Keywords
Cholangiopancreatography, Endoscopic Retrograde; Pancreatitis /prevention and control; Stents
Post-ERCP pancreatitis remains the most common complication of ERCP, and is one which can occasionally be devastating or fatal. Once thought to be unpredictable and inevitable, pancreatitis after ERCP has been the subject of evolved understanding. Increasingly, combinations of patient and procedure-related risk factors allow fairly accurate prediction of likelihood that an individual patient will develop pancreatitis [1, 2, 3, 4, 5, 6, 7, 8]. Careful endoscopic cannulation and therapeutic technique only go so far in preventing pancreatitis, and are not alone adequate to prevent this complication. Pharmacologic prevention is either ineffective or impractical [2].
Placement of trans-sphincteric pancreatic stents is a relatively new and increasingly adopted approach to reduce the risk of post- ERCP pancreatitis. The mechanism by which they work is not clearly understood. In theory, stents serve to preserve flow of pancreatic juice after pancreatic sphincter instrumentation, and/or to empty the gland of reactive enzyme substrate. According to this “plumbing” concept, drainage of manipulated pancreatic ducts prevents pancreatitis just as drainage of obstructed bile ducts prevents cholangitis. While the evidence accumulates from increasing numbers of studies at tertiary centers that placement of pancreatic stents is a highly effective method to reduce the incidence and severity of post-ERCP pancreatitis, and this practice has become standard at many large referral centers in the United States and elsewhere, the adoption of pancreatic stenting into community practice and even some advanced centers has been limited.
Many issues remain unanswered:
• Which individual patients are at sufficiently high risk to warrant a stent?
• What are the consequences of failure at attempted stent placement?
• Are success rates and efficacy of pancreatic stent placement as good in the hands of those with limited experience?
• And how serious and preventable is the risk of inducing pancreatic duct injury by placement of a stent?
• Finally, should this technique become standard for all endoscopists or should it be limited to tertiary centers?
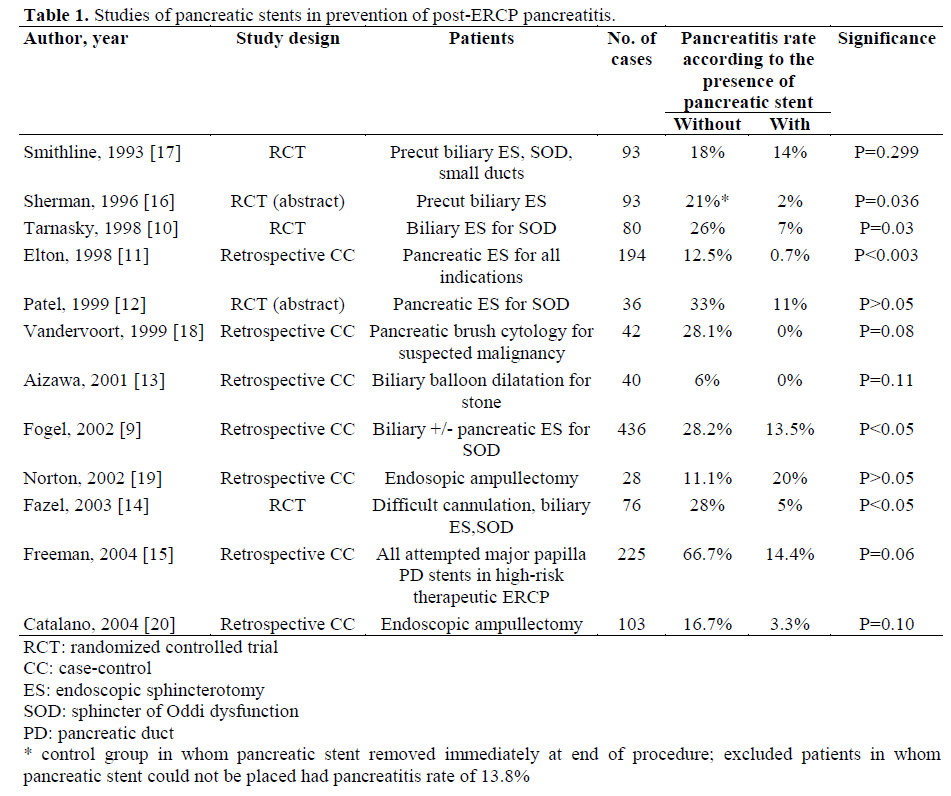
The evidence that pancreatic stent placement reduces rates of post-ERCP pancreatitis in high risk patients is substantial. Five prospective randomized controlled trials (three published in final form) and at least seven case-control studies have compared rates of pancreatitis after ERCP with and without a pancreatic stent (Table 1) [9, 10,11, 12, 13, 14, 15, 16, 17, 18, 19, 20]. These studies involved mixed high-risk groups including precut sphincterotomy, sphincter of Oddi dysfunction, difficult cannulation, pancreatic sphincterotomy, biliary balloon dilation for stone, ampullectomy and all ERCP including attempted pancreatic stents. Eleven of 12 studies, and all with more than 30 patients have shown either trends towards reduced rates or statistically significantly lower rates of post-ERCP pancreatitis in patients receiving pancreatic stents (range 0- 20%) compared to those without pancreatic stents (range 6-67%); statistical significance was reached in three of five randomized controlled trials. [10, 14, 16]. A meta-analysis of five prospective studies involving 483 patients showed that odds ratio of post-ERCP pancreatitis without stents was three-fold higher than for with pancreatic stents (15.5% vs. 5.8%; OR: 3.2, 95% CI: 1.6 to 6.4) [21]; numbers needed-to-treat analysis showed that one in every ten patients would benefit from pancreatic duct stent placement. The major limitation of the available studies is a lack of analysis by intention-to-treat, in that patients with failed pancreatic stent placement were excluded, a group in whom pancreatitis rates have been found to be high [15].
Overall, the effectiveness of pancreatic stenting in reducing pancreatitis rates after high-risk ERCP has been corroborated by accumulating experience at advanced centers. One retrospective study using historical controls showed that in 436 patients treated with biliary ± pancreatic sphincterotomy for sphincter of Oddi dysfunction, pancreatitis rates were typically high at 28.2% (5.4% severe) in those undergoing simple pull-type biliary sphincterotomy without a pancreatic stent, compared with 13.5% (0.4% severe) in those receiving biliary ± pancreatic sphincterotomy with a pancreatic stent (P<0.05); there was a tendency for pancreatitis rates to be lower if a pancreatic stent was placed prior to pancreaticobiliary sphincterotomy (10.7%) than after (19.2%) [9].
A striking finding from all of the published studies, and from accumulating experience at advanced centers at which pancreatic stents are frequently used, is that risk of severe or necrotizing pancreatitis was virtually eliminated by a properly positioned pancreatic stent. In all reported studies, including approximately 1,500 high-risk ERCPs, over half of which involved pancreatic stents, only one case of severe pancreatitis was reported in a patient receiving a pancreatic stent [9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21]. By meta-analysis, odds of developing severe pancreatitis were found to be 11.5 times lower in patients receiving pancreatic stents [21]. Caveats of pancreatic stenting as a strategy to prevent post-ERCP pancreatitis are substantial, and have led to the inconsistent adoption of this technique, even by some experts. Most studies from expert centers have reported failure rates of 5-10% of pancreatic stent placement, especially in patients with stenotic pancreatic orifices or small and tortuous ducts, when using standard techniques involving placement of a guide wire deep into the pancreatic duct [10, 14, 17]. A recent study from our center confirmed the suspicion that failed attempted pancreatic stent placement was very risky, with twothirds of patients developing moderate or severe pancreatitis - implying that pancreatic stent placement should only be considered when it can almost certainly be followed to completion; this same study showed that universal success at pancreatic stent placement could be achieved by use of a modified technique involving a small-caliber 0.018 inch diameter guidewire and short (2 cm) small-caliber stents in patients with small or tortuous ducts [15]. Many practicing endoscopists are unfamiliar with the specific techniques required to achieve pancreatic ductal access, especially the small caliber guidewires (0.018 to 0.025 inch) that are necessary to place the small caliber (3 or 4 French) stents that appear to be safest for preventing ductal injury and prevention of pancreatitis (Figure 1). Placement of guidewires deep into the pancreatic duct may require different techniques than into the bile duct because of the tortuous course, and the potential for passage of the wire tip out any of the multiple sidebranches. Pancreatic stents can be accidentally delivered entirely into the duct, can later migrate inwards (especially longer straight stents without a duodenal pigtail, or those with two inner flanges) [22] and can cause ductal perforation, all with serious consequences.
Figure 1. 4 French pancreatic stent draining clear
pancreatic juice, placed after difficult cannulation and
biliary sphincterotomy.
Pancreatic ductal and parenchymal changes induced by pancreatic stents are a concern, but one which has been greatly reduced by use of very small-caliber stents [23, 24, 25, 26, 27]. Ductal and parenchymal changes have been observed in approximately one third to two thirds of patients, sometimes after relatively brief duration of stenting, and especially in those with previously normal pancreatic ducts. While most ductal changes resolve spontaneously, the long-term outcome has not been thoroughly investigated. Ductal changes have been observed mostly in patients having traditional flanged 5 or 7 French stents, which may be of similar caliber to the native pancreatic duct, are made of rigid polyethylene, and have large pointed inner flanges, all factors that may contribute to injury while present in the duct and during stent removal. Recent data from a large retrospective study suggest that unflanged, longer 3 French stents with a single duodenal pigtail were associated with substantially reduced frequency of ductal changes (24% for 3 and 4 French stents compared with 80% for 5 and 6 French stents), and were not observed to migrate inside the duct [23]. Three French stents were also associated with slightly lower rate of post-ERCP pancreatitis (7.5%) compared with 5 French stents (9.8% pancreatitis) or 6 French stents (14.6%). It is possible but unknown whether stents made of newer softer materials than the traditional polyethylene, and with smaller inner flanges, will also result in less duct injury.
All patients with pancreatic stents must undergo specific follow-up to ascertain spontaneous passage of the stent, or for endoscopic removal in rare cases without stent passage - these add cost and complexity to the care of the patient, but one that seems minor compared with cost and consequences of managing even the occasional case of severe post-ERCP pancreatitis. Because stentinduced pancreatic injury may be related to duration of stenting, it is necessary to either document passage of pancreatic stents by abdominal X-ray or perform endoscopic removal, preferably within 2 to 4 weeks if placed for prophylaxis. The spontaneous passage rate of small caliber (3 French, unflanged) pancreatic stents has been shown to be substantially higher than for traditional stents, with spontaneous stent passage occurring in 86% of 3 French stents versus 65 to 73% of 4 to 6 French stents (P<0.001) [23]. Nasopancreatic drains have been proposed as an alternative to pancreatic stenting, as they can be removed without a repeat endoscopic procedure [11]. These require placement of a relatively large caliber (4 or 5 French) flanged catheter to the relatively narrower duct in the body or the tail of the pancreas, raising concern for possible ductal injury. Nasopancreatic drains are sometimes poorly tolerated by patients and require overnight hospitalization, limiting their utility Overall, pancreatic stenting appears to be very promising strategy for prevention of post- ERCP pancreatitis, and has dramatically altered outcomes of high-risk ERCP at centers utilizing this technique. At our center consisting of two endoscopists who perform ERCP, approximately 300 pancreatic stents are placed annually for the purpose of preventing post-ERCP pancreatitis. As such, despite performance of mostly high-risk ERCP including treatment of sphincter of Oddi dysfunction, and complex pancreatic and biliary therapy, we have found, like other centers adopting this technique, that severe post-ERCP has been virtually eliminated - now approximately one in every 1,000 to 2,000 cases - and when it occurs, always involving either omission of pancreatic stent placement, or a very rare malfunction or duct perforation from a poorly positioned pancreatic stent. Despite use of pancreatic stents, mild pancreatitis still occurs with some frequency in high-risk patients, but is more of a nuisance than a serious complication. Like many others, we have shifted almost exclusively to very small caliber stents - either long (8-10 cm), single external pigtail, and unflanged 3 French stents placed to the midbody, or in patients with small or tortuous pancreatic ducts, we use 4 French straight flanged but short (2 cm) stents made of a softer material than conventional polyethylene (Hobbs Medical, Inc., Stafford Springs, CT, USA). Most importantly, we have found that one type or size of pancreatic stent does not suit all occasions, and that the stent must be carefully chosen to match the diameter and course of the duct. We place pancreatic stents in all higher risk situations - especially suspected sphincter of Oddi dysfunction - after difficult cannulation, before precut sphincterotomy, and after ampullectomy, among others. We have found that accessing the pancreatic duct with a guidewire, and ability to subsequently place pancreatic stents removes much of the fear and apprehension from previously daunting cases, and has allowed us to proceed with much greater confidence and achieve near-universal success at achieving biductal access with advanced techniques such as precut (access) papillotomy and treatment of sphincter of Oddi dysfunction, even under the most challenging of situations such as after gastric bypass with Roux-en-Y or previously failed cannulation [28].
While pancreatic stent placement has revolutionized the reduction of post-ERCP pancreatitis, questions still remain unanswered. It can still be difficult to decide which individual patients and procedures are at sufficiently high risk to warrant placement of pancreatic stents. Most importantly, it is unclear how well this technique will translate outside major centers. Effectiveness and safety of pancreatic stent placement by community endoscopists would be expected to be less than for advanced centers. A multicenter outcome study of pancreatic stent placement in a spectrum of practices would give us a better sense of the ultimate “effectiveness” as opposed to “efficacy” of pancreatic stenting in preventing post-ERCP pancreatitis. Ultimately, the best hope for prevention of post-ERCP pancreatitis lies in careful selection of patients for ERCP, with avoidance of unnecessary or marginally indicated cases by use of laparoscopic cholangiography during cholecystectomy, MRCP, and EUS [7]. Once ERCP is undertaken, careful technique by experienced endoscopist goes a long way, but not all the way to prevent pancreatitis. It is our opinion that pancreatic stenting does have potential to greatly impact post-ERCP pancreatitis, and that practicing endoscopists should either seek specific updated training in the equipment and techniques required for pancreatic stent insertion, or refer patients at higher risk to specialized centers with experience at pancreatic stent insertion.
References
- Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991; 37:383-93. [PMID 2070995]
- Freeman ML, Guda NM. Prevention of post-ERCP pancreatitis: a comprehensive review. Gastrointest Endosc 2004; 59:845-64. [PMID 15173799]
- Freeman ML, DiSario JA, Nelson DB, Fennerty MB, Lee JG, Bjorkman DJ, et al. Risk factors for post- ERCP pancreatitis: a prospective, multicenter study. Gastrointest Endosc 2001; 54:425-34. [PMID 11577302]
- Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med 1996; 335:909-18. [PMID 8782497]
- Loperfido S, Angelini G, Benedetti G, Chilovi F, Costan F, De Berardinis F, et al. Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. Gastrointest Endosc 1998; 48:1-10. [PMID 9684657]
- Masci E, Toti G, Mariani A, Curioni S, Lomazzi A, Dinelli M, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol 2001; 96:417-23. [PMID 11232684]
- Cohen S, Bacon BR, Berlin JA, Fleischer D, Hecht GA, Loehrer PJ Sr, et al. National Institutes of Health State-of-the-Science Conference Statement: ERCP for diagnosis and therapy, January 14-16, 2002. Gastrointest Endosc 2002; 56:803-9. [PMID 12447289]
- Masci E, Mariani A, Curioni S, Testoni PA. Risk factors for pancreatitis following endoscopic retrograde cholangiopancreatography: a meta-analysis. Endoscopy 2003; 35:830-4. [PMID 14551860]
- Fogel EL, Eversman D, Jamidar P, Sherman S, Lehman GA. Sphincter of Oddi dysfunction: pancreaticobiliary sphincterotomy with pancreatic stent placement has a lower rate of pancreatitis than biliary sphincterotomy alone. Endoscopy 2002; 34:280-5. [PMID 11932782]
- Tarnasky PR, Palesch YY, Cunningham JT, Mauldin PD, Cotton PB, Hawes RH. Pancreatic stenting prevents pancreatitis after biliary sphincterotomy in patients with sphincter of Oddi dysfunction. Gastroenterology 1998; 115:1518-24. [PMID 9834280]
- Elton E, Howell DA, Parsons WG, Qaseem T, Hanson BL. Endoscopic pancreatic sphincterotomy: indications, outcome, and a safe stentless technique. Gastrointest Endosc 1998; 47:240-9. [PMID 9540876]
- Patel R, Tarnasky P, Hennessy WS, Hawes R, Payne KM, Nelles SE, et al. Does stenting after pancreatic sphincterotomy reduce post-ERCP pancreatitis in patients with prior biliary sphincterotomy? Preliminary results of a prospective randomized trial. Gastrointest Endosc 1999; 49:AB80. (Abstract)
- Aizawa T, Ueno N. Stent placement in the pancreatic duct prevents pancreatitis after endoscopic sphincter dilation for removal of bile duct stones. Gastrointest Endosc 2001; 54:209-13. [PMID 11474392]
- Fazel A, Quadri A, Catalano MF, Meyerson SM, Geenen JE. Does a pancreatic duct stent prevent post- ERCP pancreatitis? A prospective randomized study. Gastrointest Endosc 2003; 57:291-4. [PMID 12612504]
- Freeman ML, Overby C, Qi D. Pancreatic stent insertion: consequences of failure and results of a modified technique to maximize success. Gastrointest Endosc 2004; 59:8-14. [PMID 14722540]
- Sherman S, Earle DT, Bucksot L, Baute P, Gottlieb K, Lehman G. Does leaving a main pancreatic duct stent in place reduce the incidence of precut biliary sphincterotomy (ES)-induced pancreatitis? A final analysis of a randomized prospective study. Gastrointest Endosc 1996; 43:A489. (Abstract)
- Smithline A, Silverman W, Rogers D, Nisi R, Wiersema M, Jamidar P, et al. Effect of prophylactic main pancreatic duct stenting on the incidence of biliary endoscopic sphincterotomy-induced pancreatitis in high-risk patients. Gastrointest Endosc 1993; 39:652-7. [PMID 8224687]
- Vandervoort J, Soetikno RM, Montes H, Lichtenstein DR, Van Dam J, Ruymann FW, et al. Accuracy and complication rate of brush cytology from bile duct versus pancreatic duct. Gastrointest Endosc 1999; 49:322-7. [PMID 10049415]
- Norton ID, Gostout CJ, Baron TH, Geller A, Petersen BT, Wiersema MJ. Safety and outcome of endoscopic snare excision of the major duodenal papilla. Gastrointest Endosc 2002; 56:239-43. [PMID 12145603]
- Catalano MF, Linder JD, Chak A, Sivak MV, Raijman I, Geenen JE, et al. Endoscopic management of adenoma of the major duodenal papilla. Gastrointest Endosc 2004; 59:225-32. [PMID 14745396]
- Singh P, Sivak MV, Agarwal D, Wong R, Isenberg G, Das A, et al. Prophylactic pancreatic stenting for prevention of of Post-ERCP acute pancreatitis: a metaanalysis of controlled trials. Gastrointest Endosc 2003: 57:AB89. (Abstract)
- Johanson JF, Schmalz MJ, Geenen JE. Incidence and risk factors for biliary and pancreatic stent migration. Gastrointest Endosc 1992; 38:341-6. [PMID 1607087]
- Rashdan A, Fogel EL, McHenry L Jr, Sherman S, Temkit M, Lehman GA. Improved stent characteristics for prophylaxis of post-ERCP pancreatitis. Clin Gastroenterol Hepatol 2004; 2 322-9. [PMID 15067627]
- Kozarek RA. Pancreatic stents can induce ductal changes consistent with chronic pancreatitis. Gastrointest Endosc 1990; 36:93-5. [PMID 2335298]
- Sherman S, Hawes RH, Savides TJ, Gress FG, Ikenberry SO, Smith MT, et al. Stent-induced pancreatic ductal and parenchymal changes: correlation of endoscopic ultrasound with ERCP. Gastrointest Endosc 1996; 44:276-82. [PMID 8885346]
- Siegel J, Veerappan A. Endoscopic management of pancreatic disorders: potential risks of pancreatic prostheses. Endoscopy 1991; 23:177-80. [PMID 1860449]
- Smith MT, Sherman S, Ikenberry SO, Hawes RH, Lehman GA. Alterations in pancreatic ductal morphology following polyethylene pancreatic stent therapy. Gastrointest Endosc 1996; 44:268-75. [PMID 8885345]
- Freeman ML. Precut (access) sphincterotomy. Tech Gastrointest Endosc 1999; 1:40-8.


