Keywords
pancreas; Length of Stay; Pancreatectomy; Pancreatic
Fistula; surgery
Abrreviations
EUS endoscopic ultrasonography; FNAC fine needle
aspiration cytology; RACP robot-assisted central pancreatectomy
INTRODUCTION
This case report describes our technique in performing
a robot-assisted central pancreatectomy (RACP). The
operation was employed to manage a solid pseudopapillary
neoplasm of the neck of the pancreas discovered during a
routine staging for breast cancer. The setting was a busy
dedicated third-level Hepato-biliary-pancreatic Center
with great experience in both pancreatic and robotic
surgery.
PATIENT INFORMATION
The patient was a Caucasian 49-years-old
woman. Medical history was unremarkable.
No cancerous clustering present in the family tree.
Nevertheless, a breast cancer was diagnosed during
screening mammography with a Core Needle Biopsy-B5.
Staging Thorax -Abdominal CT found out an incidental
pancreatic lesion, measuring 5 centimeters in the
maximum diameter, arising from the neck/body of the
pancreas (Figure 1). An endoscopic ultrasonography
(EUS) confirmed a hypoechoic lesion with inhomogeneous
core, leading to the suspicious of a a benign to borderline
pancreatic neoplasm. No lymphadenopathy was detected.
A fine needle aspiration cytology (FNAC) was resulted for
a solid pseudo-papillary neoplasia (SPN).
Figure 1. Preoperative Abdominal CT , demonstrating a lesion measuring 5 centimeters in the maximum diameter, arising from the neck/body of the
pancreas.
The cancer multidisciplinary team meeting
recommended to perform neoadjuvant chemotherapy
and breast conserving surgery as the first step. Twelve
weeks after breast surgery, the patient was referred to
our Centre to treat the pancreatic neoplasm. Decision to
perform a RACP was undertaken secondary to the low
aggressive histology, small dimension and position of the
pancreatic neoplasm, close to the neck/body of the gland .
The young age of the patient and the good life expectancy
after surgery, concurred also in the decision making
process. In fact young and fit patients are those supposed
could benefit of the advantages of a minimally invasive and
parenchyma sparing approach.
THERAPEUTIC INTERVENTION
Technique
The procedure was performed with the robotic System
Da Vinci Xi® . Patient was placed in supine position with
inferior limbs abducted and moved to a 15-20° reverse
Trendelenburg. A nasogastric tube was placed to allow
gastric decompression. The pneumoperitoneum was
inducted up to 12 mmHg through a Verres needle. Robotic
cart was docked from patient’s head, taking attention that
the main axis of the cart was coinciding with the principal
working axis, coming from the opposite site.
Six trocar ports were employed. In details, an 8-mm
camera port was placed approximately 2–3 cm above and
to the right of the umbilicus. Other three robotic 8-mm
ports were placed to the left (R1) and to the right (R2
and R3) side laterally from the umbilicus. Two additional
laparoscopic ports were placed approximately 4–5 cm
below the camera port along the left (12 mm port) and
the right (5 mm port) mid-clavicular lines respectively, for
assistance and retraction (Figure 2).
Figure 2. Operating theatre layout for robotic central pancreatectomy. This image displays the surgeonÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s position and the trocar sites for the procedure.
We used monopolar scissors, bipolar Maryland forceps,
fenestrated forceps as retractor and ultrasonic scalpel
where indicated. We employed also a robotic ultrasound transducer probe, with fingertip control, to enable real-time
image guidance during the dissection and increase accuracy.
The operation begun with the dissection of the
gastrocolic ligament, allowing the lesser sac to be opened,
and the pancreas exposed. The anterior surface of the
portal vein (PV) was dissected at the superior edge of the
pancreatic body and the superior mesenteric vein (SMI)
was exposed at the inferior edge of the pancreatic neck.
Splenic artery and vein (SA, SV) were then identified and
the Toldt fascia incised along the superior and inferior
margin of the pancreas.
The endo-ultrasound probe (EUS) confirmed
the presence of a 5 cm lesion adjacent to the main
pancreatic duct and to the splenic vessels. Stitches of 4-0
polypropylene were placed at the inferior and superior
pancreatic borders to allow a better mobilization and to
ligate transverse pancreatic arteries.
The retropancreatic tunnel was carefully created with
gentle dissection.
Progressive dissection of the proximal stump was
achieved with the robotic ultrasonic scalpel. The main pancreatic duct was identified and selectively tied using
stitches of 4-0 polypropylene. With the endo-ultrasound
probe the diameter of the Wirsung duct was measured 1.7
mm. Small branches of the inferior mesenteric vein (IMV)
to and from the pancreas were ligated between plastic
and a metallic clip to assure proper haemostasis. The
transection of the pancreatic neck was then completed,
and a sealing patch was placed on the stump.
After sonographic identification of the margins of the
lesion, the dissection of the distal pancreatic stump was
performed with robotic ultrasonic scalpel, preserving the
main pancreatic duct.
For the reconstructive phase we used a jejunal loop
dissected 30 cm distally from the Treitz ligament to perform
an end-to-side, duct-to-mucosa, pancreatic-jejunum
anastomosis in two layers of interrupted stitches.
6 interrupted 4-0 non absorbable coated braided
polyester stitches were affixed between the pancreatic
parenchyma and the serous layer of the jejunal loop to
build up the posterior wall of the pancreatic-jejunum
anastomosis.
A duct to mucosa anastomosis was then performed
between main pancreatic duct and the jejunum enterotomy
using 5-0 polydioxanone stitches. A duct stent was used to
facilitate the suture.The anterior layer of the anastomosis
was completed with stitches of 4-0 non absorbable coated
braided polyester.
The end-to-side jejuno-jejunostomy (Roux-en-Y)
completed the distal reconstruction. Pancreatic perianastomotic
drainage suction was left in situ (Figure 3).
Figure 3. Intraoperative images. (a). Identification of the lesion and execution of intraoperative ecography. (b). Proximal stump dissection. (c).
Identification of distal main pancreatic duct during distal stump dissection. (d). Pancretico-jejunoanastomosis
FOLLOW-UP AND OUTCOMES
Operative time was 345 minutes, with an estimated
blood loss of 100 ml. No Intensive Care Recovery (ICU)
observation was indicated after surgery. Postoperative
course was uneventful, except for a mild fever managed
empirically by oral antibiotics. On postoperative day (POD)
1 bladder catheter was removed and the patient allowed to
mobilize. Pulmonary work was incentivated with specific
exercises. Amylase collected from the drain fluid were 174
U/L.
Semi-liquid diet was introduced. A routine CT-scan
revealed a small (3 cm) peripancreatic collection,
managed conservatively (Figure 4). On POD 5 blood
check was normal. Amylases in the drain fluid were
50 U/L and the drain was removed. The patient was
discharged on POD 8 with oral antibiotic therapy
prescribed (levofloxacine 500 mg mid), pancreatic
enzyme replacement (pancrealipase 25.000 UI during
lunch) and deep venous thrombosis prophylaxis (low
weight molecular heparin).
Figure 4. Post-operatory abdominal CT, demonstrating a limited peripancreatic fluid collection.
DISCUSSION
Conventional pancreatic resections may be an
overtreatment for patient with small tumors of benign or
low malignant potential, located close to the neck and the
body of the gland, and long term survival expected after
surgery. Together with risk of postoperative pancreatic
fistula (POPF), both exocrine and endocrine impairment
should be considered [1]. Therefore a careful balance
between oncological radicality and postoperative quality
of life is mandatory.
Central pancreatectomy (CP) could be a rational and
feasible surgical option to treat patients that meet the
selected criteria.
Young patients, with low aggressive, small (<5 cm)
lesions, located between the neck and the pancreatic body
or chronic focal pancreatitis [2] are the best candidates
to CP. The specific technical contraindications for simple
enucleation (lesions lying close to main pancreatic duct at
risk of major damage) are also good indications for central
pancreatectomy [2].
Although this procedure is associated with an higher
risk of postoperative fistula1 arising from the proximal
stump or the distal anastomosis, on the other hands, the
preservation of pancreatic tissue, may reduce the risk
of endocrine and exocrine postoperative impairment.
Moreover, the CP is often associated with the preservation
of the spleen as well as the biliary and upper digestive
tracts [3].
The first open CP with pancreato-enterostomy
reconstruction was reported in 1982 by Degradi and Serio
[4]. Initial experiences were earlier reported to manage
limited chronic pancreatitis or traumatic rupture of the
gland, with or without formal reconstructions.
A literature research in PubMed database (1992-
2015) about open central pancreatectomy outlines 24
articles, with a total of 1095 patients who underwent
this procedure [5]. Incidence of POPF was rated from 0 to
65%, higher if compared to the more common pancreatic
procedures (Pancreaoto-duodenectomy-PD 0-20%, Distal
pancreatectomy- DP 2-32%). Endocrine insufficiency was
reported from 0% to 14% and exocrine insufficiency from
0% to 22%. The postoperative 30-days mortality was 3%,
similar that achieved by PD and DP.
Baca and Bokan [6] described the first laparoscopic CP
(LCP) in 2003. Since then, with the increasing diffusion
of the minimally invasive techniques a total of 18 articles
regarding LCP were published (comprehensive of 91
patients) [7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20,
21, 22, 23, 24, 25]. Post-operative fistula was reported in
24 patients (26%) with only 2 patients (2.2%) requiring
consultations for postoperative exocrine impairment.
Literature search reported experiences of LCP with
reconstruction of the digestive tract both with pancreatogastro
(PG) and pancreato-jejunal (PJ) anastomosis.
Actually the study with the major number of LCP (n=51)
available was published by Machado [23]. This experience
reported 63% of PG and 35% of PJ anastomosis performed
with a POPF rate of 46%. The study did not compared
the incidence of pancreatic fistula between the PG and PJ
anastomosis group.
The few available comparative papers between
laparoscopic and open central pancreatectomy for low
aggressive lesions demonstrated longer operative times,
no differences in blood loss, a faster refeeding and shorter
hospital stay for the laparoscopic group respect to the
open group [25]. A randomized control trial published
by Song et al. [21], comparing 26 cases of LCP versus 14
cases OCP all equally performed with PJ reconstruction,
reported a POPF rate of 19,2% (n=5, grade B or C) against a
rate of 35,7% (n=5, grade B or C) in the OCP group. Fistula
outcomes are better in the laparoscopic group, but not
statistically significant (p=0.25).
Beyond any doubt pancreatic anastomosis with PG or
PJ reconstruction remains the most difficult step during
LCP, with a POPF rate that remains similar to that of OCP.
Different anastomotic techniques were also proposed to
decrease the risk of POPF in LCP. Jiao et al. [15] reported
an initial experience in 4 patients with a technique
named laparoscopic long sleeve pancreato-gastrectomy
(LPG) with only one POPF grade A occurred. A new
reconstruction technique was also proposed by Francone et al. [26] utilizing the same jejunum loop to perform the
proximal and distal anastomosis.
In 2004, Giulianotti performed the first robotic
assisted CP (RACP), just a year later the first laparoscopic
procedure.
The robot assisted pancreatic surgery was gradually
implemented over the years. Theoretically, it could merge
all the advantages of minimally invasive laparoscopic
approach with the implementation of the robotic
technology. The magnified, steady, 3D-high definition
imaging and the integrated ultrasonography system
allow to the surgeon a precise anatomical localization of
the lesion and of the vascular structures. In addition, the
seven degrees instruments replicating the human hand
movements, overcome many of the gaps encountered
with traditional laparoscopy in challenging pancreatic
resections. Vascular dissection, suturing and
reconstructions are manageable and safe to perform
with the robotics instruments with a learning curve
comparable to that of open surgery [27, 28].
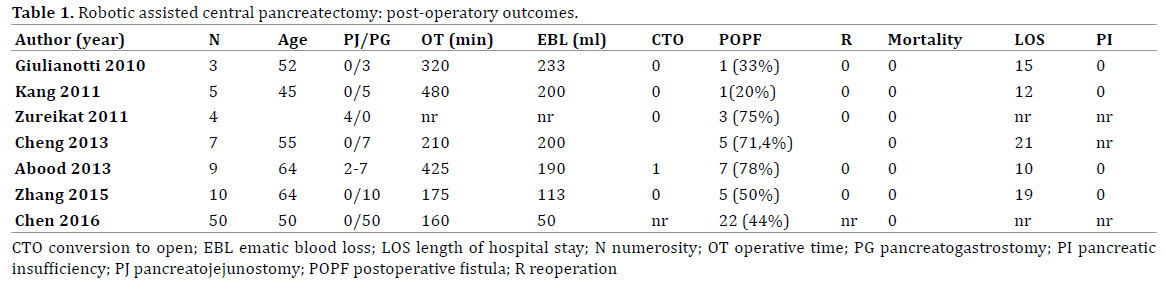
Successively Giulianotti’s [29] experience, only seven
papers regarding RACP were published [30, 31, 32, 33,
34, 35] with a total of 88 central robotic procedures
performed to the present days. In most of the robotic
procedures, reconstruction was preferentially performed
through a pancreatico-gastric anastomosis (PG, 82/88) with
a total POPF rate of 48%. In the few PJ group [30, 31] (6/88),
the POPF was reported only in three out of six cases (50%).
Between this group 4 cases were specifically reconstructed
with a modified Blumgart anastomosis [36, 37].
No study is actually available in literature comparing
different reconstruction techniques used in OCP or
LCP and RACP in term of POPF rate. Therefore the risk
of POPF depending on the reconstruction technique
cannot yet be assessed for none of these procedures. It
is anyway stimulant reflecting on the fact that a recent
Cochrane systematic review [38] highlighted little or no
difference between PJ and PG reconstruction technique
in overall risk of postoperative pancreatic fistula in
pancreaticoduodenectomy (PJ 24.3%; PG 21.4%; RR 1.19,
95% CI 0.88 to 1.62; 7 studies; low-quality evidence).
The choice to perform a PJ over a PG anastomosis as
reconstruction strategy in the case above presented was
mostly related to the fact that as pancreatic dedicated
surgical department our personal experience in regards to
PG anastomosis was slightly negative, with a major number
or bleeding events occurred and technical difficulties
encountered in the management of anastomotic leak and
bleeding in the case surgery was required a second time.
A randomized controlled trial edited in 2016 [36]
confronted 50 cases of OCP with 50 cases of RACP. Formal
reconstruction was performed with a PG anastomosis. The
comparison of POPF rate between the two groups was not
statistically significant with a POPF rate of 54% (n=27)
in the OCP group and of 44% (n=22) in the RACP group.
In detail grade A fistula occurred in major number in the
RACP group (82% vs. 64%), while grade B/C fistula were
more frequent in the OCP group (36% vs. 18%).
Unfortunately none of the published papers, confronted
LCP and RACP in terms of postoperative outcomes and
POPF risk. Nevertheless it is well accepted that complex
technical steps of pancreatic resections, mostly in the
reconstruction phase, are best managed with robotic than
traditional laparoscopy (Table 1).
CONCLUSION
Central Pancreatectomy is still an high risk and
technically challenging procedure, potentially aggravated
by perioperative complications. Accurate selection of
the patients that meet the correct surgical criteria and
careful balance of the risk of POPF with the advantages of
parenchyma preservation is recommended. The robotic
approach whenever indicated is feasible and effective and
permits a better management of the reconstructive steps
compared to traditional laparoscopy. The perioperative
parameters, including blood loss, hospital stay, recovery,
infections are optimized. The operative time is longer
in most of the experiences, although reduced with the
progression in the learning curve. However, a standardized
procedure for RACP is not actually defined, and the better
technique of robotic reconstruction not demonstrated yet.
More rigorous clinical research should be advocated for
the future.
Conflict of Interest
The authors declare that they have no conflicts of interest.
References
- Iacono C, Verlato G, Ruzzenente A, Campagnaro T, Bacchelli C,
Valdegamberi A. et al. Systematic review of central pancreatectomy and
meta-analysis of central versus distal pancreatectomy. Brit J Surg 2013;
100:873–885. [PMID: 23640664]
- Iacono C, Bortolasi L, Facci E, Nifosi F, Pachera S, Ruzzenente A,
et al. The Dagradi-Serio-Iacono operation central pancreatectomy. J
Gastrointest Surg 2007; 11:364–76. [PMID: 17458612]
- Iacono C, Bortolasi L, Serio G. Is there a place for central
pancreatectomy in pancreatic surgery? J Gastrointest Surg 1998; 2:509-
516. [PMID: 10457309]
- Dagradi A, Serio G. Enciclopedia Medica Italiana. Pancreatectomia
intermedia. In: Vol XI: pancreas. Firenze: USES Edizioni Scientifiche 1984;
850-51.
- Santangelo M, Esposito A, Tammaro V, Calogero A, Criscitiello C,
Roberti G, et al. What indication, morbidity and mortality for central
pancreatectomy in oncological surgery? A systematic review. Int J Surg
2016; 28-1:S172-6. [PMID: 26708862]
- Baca I, Bokan I. Laparoscopic segmental pancreas resection and
pancreatic cystadenoma, Chirurg 2003; 74:961-965. [PMID: 14605740]
- Sa CA, Rault A, Beau C, Masson B. Laparoscopic central
pancreatectomy: single institution experience of 6 patients. Surgery
2007; 142:405–409. [PMID: 17723894]
- Ayav A, Bresler L, Brunaud L. Laparoscopic approach for solitary
insulinoma: a multicentre study. Langenbeck Arch Surg 2005; 390:134–
140. [PMID: 15609056]
- Orsenigo E, Baccari P, Bissolotti G, Staudacher C. Laparoscopic central
pancreatectomy. Am J Surg 2006; 191:549–552. [PMID: 16531153]
- Sucandy I, Pfeifer CC, Sheldon DG. Laparoscopic assisted central
pancreatectomy with pancreaticogastrostomy reconstruction—an
alternative surgical technique for central pancreatic mass resection. N
Am J Med Sci 2010; 2:438–441. [PMID:22558594]
- Gumbs AA, Rodriguez-Rivera AM, Hoffman JP. Minimally invasive
pancreatic surgery of the entire gland: initial experience. Minerva Chir
2011; 66:269–280 [PMID:21873961]
- Gonzalez F, Mesleh MG, Lukens FJ, Wallace MB, Asbun HJ, Stauffer JA.
Laparoscopic central pancreatectomy and pancreaticogastrostomy for
the management of a proximally migrated pancreatic stent. JOP 2013;
14:273–276. [PMID: 23669478]
- Gumbs AA, Rodriguez Rivera AM, Milone L, Hoffmann JP. Laparoscopic
pancreatoduodenectomy: a review of 285 published cases. Ann Surg
Oncol 2011; 18:1335–1341. [PMID: 21207166]
- Cienfuegos JA, Salguero J, Núñez-Córdoba JM, Ruiz-Canela M, Benito
A, Ocaña S, et al. Short and long-term outcomes of laparoscopic organsparing
resection in pancreatic neuroendocrine tumors: a single-center
experience. Surg Endosc 2017; 31:3847-3857 [PMID:28127714]
- Jiao LR, Gall TMH, Sodergren MH, Fan R. Laparoscopic long sleeve
pancreaticogastrostomy (LPG): a novel pancreatic anastomosis following
central pancreatectomy. Hepatobiliary Surg Nutr 2016; 5:245–248
[PMID:4876250]
- Francone E, Berti S, Celoria GM, Bianchi C, Magistrelli P, D'Ambra
L, et al. Double pancreaticojejunostomy in pure laparoscopic central
pancreatectomy: an uncommon reconstructive strategy. Minerva Chir
2016; 71:156-8 [PMID: 27096469]
- Schwarz L, Katz MHG. Diagnosis and Management of Borderline
Resectable Pancreatic Adenocarcinoma. Hematol Oncol Clin North Am
2015; 29:727-740 [PMID: 26226907]
- Senthilnatha P, Gul SI, Gurumurthy SS, Palanivelu PR, Parthasarathi
R, Palanisamy NV, et al. Laparoscopic central pancreatectomy: Our
technique and long-term results in 14 patients. J Minim Access Surg 2015;
11:167–171. [PMID:26195873]
- Jiang CY, Wang W. Initial Experience in Total Laparoscopic Central
Pancreatectomy with Pancreatogastrostomy. Cell Biochem Biophys
2015; 71:1023. [PMID: 25355079]
- Chen, XM, Zhang Y, Sun DL. Laparoscopic central pancreatectomy for
solid pseudopapillary tumors of the pancreas: our experience with ten
cases. World J Surg Oncol 2014; 12:312. [PMID: 25307540]
- Song KB, Kim SC, Park KM, Hwang DW, Lee JH, Lee DJ, et al.
Laparoscopic Central Pancreatectomy for Benign or Low-Grade Malignant
Lesions in the Pancreatic Neck and Proximal Body. Surg Endosc 2014;
29:937-946. [PMID: 25149632]
- Zhang R, Xu X, Yan J, Wu D, Ajoodhea H, Mou YJ. Laparoscopic central
pancreatectomy with pancreaticojejunostomy: preliminary experience with
8 cases. Laparoendosc Adv Surg Tech A 2013; 23:912-8. [PMID: 24093934]
- Machado MAC, Surjan RC, Epstein MG, Makdissi FF. Laparoscopic
Central Pancreatectomy: A Review of 51 Cases. Surg Laparosc Endosc
Percutan Tech 2013; 23:486–490. [PMID: 24300922]
- Senthilnathan, Gul P, Gurumurthy SI, Palanivelu SS, Parthasarathi PR,
Palanisamy R. Laparoscopic central pancreatectomy: Our technique and
long-term results in 14 patients. J Minim Access Surg 2015; 11:167–171.
[PMID: 26195873]
- Kang MK, Kim SC, Song KB, Park KM, Lee JH, Hwang JW, et al.
Laparoscopic versus Open Central Pancreatectomy: Single-institution
Comparative Study. J Minim Invasive Surg 2012; 15:83-92.
- Francone E, Berti F, Celoria GM. Double pancreaticojejunostomy in
pure laparoscopic central pancreatectomy: an uncommon reconstructive
strategy. Minerva Chirurgica 2016; 71:156-8. [PMID: 27096469]
- Stafford AT, Walsh RM. Robotic surgery of the pancreas: The current
state of the art. J Surg Oncology 2015; 112: 289–294. [PMID: 26220683]
- Boone BA, Zenati M, Hogg ME, Steve J, Moser AJ, Bartlett DL, et al.
Assessment of Quality Outcomes for Robotic Pancreaticoduodenectomy:
identification of the Learning Curve. JAMA Surg 2015; 150:416-422.
[PMID: 25761143]
- Giulianotti PC, Sbrana F, Bianco FM, Addeo P, Caravaglios G. Robotassisted
laparoscopic middle pancreatectomy. J Laparoendosc Adv Surg
Tech 2010; 20:135-139. [PMID: 20201684]
- Kang CM, Kim DH, Lee WJ, Chi HS. Initial experiences using robotassisted
central pancreatectomy with pancreaticogastrostomy: a
potential way to advanced laparoscopic pancreatectomy. Surg Endosc
2011; 25:1101–1106. [PMID: 20835724]
- Zureikat AH, Nguyen KT, Bartlett DL, Zeh HJ, Moser AJ. Robotic-
Assisted Major Pancreatic Resection and Reconstruction. Arch Surg 2011;
146:256-261. [PMID: 21079111]
- Cheng K, Shen B, Peng C, Deng X, Hu S. Initial experiences in
robot-assisted middle pancreatectomy. HPB 2013; 15:315–321.
[PMID:23461633]
- Abood GJ, Can MF, Daouadi M, Huss HT, Steve JY, Ramalingam L, et al.
Robotic-Assisted Minimally Invasive Central Pancreatectomy: Technique
and Outcomes. J Gastroint Surg 2013; 17:1002–1008. [PMID: 23325340]
- Zhang T, Wang X, Huo Z, Wen C, Wu Z, Zhan Q. Robot-Assisted Middle
Pancreatectomy for Elderly Patients: Our Initial Experience. International
Med J of Exp and Clin Res 2015; 21:2851–2860. [PMID: 26395335]
- Chen S, Zhan Q, Jin JB, Wu ZC, Shi Y, Cheng DF, et al. Robot-assisted
laparoscopic versus open middle pancreatectomy: short-term results of a
randomized controlled trial. Surg Endosc 2016; 31:962-971. [PMID: 27402095]
- Crippa S, Cirocchi R, Randolph R, Partelli S, Belfiori S, Piccioli A, et al.
Pancreaticojejunostomy is comparable to pancreaticogastrostomy after
pancreaticoduodenectomy: an updated meta-analysis of randomized
controlled trials. Langenbecks Arch Surg 2016; 401:427-437.
[PMID 27102322]
- Grobmyer SR, Kooby D, Blumgart LH, Hochwald SN. Novel
pancreaticojejunostomy with a low rate of anastomotic failure-related
complications. J Am Coll Surg 2010; 210:54-59. [PMID: 20123332]
- Cheng Y, Briarava M, Lai M, Wang X, Tu B, Cheng N, et al.
Pancreaticojejunostomy versus pancreaticogastrostomy reconstruction
for the prevention of postoperative pancreatic fistula following
pancreaticoduodenectomy. Cochrane Database Syst Rev 2017;
9:CD012257. [PMID: 28898386]





