Keywords
Octreotide; Pancreas
Abbreviations
POPF Post-Operative Pancreatic Fistula; PD Pancreaticoduodenectomy; OG Octreotide Group; NOG No Octreotide Group
INTRODUCTION
The prophylactic use of Somatostatin analogue is controversial in pancreatic surgery. Octreotide reduces pancreatic exocrine secretion and is used by many pancreatic surgeons in an attempt to reduce pancreatic fistula formation following proximal pancreatic resection [1]. However, Octreotide also reduces portal perfusion and decreases gastrointestinal motility which may have a direct adverse effect on a newly formed anastomosis [2].
Randomised controlled trials from Europe [3, 4] and USA [5-7] have questioned the efficacy of analogues for the prevention of complications and a study in 2012 showed that the prophylactic use of Octreotide did not reduce the clinical severity of Post-Operative Pancreatic leak once a fistula has been established [8]. A recent multicentre retrospective analysis of 1018 patients from 4 institutions undergoing PD found an increased rate of POPF when prophylactic Octreotide was used [9].
Meta-analysis studying the use Somatostatin and its analogues in pancreatic surgery also find apparently conflicting results. A meta-analysis from China published in 2008 looking at 8 individual studies found that the use of Octreotide did not significantly reduce postoperative complications after Pancreaticoduodenectomy [10]. In contrast, a meta-analysis and Cochrane review in 2010 looking at 17 randomised controlled studies with 2143 patients concluded that perioperative use of Somatostatin analogue reduced perioperative morbidity but didn’t have any influence on mortality [11].
The objective of this study was to evaluate the effect of prophylactic use of Octreotide on prevention and severity of complications in a large cohort of patients and evaluate the cost effectiveness of using this drug.
METHODS
In our unit all clinical data is prospectively collected in a dedicated Hepatico-pancreatic and Biliary (HpB) database. This was extensively searched for all patients undergoing Whipples’s Pancreaticoduodenectomy (PD) between 2003 and 2013.
Clinical practice varies slightly within the unit whereby some surgeons use prophylactic Octreotide routinely for all patients, another surgeon never uses prophylactic Octreotide and a further surgeon uses Octreotide selectively in patients where a soft pancreas and or small pancreatic duct are found at operation. All patients undergoing PD by the surgeon who selectively uses Octreotide, were excluded from the analysis to reduce the bias in the two groups. Patients in whom a Pancreatico-gastrostomy anastomosis was fashioned were also excluded.
In total, 456 patients were included in the analysis. Patients included had a Whipples’s PD with Pancreaticojejunostomy fashioned in two layers and had surgical drains placed at or near the anastomosis. Drain effluent was routinely collected from each drain starting on the 3rd post-operative day and analysed for total amylase level. The definition and severity of Pancreatic Leak was based on the ISGPF classification, defined as positive for pancreatic fistula when a drain Amylase level of more than three times the normal serum upper limit (>300U/L) from the 3rd day post-surgery onwards was detected [12, 13]. Patients undergoing Whipple’s PD by surgeons who routinely used prophylactic Octreotide (OG, n=255), were given subcutaneous administration of 200 mcg Octreotide twice or three times daily peri-operatively for 5-10 days in an effort to prevent pancreatic leaks and were compared to patients having no Octreotide administration (NOG, n=201).
Once patients were diagnosed with a pancreatic fistula, if they were receiving Prophylactic Octreotide this was continued as a continuous IV infusion at a dose of 200μg/ hour and Total Parenteral Nutrition instituted until the fistula stopped or the Amylase level in the fluid became less than 300U/L. Patients who were not receiving Octreotide when the fistula was detected were given the same treatment if the volume of fistula effluent was greater than 50mls/24hours and/or the patient displayed any of the following signs of systemic upset; pyrexia, elevated white cell count, high volume nasogastric effluent, abdominal pain.
All results are expressed as median and ranges. The Mann-Whitney U test was applied to compare nonparametric data, and the chi-squared test or Fisher’s exact test was applied for analysis of categorical variables. The level of statistical significance was set at p<0.05.
RESULTS
As depicted in Table 1, there were no significant differences in the Mean or Range of Age, Sex, Diagnosis between the two groups at the time of surgery. There was significantly less peri-operative morbidity and overall days hospital stay in the NOG group vs. the OG group (Any Complication OG 126 vs. NOG 59 p=0.001; Inpatient Stay days OG 20.29 days vs. NOG 17.90 days p=0.001); Table 2. There was a trend for lower 30 day mortality in the NOG but this difference was not significant (OG 2.35% vs. NOG 1.49% p=0.190). The overall Mortality in our total cohort of patients was 1.97%.


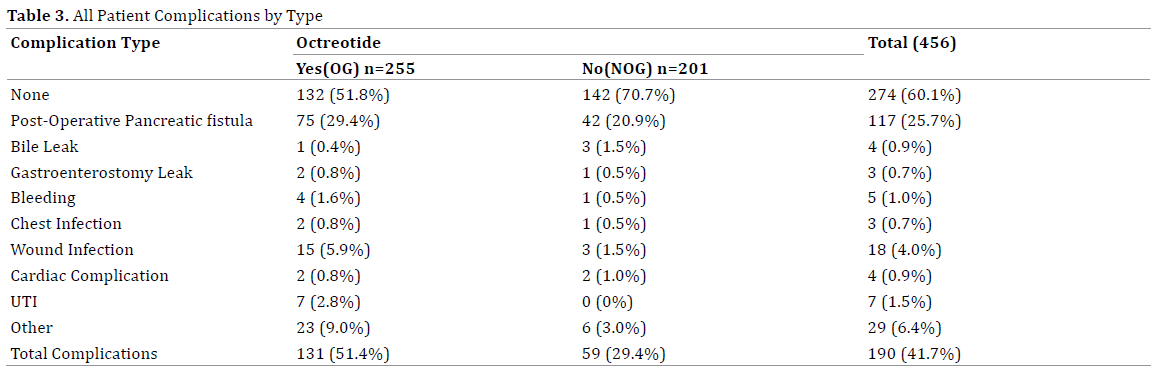
All complications and frequency of complication for both groups are listed in Table 3. Pancreatic leak was the most common recorded complication in either group. It should be noted that a small number of patients had more than one complication.
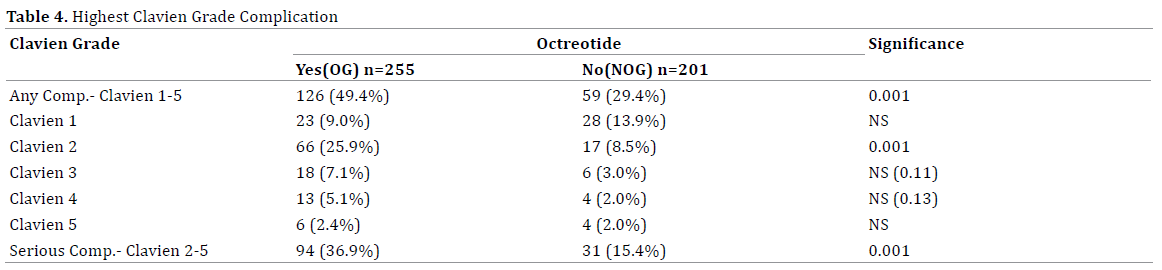
Complications were graded in severity using the Clavien system [14] and are displayed in Table 4. For patients with multiple complications, the most serious complication was used for Clavien scoring. With exception of Clavien Grade 2 complications which were significantly more frequent in the OG cohort, there were no significant differences in the frequency of complication in other individual Clavien Grades. However, overall complications (any Clavien Grade OG 126 vs. NOG 59 p=0.001) and serious complications (Clavien Grade 2-5 OG 94 vs. NOG 31 p=0.001) were significantly higher in the OG vs. NOG.
When POPF occurred in this series, they were segregated into two broad categories, clinically significant or strictly biochemical fistulae and graded A, B or C as defined by ISPGF [12]. Clinically significant fistulae were defined as leaks whereby the volume of fistula effluent was greater than 50mls/24hours and/or the patient displayed pyrexia, elevated white cell count, high volume nasogastric effluent, or abdominal pain. Biochemical fistulae (Grade A) were transient and asymptomatic, characterized only by elevated drain amylase levels and had no significant clinical sequelae [12, 13]. In contrast, clinically significant POPF (Grades B and C) were more morbid and required deviation from normal clinical management. Grade B fistulae (therapeutic medical management) require treatment with antibiotics or Octreotide infusion and Total Parenteral Nutrition (TPN). Grade C fistulae are defined as requiring more invasive intervention in the form of an operative intervention under general anaesthesia, percutaneous radiological insertion of drain with return to ICU for intense management. These particularly severe fistulae can also develop to sepsis, organ failure or death [12].
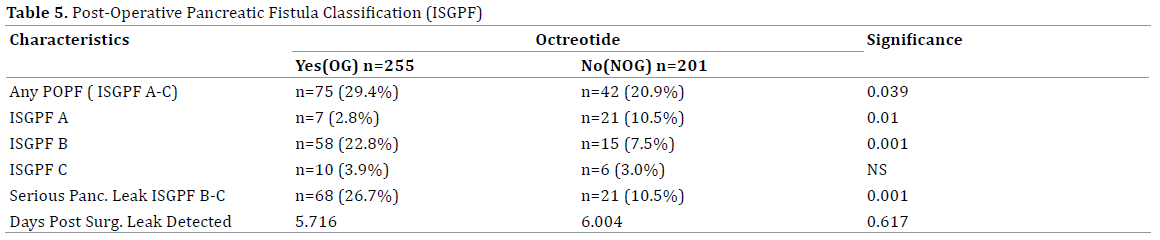
The timing of pancreatic leak detection and pancreatic leak severity are depicted in Table 5; interestingly there was no delay in pancreatic leak detection when prophylactic Octreotide was given (Days post surgery leak detected OG 5.7 vs. NOG 6.0). Most of the pancreatic leaks in the NOG required no treatment or deviation from normal post-operative recovery practice (ISGPF A OG 7 vs. NOG 21 p=0.01). In addition, Pancreatic leaks were significantly more common overall and were deemed more serious by ISGPF classification when Octreotide was used prophylactically then when it was not used (ISGPF A-C OG 75 vs. NOG 42 p=0.039; Serious Leak (ISGPF B-C OG 68 vs. NOG 21 p=0.001).
The total cost of using prophylactic Octreotide has also been calculated. When combining the cost of an additional 2.37 days inpatient stay with that of the pharmaceutical agent, patients receiving Octreotide were $3555 each more expensive to treat just for the inpatient hospital stay, than patients who did not receive Octreotide. The extra expense to the hospital for the entire cohort was $906,525 with a daily expenditure of $1500 per day on an average
DISCUSSION
In this study, patients were well matched with regards to Age, Sex, ASA grade, and type of tumour. The surgical experience and practise of all the surgeons’ involved as well as total operative time was also similar in both arms of the study. Our study has the limitations of being a retrospective analysis of prospectively collected data stored in a dedicated HpB database. The characteristics of the Pancreas itself, for example consistency (soft, brittle or firm) or pancreatic duct diameter (small, medium or large) were not taken into account due to the subjective nature of measurement between surgeons but we feel should be well controlled given the large cohort size. In this study, we have used the most stringent definition of pancreatic leak whereby drain fluid effluent collected daily, no matter how small the volume, was analysed biochemically for Amylase level and reported positive when Amylase levels were found to be three times greater than normal serum Amylase (>300μMol/L).
The prophylactic use of Somatostatin analogue in pancreatic resection surgery has remained an issue of constant debate and has been employed empirically as a method of preventing post-operative fistula since 1979 [1]. The findings of our study reveal that the use of prophylactic Octreotide does not prevent significant complications including pancreatic leak. On the contrary its use was associated with increased overall complication rates and severity of complication as well as increased hospital stay and expense. This is a similar finding to another multi-institutional retrospective study analysing 1018 PD from 2001-2013 which found POPF rate of 21% vs. 7% and 2 day prolonged in hospital stay when Octreotide prophylaxis was given [9]. Octreotride reduces splachnic blood flow mirrored as decreased mucosal blood flow is well established. We feel that the alteration of gastrointestinal motility coupled with altered perfusion of the anastomosis with Octreotide probably causes ischemia and congestion, adversely affecting the newly fashioned pancreatico-jejunal anastomosis contributing to leakage and outweighs any benefit of reducing pancreatic exocrine secretion
We have shown that low cardiopulmonary reserve is a risk factor for pancreatic leak following Pancreaticoduodenectomy [15]. Several other studies have looked at other patient factors responsible for the post operative pancreatic fistula and have suggested various variables like age more than 60 years [16-18], female sex, coronary artery disease, diabetes mellitus [18] as risk factors. Surgeon related risk factors in the univariate model include operative time, blood loss, amount of transfusion and dissection [18]. Tissue organ related factors such as soft pancreas, diagnosis other than pancreatic cancer [18] and pancreatic duct diameter [17] have been implicated. However it is interesting to note that most of these studies do not show a significant difference in the multivariate model with only obvious factors like coronary artery disease and texture of pancreas being significant [16, 18-21]. Another retrospective study from Korea showed using a multivariate regression model, that prophylactic Octreotide, combined gastrectomy and cellular origin of disease increased the frequency of pancreatic fistula [22].
There have been at least 5 randomly controlled trials (RCT) which have clearly discouraged the use of Somatostatin analogues [2-6]. In spite of this, Octreotide is still fairly commonly used in various HpB tertiary referral centres, including our own. Fear of pancreatic leak has led to varied practise in the use of Somatostatin analogue and its dose. Few surgeons follow a selective approach of using Octreotide to switch off the pancreas in order to avoid any pancreatic leak when the pancreatic anastomosis is precarious [23]. The effect of prophylactic Octreotide on the incidence of delayed gastric emptying has also been studied in a RCT in Switzerland. That study concluded that prophylactic Octreotide did not influence gastric emptying or reduce pancreatic fistula [24].
A meta-analysis including 1918 patients concluded that Somatostatin analogue reduced the rate of biochemical fistula but not the incidence of clinical anastomotic disruption. The study recommended using prophylactic Octreotide but noted that the numbers needed to treat to prevent a single pancreatic biochemical leak, was nine patients [25]. The limitation of this meta-analysis was the heterogeneity in the study and also the lack of standardisation of leak criteria. A more recent metaanalysis including 17 trials and 2143 patients concluded that Somatostatin analogues reduce post-operative complications but did not alter post-operative mortality [10].
Another systematic review and meta-analysis from Toronto involving 1359 patients suggested there is a significant reduction in the incidence of pancreatic fistula after Pancreatic Surgery [26] with Somatostatin analogue use. This review included 5 studies in favour of Somatostatin analogues [27-32] and only 2 studies against its use [4, 5]. The sub group analysis of this review found that the 2 studies where Octreotide was not found to be beneficial came from single centre high volume units in the USA with low overall pancreatic fistula rate of 6-9% in the no Octreotide arms. The 5 studies which favoured Octreotide usage all came from smaller European Centres where the leak rate was much higher and ranged from 19- 37% in the placebo arm of the trials [19-24].
Economic evaluation of the use of prophylactic Octreotide has also been looked at in a few studies with mixed conclusions. One study found an average saving of $1642 per patient with Octreotide usage suggesting its use in patients with high risk of development of fistula and in patients with no contraindications to its use [33]. Another recent study suggested that the indiscriminate use of Octreotide resulted in an over spending of about $781 per patient but suggested that using it selectively in patients with high risk of leak significantly decreased costs resulting in an overall cost saving [23]. Attempts to define high risk glands have been done but no validated scoring system has been developed yet [23, 24]. In our study the significant increase in the hospital stay and complication rate with indiscriminate Octreotide usage prophylactically, translated to a cost saving for the NOG group
CONCLUSION
In our unit, routine prophylactic Octreotide given at a dose of 200μg twice or three times daily for Whipple’s resection did not prevent post-operative pancreatic leak rates and is associated with increased frequency and more severe fistula formation. In this study, prophylactic Octreotide was also associated with increased overall morbidity, inpatient hospital stay and cost of hospitalisation. OG group had overall morbidity of 51.4% with significant morbidity of 36% as compared to NOG group which had a overall morbidity of 29.3% and significant morbidity of 15% respectively. The OG group also had serious fistulae (ISGPF B&C) incidence of 26.7% as compared to 10.5% in the NOG group. Patients receiving Octreotide were $3555 more expensive to treat on an average. The conflicting outcomes of trials till date, suggests the need for higher level of evidence regarding the usage of prophylactic Octreotide [34, 35]. It appears that the use of prophylactic use of Octreotride is not doing any good but a higher level of evidence is required to resolve the issue of effect on morbidity and cost-effectiveness of Somatostatin analogues in pancreatic surgery.
Conflict of interest
All the authors have no conflicts of interest
References
- Klempa I, Schwedes U, Usadel KH. [Prevention of postoperative pancreatic complications following duodenopancreatectomy using somatostatin].Der Chirurg; Zeitschrift fur alleGebiete der operativenMedizen 1979;50:427-31. [PMID: 477469]
- Foxx-Orenstein A, Camilleri M, Stephens D, Burton D. Effect of a somatostatin analogue on gastric motor and sensory functions in healthy humans. Gut 2003;52:1555-61. [PMID: 14570722]
- Suc B, Msika S, Piccinini M, Fourtanier G, Hay JM, Flamant Y, et al. Octreotide in the prevention of intra-abdominal complications following elective pancreatic resection: a prospective, multicenter randomized controlled trial. Archives of surgery 2004;139:288-94; discussion 95. [PMID: 15006886]
- Hesse UJ, DeDecker C, Houtmeyers P, Demetter P, Ceelen W, Pattyn P, et al. Prospectively randomized trial using perioperative low-dose octreotide to prevent organ-related and general complications after pancreatic surgery and pancreatico-jejunostomy. World journal of surgery 2005;29:1325-8. [PMID: 16132406]
- Lowy AM, Lee JE, Pisters PW, Davidson BS, Fenoglio CJ, Stanford P, et al. Prospective, randomized trial of octreotide to prevent pancreatic fistula after pancreaticoduodenectomy for malignant disease. Ann Surg 1997;226:632-41. [PMID: 9389397]
- Yeo CJ, Cameron JL, Lillemoe KD, Sauter PK, Coleman J, Sohn TA, et al. Does prophylactic octreotide decrease the rates of pancreatic fistula and other complications after pancreaticoduodenectomy? Results of a prospective randomized placebo-controlled trial. Ann Surg 2000;232:419-29. [PMID: 10973392]
- Sarr MG, Pancreatic Surgery G. The potent somatostatin analogue vapreotide does not decrease pancreas-specific complications after elective pancreatectomy: a prospective, multicenter, double-blinded, randomized, placebo-controlled trial. J Am CollSurg 2003;196:556-64; discussion 64-5; author reply 65. [PMID: 12691930]
- Droeser RA, Jeanmonod P, Schuld J, Moussavian MR, Schilling MK, Kollmar O. Octreotide prophylaxis is not beneficial for biochemical activity and clinical severity of postoperative pancreatic fistula after pancreatic surgery. Digestive surgery 2012;29:484-91. [PMID: 23392293]
- McMillan MT, Christein JD, Callery MP, Behrman SW, Drebin JA, Kent TS, Miller BC, et al. Prophylactic octreotide for pancreatoduodenectomy: more harm than good? HPB 2014. [PMID: 25041506]
- Zeng Q, Zhang Q, Han S, Yu Z, Zheng M, Zhou M, et al. Efficacy of somatostatin and its analogues in prevention of postoperative complications after pancreaticoduodenectomy: a meta-analysis of randomized controlled trials. Pancreas 2008;36:18-25. [PMID: 18192875]
- Koti RS, Gurusamy KS, Fusai G, Davidson BR. Meta-analysis of randomized controlled trials on the effectiveness of somatostatin analogues for pancreatic surgery: a Cochrane review. HPB: the official journal of the International HepatoPancreato Biliary Association 2010;12:155-65. [PMID: 20590882]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J et al. International Study Group on Pancreatic Fistula Definition. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005;138:8-13. [PMID: 16003309]
- Pratt WB, Maithel SK, Vanounou T, Huang ZS, Callery MP, Vollmer CM, Jr. Clinical and economic validation of the International Study Group of Pancreatic Fistula (ISGPF) classification scheme. Ann Surg 2007; 245:443–451. [PMID: 17435552]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications.A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240:205-13. [PMID: 15273542]
- Ausania F, Snowden CP, Prentis JM, Holmes LR, Jaques BC, White SA, et al. Effects of low cardiopulmonary reserve on pancreatic leak following pancreaticoduodenectomy. British Journal of Surgery 2012;99:1290-4. [PMID: 22828960]
- Han SL, Zheng XF, Shen X, Liu Z, Li JL, Lan SH, et al. Analysis of procedure-related complications after pancreatodoudenectomy. The Indian journal of surgery 2010;72:194-9. [PMID: 23133246]
- Choe YM, Lee KY, Oh CA, Lee JB, Choi SK, Hur YS, et al. Risk factors affecting pancreatic fistulas after pancreaticoduodenectomy. World journal of gastroenterology : WJG 2008;14:6970-4.[PMCID: PMC2773861]
- Lin JW, Cameron JL, Yeo CJ, Riall TS, Lillemoe KD.Risk factors and outcomes in postpancreaticoduodenectomypancreaticocutaneous fistula. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract 2004;8:951-9. [PMID: 15585382]
- Wellner UF, Kayser G, Lapshyn H, Sick O, Makowiec F, Hoppner J, et al. A simple scoring system based on clinical factors related to pancreatic texture predicts postoperative pancreatic fistula preoperatively. HPB: the official journal of the International HepatoPancreato Biliary Association 2010;12:696-702. [PMID: 21083795]
- Schmidt CM, Choi J, Powell ES, Yiannoutsos CT, Zyromski NJ, Nakeeb A, et al. Pancreatic fistula following pancreaticoduodenectomy: clinical predictors and patient outcomes. HPB surgery: a world journal of hepatic, pancreatic and biliary surgery 2009;2009:404520. [PMID: 19461951]
- Yang YM, Tian XD, Zhuang Y, Wang WM, Wan YL, Huang YT. Risk factors of pancreatic leakage after pancreaticoduodenectomy.World journal of gastroenterology 2005;11:2456-61. [PMID: 15832417]
- Moon HJ, Heo JS, Choi SH, Joh JW, Choi DW, Kim YI. The efficacy of the prophylactic use of octreotide after a pancreaticoduodenectomy.Yonsei Med J 2005;46:788-93. [PMID: 16385654]
- Vanounou T, Pratt WB, Callery MP, Vollmer CM, Jr. Selective administration of prophylactic octreotide during pancreaticoduodenectomy: a clinical and cost-benefit analysis in low- and high-risk glands. J Am CollSurg 2007;205:546-57. [PMID: 17903728]
- Kollmar O, Moussavian MR, Richter S, de Roi P, Maurer CA, Schilling MK. Prophylactic octreotide and delayed gastric emptying after pancreaticoduodenectomy: results of a prospective randomized double-blinded placebo-controlled trial. European journal of surgical oncology: the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology 2008; 34:868-75. [PMID: 18299182]
- Connor S, Alexakis N, Garden OJ, Leandros E, Bramis J, Wigmore SJ. Meta-analysis of the value of somatostatin and its analogues in reducing complications associated with pancreatic surgery. The British journal of surgery 2005;92:1059-67. [PMID: 16044410]
- Alghamdi AA, Jawas AM, Hart RS. Use of octreotide for the prevention of pancreatic fistula after elective pancreatic surgery: a systematic review and meta-analysis. Can J Surg 2007;50:459-66. [PMID: 18053374]
- Gouillat C, Gigot JF. Pancreatic surgical complications--the case for prophylaxis. Gut 2001; 49:iv32-9. [PMID: 11878792]
- Montorsi M, Zago M, Mosca F, Capussotti L, Zotti E, Ribotta G, et al. Efficacy of octreotide in the prevention of pancreatic fistula after elective pancreatic resections: a prospective, controlled, randomized clinical trial. Surgery 1995;117:26-31. [PMID: 7809832]
- Buchler M, Friess H, Klempa I, Hermanek P, Sulkowski U, Becker H, et al. Role of octreotide in the prevention of postoperative complications following pancreatic resection. American journal of surgery 1992;163:125-30; discussion 30-1. [PMID: 1733360]
- Pederzoli P, Bassi C, Falconi M, Camboni MG. Efficacy of octreotide in the prevention of complications of elective pancreatic surgery. Italian Study Group. The British journal of surgery 1994;81:265-9. [PMID: 8156354]
- Friess H, Beger HG, Sulkowski U, Becker H, Hofbauer B, Dennler HJ, et al. Randomized controlled multicentre study of the prevention of complications by octreotide in patients undergoing surgery for chronic pancreatitis.The British journal of surgery 1995;82:1270-3. [PMID: 7552016]
- Shan YS, Sy ED, Lin PW. Role of somatostatin in the prevention of pancreatic stump-related morbidity following elective pancreaticoduodenectomy in high-risk patients and elimination of surgeon-related factors: prospective, randomized, controlled trial. World journal of surgery 2003;27:709-14. [PMID: 12732998]
- Rosenberg L, MacNeil P, Turcotte L. Economic evaluation of the use of octreotide for prevention of complications following pancreatic resection. Journal of gastrointestinal surgery : official journal of the Society for Surgery of the Alimentary Tract 1999;3:225-32. [PMID: 10481115]
- Yamamoto Y, Sakamoto Y, Nara S, Esaki M, Shimada K, Kosuge T. A preoperative predictive scoring system for postoperative pancreatic fistula after pancreaticoduodenectomy.World journal of surgery 2011;35:2747-55. [PMID: 21913138]
- Poon RT, Lo SH, Fong D, Fan ST, Wong J. Prevention of pancreatic anastomotic leakage after pancreaticoduodenectomy. American journal of surgery 2002;183:42-52. [PMID: 11869701]

