yonsei Med J.2012; 53(5):944-51. [PMID 22869477]
- Panzuto F, Nasoni S, Falconi M, Corleto VD, Capurso G,Cassetta S, et al. Prognostic factors and survival in endocrinetumor patients: comparison between gastrointestinal andpancreatic localization. Endocr Relat Cancer 2005; 12(4):1083-92. [PMID 16322345]
- Madeira I, Terris B, Voss M, Denys A, Sauvanet A, Flejou JF, etal. Prognostic factors in patients with endocrine tumors of theduodenopancreatic area. Gut 1998; 43(3):422-7. [PMID9863490]
- Tomassetti P, Campana D, Piscitelli L, Casadei R, Santini D,Nori F, et al. Endocrine pancreatic tumors: factors correlatedwith survival. Ann Oncol 2005; 16(11):1806-10. [PMID16085691]
- National Comprehensive Cancer Network (NCCN) ClinicalPractice Guidelines in Oncology. Version 1.2012 Neuroendocrinetumors of the pancreas. https://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf
- Pavel M, Baudin E, Couvelard A, Krenning E, Öberg K,Steinmüller T, et al. ENETS Consensus Guidelines for themanagement of patients with liver and other distant metastasesfrom neuroendocrine neoplasms of foregut, midgut, hindgut, andunknown primary. Neuroendocrinology. 2012; 95(2):157-76.[PMID 22262022]
- Falconi M, Bartsch DK, Eriksson B, Klöppel G, Lopes JM,O'Connor JM, et al. ENETS Consensus Guidelines for themanagement of patients with digestive neuroendocrineneoplasms of the digestive system: well-differentiated pancreaticnon-functioning tumors. Neuroendocrinology. 2012; 95(2):120-34. [PMID 22261872]
- Kulke MH, Anthony LB, Bushnell DL, de Herder WW,Goldsmith SJ, Klimstra DS, et al. NANETS treatment guidelines:well-differentiated neuroendocrine tumors of the stomach andpancreas. Pancreas. 2010; 39(6):735-52. [PMID 20664472]
- Eriksson B, Klöppel G, Krenning E, Ahlman H, Plöckinger U,Wiedenmann B, et al. Consensus guidelines for the managementof patients with digestive neuroendocrine tumors--welldifferentiatedjejunal-ileal tumor/carcinoma.Neuroendocrinology. 2008; 87(1):8-19. [PMID 18097129]
- Boudreaux JP, Klimstra DS, Hassan MM, Woltering EA, JensenRT, Goldsmith SJ, et al. The NANETS consensus guideline for thediagnosis and management of neuroendocrine tumors: welldifferentiatedneuroendocrine tumors of the Jejunum, Ileum,Appendix, and Cecum. Pancreas. 2010; 39(6):753-66. [PMID20664473]
- Yao JC, Shah MH, Ito T, Bohas CL, Wolin EM, Van Cutsem E, etal. Everolimus for advanced pancreatic neuroendocrine tumors.N Engl J Med. 2011; 364(6):514-23. [PMID 21306238]
- Raymond E, Dahan L, Raoul JL, Bang YJ, Borbath I, Lombard-Bohas C, et al. Sunitinib malate for the treatment of pancreaticneuroendocrine tumors. N Engl J Med. 2011; 364(6):501-13.[PMID 21306237]
- Duran I, Kortmansky J, Singh D, Hirte H, Kocha W, Goss G, etal. A phase II clinical and pharmacodynamic study oftemsirolimus in advanced neuroendocrine carcinomas. Br JCancer. 2006; 95(9):1148-54. [PMID 17031397]
- Volante M, Brizzi MP, Faggiano A, La Rosa S, Rapa I, FerreroA, et al. Somatostatin receptor type 2A immunohistochemistry inneuroendocrine tumors: a proposal of scoring system correlatedwith somatostatin receptor scitigraphy. Mod Pathol 2007;20(11):1172-82. [PMID 17873898]
- Wente MN, Bassi C, Devenis C, Fingerhut A, Gouma DJ, IzbickiJR, et al. Delayd gastric emptying (DGE) after pancreatic surgery:a suggested definition by the International Study Group ofPancreatic Surgery (ISGPS). Surgery. 2007; 142(5):761-8. [PMID17981197]
- Ito T, Sasano H, Tanaka M, Osamura RY, Sasaki I, Kimura W,et al. Epidemiological study of gastroenteropancreaticneuroendocrine tumors in Japan. J Gastroenterol 2010;45(2):234-43. [PMID 20058030]
- Eriksson B, Oberg K: Neuroendocrine tumours of thepancreas. Br J Surg 2000; 87(2): 129-31. [PMID 10671915]
- Ito T, Tanaka M, Sasano H, Osamura YR, Sasaki I, Kimura W,et al. Preliminary results of a Japanese nationwide survey ofneuroendocrine gastrointestinal tumors. J Gastroenterol. 2007;42(6):497-500. [PMID 17671766]
- Zerbi A, Falconi M, Rindi G, Delle Fave G, Tomassetti P,Pasquali C, et al. Clinicopathological features of pancreaticendocrine tumors: a prospective multicenter study in Italy of 297sporadic cases. Am J Gastroenterol. 2010; 105(6):1421-9.[PMID:20087335]
- Hill JS, McPhee JT, McDade TP, Zhou Z, Sullivan ME, WhalenGF, et al. Pancreatic neuroendocrine tumors: the impact ofsurgical resection on survival. Cancer. 2009; 115(4):741-51.[PMID 19130464]
- Tsuchikawa T, Hirano S, Tanaka E, Kato K, Matsumoto J,Nakayama T, et al. Surgical strategy for liver metastases ofneuroendocrine tumors. Hepatogastroenterology. 2012;59(115):921-3. [PMID 22024223]
- Saxena A, Chua TC, Zhao J, Morris DL. Liver-directed therapyfor neuroendocrine neoplasm hepatic metastasis prolongssurvival following progression after initial surgery. J Surg Oncol.2012; 105(4):342-50. [PMID 22006355]
- Chamberlain RS, Canes D, Brown KT, Saltz L, Jarnagin W,Fong Y, et al. Hepatic neuroendocrine metastases: doesintervention alter outcomes? J Am Coll Surg. 2000; 190(4):432-45. [PMID 10757381]
- Solorzano CC, Lee JE, Pisters PW, Vauthey JN, Ayers GD, JeanME, et al. Nonfunctioning islet cell carcinoma of the pancreas:survival results in contemporary series of 163 patients. Surgery.2001; 130(6):1078-85. [PMID 11742342]
- Metz DC, Benjamin SB. Islet cell carcinoma of the pancreaspresenting as bleeding from isolated gastric varices. Report of acase and review of the literature. Dig Dis Sci. 1991; 36(2):241-4.[PMID 1846333]
- Yamaguchi T, Takahashi H, Kagawa R, Takeda R, Sakata S,Yamamoto M, et al. Nonfunctioning pancreatic endocrine tumorpresenting with hemorrhage from isolated gastric varices. AmSurg. 2005; 71(12):1027-30. [PMID 16447473]
- Gupta S, Johnson MM, Murthy R, Ahrar K, Wallace MJ, MadoffDC, et al. Hepatic arterial embolization and chemoembolizationfor the treatment of patients with metastatic neuroendocrinetumors: variables affecting response rates and survival. Cancer.2005; 104(8):1590-602. [PMID 16134179]
- Capurso G, Bettini R, Rinzivillo M, Boninsegna L, Fave GD,Falconi M. Role of resection of the primary pancreaticneuroendocrine tumour only in patients with unresectablemetastatic liver disease: a systematic review.Neuroendocrinology. 2011; 93(4):223-9. [PMID 21358176]
- Hung JS, Chang MC, Lee PH, Tien YW. Is surgery indicated forpatients with symptomatic nonfunctioning pancreaticneuroendocrine tumor and unresectable hepatic metastases?World J Surg. 2007; 31(12):2392-7. [PMID 17960455]
- Yeo CJ, Cameron JL, Lillemoe KD, Sitzmann JV, Hruban RH,Goodman SN, et al. Pancreaticoduodenectomy for cancer of thehead of the pancreas. 201 patients. Ann Surg 1995; 221:721-31.[PMID 7794076]
- Gordon TA, Burleyson GP, Tielsch JM, Cameron JL. The effectsof regionalization on cost and outcome for one general high-risksurgical procedure. Ann Surg 1995; 221:43-9. [PMID 7826160]
- Brennan MF, Moccia RD, Klimstra D. Management ofadenocarcinoma of the body and tail of the pancreas. Ann Surg1996; 223: 506-11. [PMID 8651741]
- Chen C, Tsang YM, Hsueh PR, Huang GT, Yang PM, Sheu JC, etal. Bacterial infections associated with hepatic arteriography andtransarterial embolization for hepatocellular carcinoma: aprospective study. Clin Infect Dis. 1999; 29(1):161-6. [PMID10433580]
- Ishikawa O, Ohigashi H, Yasuda T, Shibata T, Sasaki Y,Kameyama M, et al. Transarterial chemoembolization inmetastatic liver tumor after curative resection of pancreaticcancer. (Article in Japanese) Gan To Kagaku Ryoho. 1988; 15(8 Pt2):2505-9. [PMID 2843113]
- Oberstein PE, Saif MW. Safety and efficacy of everolimus in adult patients with neuroendocrine tumors. Clin Med Insights Oncol. 2012; 6:41-51. [PMID 22253554]
- Raymond E, Hammel P, Dreyer C, Maatescu C, Hentic O, Ruszniewski P, et al. Sunitinib in pancreatic neuroendocrine tumors. Target Oncol. 2012; 7(2):117-25. [PMID 22661319]
- Oberstein PE, Remotti H, Saif MW, Libutti SK. Pancreatic neuroendocrine tumors: entering a new era. JOP. 2012; 13(2):169-73. [PMID 22406593]
- Oberstein PE, Saif MW. Update on novel therapies for pancreatic neuroendocrine tumors. JOP. 2012; 13(4):372-5. [PMID 22797392]


