Keywords
Tuberculosis; Anti-tuberculosis treatment; Treatment success; Continuation phase; Rifampicinisoniazide; Ethambutol-isoniazide
Introduction
Tuberculosis (TB) remains a major global health problem. It causes ill-health among millions of people each year and ranks in the top ten leading causes of mortality. About a third of the world’s population is estimated to be infected with TB bacilli and hence at risk of developing active disease. The latest estimates indicate almost 9 million new cases and 12 million prevalent cases of TB globally, of which 1.1 million (13%) were among people living with HIV in 2013, and 1.5 million TB deaths (360 000 were HIV-associated). About 26% of the incident TB cases occurred in Africa. The proportion of TB cases co-infected with HIV is highest in African country; overall, the African region accounted for 79% of TB cases among people living with HIV [1].
Ethiopia is one of the 22 High Burden Countries (HBCs) that have been given highest priority at the global level since 2000 and HBCs accounted for 80% of all estimated cases worldwide.
According to the 2014 quarterly health bulletin of the Federal Ministry of Health (FMOH), tuberculosis was in the top ten causes of in-hospital deaths in Ethiopia [2,3].
For effective TB control program it is very important to detect the disease as early as possible and put patients on treatment and take those to completion in order to get cure [4]. According to the WHO, treatment outcome is an important indicator to monitor the TB prevention and control program [5]. A number of factors may affect treatment outcomes.The efficacy of treatment regimens is assumed to be the same but Refampicin-based continuation phase regimens are preferred for various reasons including low treatment failure and relapse rate, higher cure rate, and shorter duration of treatment [6].
Since 2009, Ethiopia, in complaince with the global recommendations has changed the continuation phased regimen from Ethambutol-Isonized (EH) to Refampicin-Isoniazid (RH [6]. However, no study has compared treatment outcomes among patients treated with the two regimens after the change in treatment regimen. In addition, data source for a good number of studies that evaluated treatment outcome in Ethiopia were routine facility reports which might have low quality [7-12]. Therefore, in this study, we assessed treatment success rates and its predictors using the unit TB register as data source and included continuation phase treatment regimen as one of the independent variables in the analysis.
Methods
Study setting
We conducted this study in Gamo Gofa zone is one of the 15 administrative zones of Southern Nations Nationalities and Peoples (SNNP) region in Ethiopia. Administratively, it is subdivided in to 15 woreda or district and two town administrations. The total population of the zone was 1,793,255 in 2011 which account for 10.7% of the regional population. Based on the high TB case load, we selected Arba Minch general hospital, Arba Minch health center, Sawla hospital, Sawla health center and Chencha Hospital for this study. In 1992 a standardized TB prevention and control programme, incorporating Directly Observed Treatment, Short Course (DOTS), was started in the country as a pilot, at Arsi zone in Oromia. According to the Ministry of Health 2011 report, the DOTS geographic coverage reaches 100%, whereas hospital and health centre coverage is 92% and 95%, respectively. TB treatment regimen change in the continuation phase from Ethambutol Isoniazid (EH) to Rifampicin Isoniazid (RH) has been already started on Sep 11, 2009. This change reduced TB treatment period from 8 month to 6 month.
Study design
A register based, four year retrospective cross sectional study of TB patients under DOTS in Gamo Gofa Zone was carried out from October 2013 to May 2014.
Study population
We included all TB Patients who took anti TB as new treatment category for more than one month in the selected facilities and in the time period between June 2009 and July 2013. We excluded those TB patients who were diagnosed and started TB treatment in the selected facilities but transferred out to other facilities for continuation of treatment, retreatment cases (relapse, treatment after failure, or return after lost to follow-up) and TB Patients who had incomplete documentation on important variable such as Age, Sex and outcome variable.
Data management and analysis
We used data abstraction tool to collect the age, sex, address, type of TB, HIV status, continuation phase anti-TB treatment regimen, and treatment success (either cure or treatment completion). Data collection was supervised and 5% of random sample of records were rechecked for completeness and accuracy against registration books. The data was entered into SPSS version 20 and cleaned for further analysis. Predictors of treatment success were analyzed using logistic regression. All variables significant at 0.25 levels on the binary logistic analysis were included in to multi variable logistic regression model.
After model selection Hosmer and Lemeshow Goodness of fit test was carried out. P value of less than 5% was considered statistically significant.
Operational definition
Treatment outcome defined as treatment success if patient who was cured or who completed treatment whereas unsuccessful treatment is a patient, whose treatment was interrupted, failed on treatment or died [6].
Ethical consideration
The study protocol was reviewed and approved by Addis Continental Institute of Public Health and Arba Minch University Institutional Review Board, and permission was also obtained from the study facilities. Consent was not required as patients were not contacted. In addition, any identifier data was removed from the final dataset after completion of data collection.
Results
Demographic and clinical characteristics of study participants
Among 2,019 TB patients registered for treatment in the selected health facilities between July 2009 and June 2013, treatment outcome was evaluated for 1,667 (82.6%) patients. From all patient 87 (4.3%) were excluded because they were retreatment cases (relapse, treatment after failure, or return after lost to follow-up). Additional 265 patients were excluded because they were transferred-out to other facilities and their treatment outcome was not known. Of the final study sample 1,052 (63.1%) were male. The median age of the study participants was 26 years. From all considered patient for analysis 540 (32.4 %) were smear pulmonary positive cases, 888 (53.3%) were smear pulmonary negative TB cases and 239 (14.3%) were extra-pulmonary TB patients. The majority of the patients 1,454 (87.2 %) were between ages 15 and 64 years. About 56 % (n=927) of the patients were urban residents. HIV status for 1,603 (96.2%) patients was known and 14.2% (n=237) of them were HIV positive.
Tuberculosis treatment outcome
Fifty seven percent (n=951) of the patients took Rifampicin-Isoniazid (RH) during continuation phase of anti-tuberculosis treatment as shown in and 43 % were on EH (Table 1).
| Variable |
Subcategory |
Frequency (n) |
Percentage (%) |
| Age in years |
<15 |
149 |
8.94 |
| |
15-39 |
1,112 |
66.71 |
| |
40-64 |
342 |
20.52 |
| |
>64 |
64 |
3.84 |
| Gender |
Male |
1,052 |
63.11 |
| |
Female |
615 |
36.89 |
| Address |
Urban |
927 |
55.61 |
| |
Rural |
740 |
44.39 |
| HIV status |
Negative |
1,366 |
81.94 |
| |
Positive |
237 |
14.22 |
| |
Unknown |
64 |
3.84 |
| Type of Tuberculosis |
Smear positive pulmonary |
540 |
32.39 |
| |
Smear negative pulmonary |
888 |
53.27 |
| |
Extra pulmonary |
239 |
14.34 |
| Continuation phase treatment regimen |
Rifampicin-Isoniazid |
951 |
57.05 |
| |
Ethambutol-Isoniazid |
716 |
42.95 |
| Treatment center |
Arba Minch Hospital |
603 |
36.17 |
| |
Arba Minch HC |
254 |
15.24 |
| |
Sawla Hospital |
182 |
10.92 |
| |
Sawla HC |
65 |
3.9 |
| |
Chencha Hospital |
563 |
33.77 |
Table 1: Baseline characteristics of study sample for TB patients in selected facilities in Gamo Gofa Zone, Ethiopia, 2014.
Of the smear positive TB patients, sputum smear microscopy was done for 455 (84.3%) at the end of the second month of treatment and 22 (4.1%) were documented to have smear positive microscopy findings at that stage. but only, 2 (0.2%) were still smear positive at the end of the treatment, which indicates failure to respond to the first line anti TB drugs.
As for treatment outcome, 1,004 (60.2%) completed treatment out of which 440 patients were cured (26.4%) this adds up to a total of 1,444 (86.6%) patients with treatment success or favorable treatment outcome. Of the remaining patients 55 (3.3%) had died, 2 (0.1%) had treatment failure and 166(10%) were lost to follow-up as shown in Figure 1..
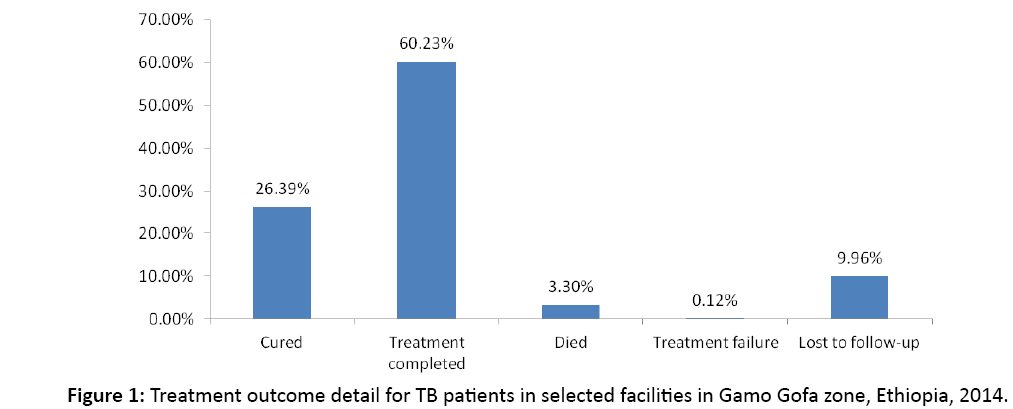
Figure 1: Treatment outcome detail for TB patients in selected facilities in Gamo Gofa zone, Ethiopia, 2014.
There is a trend of increasing treatment success from year 2009/10 to 2012/13 as shown in Figure 2 reaching 90% in the final follow-up interval. Proportion of patients who were lost to follow-up from treatment steadily dropped from 14.6% to 6.2% over the study period. The proportion of TB patients with unknown HIV status also showed a reduction from 7.4% in 2009/10 to 2.2 % in 2012/13. Although treatment success of 86.3% was high overall in the study there were variations across treatment centers from as low as 80.1% in Chencha hospital to as high as 91.7% in Arba Minch health center (p<0.001).
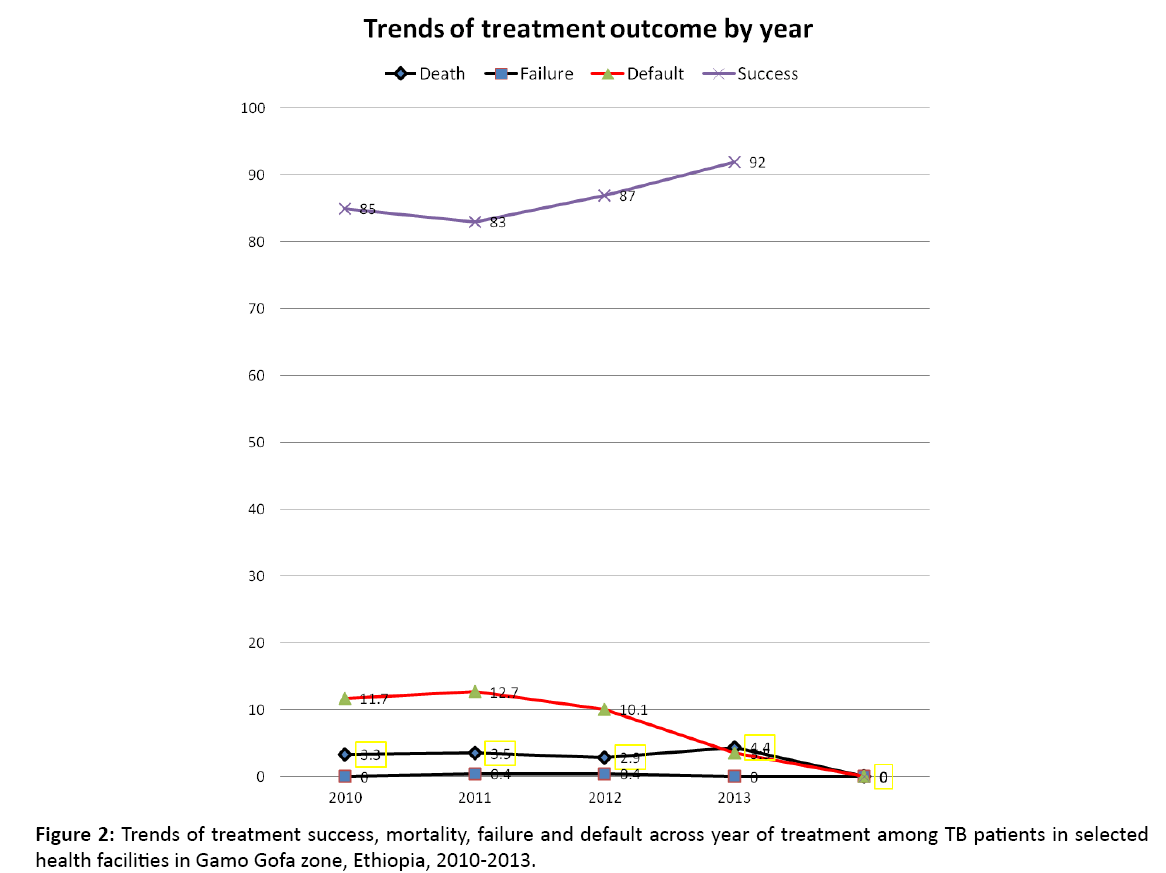
Figure 2: Trends of treatment success, mortality, failure and default across year of treatment among TB patients in selected health facilities in Gamo Gofa zone, Ethiopia, 2010-2013.
Factors affecting treatment success
Result from multivariable logistic regression analysis reveals that place of residence, type of TB, anti-TB regimen during continuation phase, and HIV status were found to be significantly associated with treatment success. Patients from rural areas had significantly lower treatment success [AOR=0.62 (95% CI 0.46-0.83)] than those from urban areas. HIV positivity on the TB patients who [AOR=0.56 (95% CI 0.39- 0.81)] was independently associated with higher proportion of unfavorable treatment outcome. Ethambutol-Isoniazid Regimen during continuation phase [AOR=0.72 (0.54-0.96)] was associated with unfavorable treatment outcome. Similarly, patients with pulmonary TB - smear positive pulmonary TB patients [AOR=0.59 (95% CI=0.35-0.99)] and Smear negative pulmonary TB patients [AOR=0.63 (95% CI=0.38-1.00)] had significantly lower treatment success as compared to extra pulmonary TB patients (Table 2).
| Variable |
Subcategory |
Treatment success, Number |
Treatment success, Percent |
Crude Odds ratio (95% CI) |
adjusted Odds ratio (95% CI) |
P value |
| Age, in years |
<15 |
132 |
89% |
1 |
|
|
| |
15-39 |
975 |
88% |
0.92 (0.54-1.6) |
|
|
| |
40-64 |
283 |
83% |
0.62 (0.35-1.1) |
|
|
| |
>64 |
54 |
84% |
0.70 (0.30-1.6) |
|
|
| Gender |
Male |
917 |
87% |
1 |
|
|
| |
Female |
527 |
86% |
0.88 (0.66-1.2) |
|
|
| Address |
Urban |
825 |
89% |
1 |
1 |
|
| |
Rural |
619 |
84% |
0.63 (0.48-0.84) |
0.62 (0.46-0.83) |
0.001 |
| HIV status |
Negative |
1,197 |
88% |
1 |
1 |
|
| |
Positive |
191 |
81% |
0.59 (0.41-0.84) |
0.56 (0.39-0.81) |
0.002 |
| |
Unknown |
56 |
88% |
0.99 (0.46-2.1) |
0.90 (0.42-1.9) |
0.786 |
| Type of Tuberculosis |
Extra pulmonary |
219 |
92% |
1 |
1 |
|
| |
Smear positive pulmonary |
462 |
86% |
0.54 (0.32-0.91) |
0.59 (0.35-0.99) |
0.048 |
| |
Smear negative pulmonary |
763 |
86% |
0.56 (0.34-0.91) |
0.63 (0.38-1.0) |
0.070 |
| Continuation phase treatment regimen |
Rifampicin-Isoniazid |
839 |
88% |
1 |
1 |
|
| |
Ethambutol-Isoniazid |
605 |
84% |
0.73 (0.55-0.97) |
0.72 (0.54-0.96) |
0.023 |
Table 2: Factors associated with TB treatment success among TB patients registered from 2009-2013 in Gamo Gofa Zone, South Ethiopia (1,444).
Discussion
Treatment success patients in this study is 86.6% (95% CI=85.0-88.3) was high and favorable treatment outcomes improved steadily over the last four years in six health facilities with high TB case load in Gamo Gofa Zone of southern Ethiopia. Being HIV negative, having extra-pulmonary TB and being on RH-based continuation phase regimen were associated with favorable treatment success.
Treatment success in this study was very good as it exceeded the earlier WHO target of 85% and is close to the Millennium Development Goal target of 87% [13]. The reason for progressive improvement of treatment outcome may be the use of DOTS treatment supporters to closely monitor and trace patients who default from treatment. The presence of health extension workers may also have contributed for this as there is well documented evidence from studies conducted in other parts of Ethiopia [14,15] that reported higher treatment success as a result of the use of community health extension workers to follow-up patients. The finding of treatment success in this study is lower than what was reported in Dabat district in Amhara region, in Tigray region and in southern Ethiopia with 87.8%, 89.2% and 89.3% respectively [14-16]. At the same time it is higher as compared to previous reports from in SNNP region [8], Bahir Dar [17], Gondar [10] and Brazil [18] which reported treatment outcomes of 74.8%, 26%, 29.5% and 75.9% respectively. These lower or under estimated achievement in the other studies could be due to the fact that large numbers of transferred-out TB patients are categorized as having unfavorable treatment outcome.
Rifampicin-Isoniazid based anti-TB Regimen in continuation phase was associated with higher rate of treatment success. This might be due to the effectiveness of RH regimen in treating TB or improvement of adherence associated with shortening treatment period from eight to six months. It might also be due to co-interventions like availability of treatment supporters associated with treatment with RH which was not present in the period EH was dispensed during continuation phase [6].
The TB/HIV co-infection in this study was 14.2%. There are lower, 10.9% [19] as well as higher reports of TB/ HIV co-infection, 52.1% [20] reported from Ethiopia which may depend on the local epidemiology of HIV. Treatment success was 81%among HIV positive and 88%among HIV negative patients, and the difference in treatment outcome was statistically significant. This is in agreement with previous studies conducted in Kolla Diba [19], Azezo [21] and Addis Ababa [22] and in Malawi [23]. This might be due to increased prevalence of toxicity, high pill burden and high death rate among HIV positive [24].
The lower treatment success among pulmonary TB patients, as compared to extra-pulmonary TB patients, observed in this study were demonstrated in one other study as well [21] but was inconsistent with other studies done in Ethiopia [10,19]. The reason for higher treatment success for patients with extrapulmonary TB may be because the commonest form of extrapulmonary TB, which is lymph node accounting for 60% of all extra-pulmonary TB cases, is a less severe disease associated higher proportion of treatment success [25]. In addition, treatment outcome is determined clinically for extra-pulmonary patients in Ethiopia for which reason they are unlikely to be classified as having treatment failure by bacteriological criteria as compared to smear positive pulmonary patients. However, the contribution of this factor may not be that much as treatment failure is generally low at around 1%.
Urban residence was associated with better treatment success. This might be due to better access to health facilities or better access to information in people living in urban areas.
One of the most important lessons to take from this study is the wide variation of treatment outcome across treatment centers. This might be due to geographic accessibility of facilities or cultural factors and provider factors. It is important to find out what worked for those with higher treatment success and replicate it in those places where it was lower. The establishment and maintenance of functional tracing mechanism at community level is very important to be able to locate patients lost to follow-up and address barriers to treatment completion there-by reducing risk of disease transmission, drug resistance or even death. Clinicians and health extension workers should also pay particular attention to HIV positive TB patients who are prone to develop other opportunistic infections which may affect their TB treatment outcome [26].
The study has strengths and limitations. We included continuation phase drug regimen as key predictor variable in our analysis. We also used data from multiple treatment sites. However, important social and clinical variables were missing from the data source which restricted our ability to do more analysis. The fact that this was a retrospective review made it impossible to get treatment outcome for patients transferredout to other facilities. This is because of the lack of feedback mechanism between facilities on final status of patients. This was handled by excluding these patients.
Conclusion
The level of treatment success in this study was encouraging at 86.6%. Transitioning continuation phase anti-TB treatment regimen from EH to RH contributed to the improvement of treatment outcome. However, more effort is needed to further improve treatment success rates among patients from rural areas, those co-infected with HIV, and patients with pulmonary TB. Factors contributing to variations in treatment outcomes among the different health facilities should be studied further.
Acknowledgement
We would like to thank Arba Minch University and Addis Continental Institute of Public Health. Our sincere gratitude also goes to all TB clinic staffs in the selected health institutions.
Authors’ Contribution
OZ: Initiated the research, wrote the research proposal, conducted the research, did data analysis and wrote the manuscript, EA: Involved in the write up of methodology of proposal and research work.
References
- World Health Organization. Global Tuberculosis Report 2014.
- Federal Ministry of Health. Quarterly health bulletin policy and practice information for action 2014; 6.
- Federal Ministry of Health. Guideline for clinical and programmatic management of TB, TB/HIV and Leprosy in Ethiopia (5th edn) Addis Ababa, Ethiopia 2013.
- Federal Ministry of Health. Comprehensive training manual for clinical and programmatic management of tuberculosis, leprosy and TB/HIV 2012.
- World Health Organization. Definitions and reporting framework for tuberculosis–2013 revision. Geneva, Switzerland 2013.
- Federal Ministry of Health. Implementation manual for transitioning continuation phase tuberculosis treatment from EH to RH. Addis Ababa, Ethiopia 2010.
- Woldeyohannes D, Kebede N, Erku W, Tadesse Z. Ten years’ experience of directly observed treatment short-course (DOTS) therapy for tuberculosis in Addis Ababa, Ethiopia. Ethiop Med J 2011; 49: 221.
- Muñoz-Sellart M, Cuevas L, Tumato M, Merid Y, Yassin M. Factors associated with poor tuberculosis treatment outcome in the southern region of Ethiopia. Int J Tuberc Lung Dis 2010; 14: 973-979.
- Lindtjørn B, Madebo T. The outcome of tuberculosis treatment at a rural hospital in Southern Ethiopia. Trop Doct 2001; 31: 132-135.
- Tessema B, Muche A, Bekele A, Reissig D, Emmrich F, et al. Treatment outcome of tuberculosis patients at Gondar University Teaching Hospital, Northwest Ethiopia: A five year retrospective study. BMC Public Health 2009; 9: 371.
- Ramos JM, Reyes F, Tesfamariam A. Childhood and adult tuberculosis in a rural hospital in Southeast Ethiopia: A ten year retrospective study. BMC Public Health 2010; 10: 215.
- Getahun B, Ameni G, Biadgilign S, Medhin G. Mortality and associated risk factors in a cohort of tuberculosis patients treated under DOTS programme in Addis Ababa, Ethiopia. BMC Infectious Diseases 2011; 11: 127.
- World Health Organization. The global plan to stop TB 2011–2015. WHO 2010.
- Berhe G, Enquselassie F, Aseffa A. Treatment outcome of smear-positive pulmonary tuberculosis patients in Tigray region, Northern Ethiopia. BMC Public Health 2012; 12: 537.
- Datiko DG, Lindtjørn B. Health extension workers improve tuberculosis case detection and treatment success in southern Ethiopia: A community randomized trial. PloS ONE 2009; 4: e5443.
- Tadesse S, Tadesse T. Treatment success rate of tuberculosis patients in Dabat, northwest Ethiopia. Health 2014; 6: 5.
- Biadglegne F, Anagaw B, Debebe T, Anagaw B, Tesfaye W, et al. A retrospective study on the outcomes of tuberculosis treatment in Felege Hiwot Referral Hospital, Northwest Ethiopia. International Journal of Medicine and Medical Sciences 2013; 5: 86-92.
- Belo M, Luiz R, Teixeira E, Hanson C, Trajman A. Tuberculosis treatment outcomes and socio-economic status: A prospective study in Duque de Caxias, Brazil. Int J Tuberc Lung Dis 2011; 15: 978-981.
- Beza MG, Wubie MT, Teferi MD, Getahun YS, Bogale SM, et al. A five years tuberculosis treatment outcome at Kolla Diba health center, Dembia District, Northwest Ethiopia: A retrospective cross-sectional analysis. J Infect Dis Ther 2013.
- Kassu A, Mengistu G, Ayele B, Diro E, Mekonnen F, et al. Co-infection and clinical manifestations of tuberculosis in human immunodeficiency virus-infected and uninfected adults at a teaching hospital, northwest Ethiopia. Journal of Microbiology, Immunology, and Infection 2007; 40: 116-22.
- Addis Z, Birhan W, Alemu A, Mulu A, Ayal G, et al. Treatment outcome of tuberculosis patients in Azezo Health Center, North West Ethiopia. International Journal of Biomedical and Advance Research 2013; 4: 167-173.
- Hailu D, Abegaz WE, Belay M. Childhood tuberculosis and its treatment outcome in Addis Ababa: A 5 years retrospective study. BMC Pediatrics 2014; 14: 61.
- Tweya H, Feldacker C, Phiri S, Ben-Smith A, Fenner L, et al. Comparison of treatment outcomes of new smear-positive pulmonary tuberculosis patients by HIV and antiretroviral status in a TB/HIV clinic, Malawi. PloS ONE 2013; 8: e56248.
- World Health Organization. Guideline for intensified TB case-findings and ionized preventive therapy for HIV positive patients in resource constrained settings. Geneva, Switzerland 2011.
- Alemie GA, Gebreselassie F. Common types of tuberculosis and co-infection with HIV at private health institutions in Ethiopia: A cross sectional study. BMC Public Health 2014; 14: 319.
- World Health Organisation. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: Recommendations for a public health approach. Geneva, Switzerland 2013.

