Terkimbi UB1*, Joseph IT2 and Barnabas E3
1Department of Obstetrics and Gynecology, Benue State University Teaching Hospital Makurdi, Nigeria
2Department of Family Medicine, Benue State University Teaching Hospital Makurdi, Nigeria
3Department of Surgery, Benue State University Teaching Hospital Makurdi, Nigeria
*Corresponding Author:
Utoo Bernard Terkimbi
Department of Obstetrics and Gynecology
Benue State University Teaching
Hospital Makurdi, Nigeria
Tel: +2348033725168
E-mail: bernardutoo@yahoo.com
Received date: 24 June, 2016; Accepted date: 26 August, 2016; Published date: 29 August, 2016
Citation: Terkimbi UB, Joseph IT, Barnabas E. Retained Post-Operative Foreign Body of Gynaecologic Origin at Ascending Colon, Gynecol Obstet Case Rep. 2016, 2:2. doi:10.21767/2471-8165.1000028
Keywords
Gossypiboma; Surgical gauze; Medico-legal; Colonic tumor
Introduction
Retention of surgical sponges following surgery though rare does occur. Many of these cases are unreported due to medico-legal implications [1,2]. In most instances, the foreign body is left in the abdomen of the patient for a period of few months to as much as 20 years [2]. A few researchers have reported retained surgical gauze in other body cavities such as; the thoracic cavity, pericardial space and paraspinal muscles [2]. Gossypiboma is the term used when referring to a piece of cotton material forgotten in a body cavity after surgical operation. The word “gossypium” in Latin means cotton, and “boma” is Swahili which means a “place of concealment”. Other historical terminologies used to describe gossypiboma are “textiloma”, “gauzeoma”, “cottoniod”, and “cottonbaloma” [2,3]. The granulomatous reaction around the foreign body can produce exudates with formation of abscess or a fibrotic mass [1,2,4]. The patient may initially be asymptomatic, but will become symptomatic after few days to 28 years [5,6]. In most cases diagnosis could be ascertained through imaging techniques such as MRI, CT scan, radiography and ultrasound [3,5]. We report a case of retained sanitary pads in the abdomen of a patient following open myomectomy at a peripheral health facility.
Case Presentation
Four months after an open myomectomy, a 38 year old nullipara developed increasingly painful abdominal swelling. She initially presented to a secondary health care facility where the post-surgical draining sinus and colicky abdominal pain were observed for two weeks, after which she was transferred to the tertiary health care facility. She had history of low grade fever, loss of appetite, constipation and weight loss, but no vomiting or diarrhoea. She did not have vaginal discharge or bleeding. There were no significant respiratory or urinary symptoms. She was in a monogamous relationship. She was a known HIV patient on highly active antiretroviral drugs (HAART) but was not diabetic or hypertensive.
On examination, she was mildly/moderately distressed, chronically ill-looking, and afebrile (Temperature-36.5°C). She was well dehydrated without pedal edema. Her cardiovascular and respiratory examinations were normal. Abdominal examination showed a right sided Para-umbilical mass approximately 8 cm × 6 cm, firm, mobile and tender, with a discharging sinus along the lower 1/3 of the surgical wound. There was no palpable organomegally. Bowel sounds were active. Pelvic examination showed a vulva smeared with copious whitish foul smelling discharge. Speculum examination revealed a healthy looking cervix with thick whitish discharge in the posterior fornix. Bimanual examination was difficult due to tenderness on the lower abdomen. There was right adnexal tenderness; none on the left and the pouch of Douglas was free. Gloved finger was stained with discharge. Digital rectal examination did not reveal anything significant. The working differential diagnoses were postsurgical abdomino pelvic abscess and colonic tumor. Ultrasound showed a normal sized homogeneous, empty uterus with a significant free fluid collection in the POD. There was a right sided abdomino pelvic mixed echogenic mass. The urinary bladder, kidneys, ureters, liver, spleen, gall bladder, pancreas and stomach were all normal. The peri-portal, peri-pancreatic and peri-aortic lymph nodes were not enlarged. The renal system was normal. Preoperative hematological and biochemical evaluation were normal.
Exploratory laparatomy revealed severe fibrinoid adhesions involving the fundus of the uterus, sigmoid colon, ascending colon and anterior abdominal wall. Two sanitary pads formed a mass in the ascending colon (Figure 1).
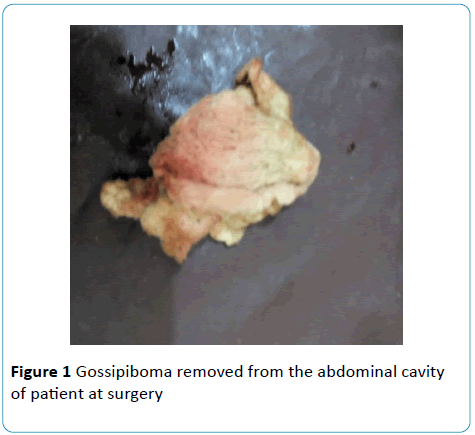
Figure 1: Gossipiboma removed from the abdominal cavity of patient at surgery.
There were bowel perforations involving the illeocecal complex and ascending colon. The ovaries and Fallopian tubes were not visualized. Estimated blood loss was 750 mls. The pads were removed. Right hemicolectomy, ileocolic anastomosis and copious abdominal lavage were performed by the general surgeon who was invited during the surgery. Perioperative antibiotic treatment was with intravenous ceftriazone 1 g 12 hourly for 72 hours, intravenous metronidazole 500 mg 8 hourly for 72 hours and intravenous 5% dextrose-saline 1 liter 8 hourly for 24 hours were administered. She had 2 units of blood transfused in order to optimized wound healing been an immunosuppressed patient. Two weeks after surgery she developed an enterocutenous fistula (ECF) which eventually healed spontaneously within 2 weeks.
Discussion
The incidence of gossypiboma is not accurately known due to poor reporting. It is however reported to vary from 0.01% to 0.03% [7]. Cotton pads, towels and sponges are usually used to control bleeding and occasionally for packing the paracolic gutters during gynaecologic surgeries. Strangely, sanitary pads instead of surgical cotton pads were used in the patient. Health workers practicing in rural health care facilities in a low resource setting like ours could do unconventional practices. However, despite precautions to ensure that surgical instruments are removed from body cavities after surgery, mistakes occur leading to gossypiboma. Clinically, abdominal gossypiboma can present with pain, distension, vomiting, diarrhoea, intestinal obstruction, fistula formation or pseudotumour [8,9]. In the case presented above the patient’s symptoms were colicky abdominal, nausea and constipation. Some authors have reported cases in which there was transmural migration of surgical sponges without an obvious incision on the bowels [3,10]. It is reported that wattanasirichaqoon from his experiments on rats explained the fate of a foreign gauze in the abdomen to include reaction, sepsis, mass and remodelling [11]. Intra-abdominal abscess and colonic tumor were the entertained diagnoses due to the low index of suspicion usually associated with retained surgical gauze. Some authors have reported long discovery time of gossypiboma. Taylor et al. reported foreign body discovery 43 years after thoracotomy [4]. In neurosurgery procedure of laminectomy a forgotten foreign body was discovered 40 years later. Sumer et al. reported foreign body extraction 23 years after caesarean section [4]. Research has shown that patient with gossypiboma are most likely to have had emergency surgeries, sudden change in surgical procedure, torrential blood loss, high BMI, long operating time, incorrect sponge count etc. [4,10]. Despite the invasion of the ascending colon without a visible breech in the wall of the bowel prior to our surgical intervention significant obstructive gastrointestinal symptoms had not occurred. This could be due to partial invasion and may be the fact that the large bowel unlike the small bowel was capable of accommodating the squeezed cotton material. Obstructive symptoms could have been more obvious if the small bowel was involved [3,12,13]. This made the impression of an abdominal abscess the most likely consideration. Hojjat et al. reported a similar experience in Iran [3]. Radiological diagnosis of gossypiboma could be difficult pre-operatively especially if the foreign body is not radio opaque. Although majority of the sponges are not radioopaque, recent researchers are focusing on the use of radioopaque and or QP coded surgical sponges [8,12,14]. In the reported case, ultrasound was utilized. The ultrasonographic appearance of sanitary pads however mimicked abscess cavity. If they are readily available, CT or MRI can be used. Treatment is necessary to preclude further morbidity and potential mortality. A high index of suspicion for gossypiboma should be entertained by surgeons caring for postoperative patients. Sponges should be tagged during surgery to avoid leaving them behind after operation. The tradition of strict swab count and record system should be sustained.
Conclusion
Meticulous surgical technique including sponge and instrument counts aimed at preventing post-operative retention of foreign materials in body cavities should be observed routinely. Junior and lower cadre of health personnel working in peripheral health facilities should undertake continuing medical training in order to reduce the incidence to a barest minimum. A high index of suspicion for retains foreign body after surgery should be entertained in patient with significant gastrointestinal symptoms and a past history of surgery.
Acknowledgement
We appreciate the resident doctors in Obstetrics and Gynaecology especially in our unit (Drs. Ameh, Icha and Okoh), the gynecology theatre nurse (Mr. James) and anesthesiologist (Dr. Efu) who were involved in the management of this patient.
References
- Monika G, Akash DA (2010) A review of medico legal consequences of gossypiboma. J Indian Acad Forensic Med 32(4): 358-361.
- Al-Farah RU, Samia S, Sanaullah G(2012) Intra-abdominal surgical gauze pseudoturmour (Gossypiboma) mimicking a dermoid cyst. Int J Pathol 10: 85-87.
- Hojjat MG, Mohsen T, Farinaz F, Mohammad EA(2010) Textiloma, migration of retained long gauze from abdominal cavity to intestine.J Res Med Sci 15:54-57.
- Indu L, Deepa K and Sandeep S(2011) Gossypiboma a rare cause of acute abdomen: A case report and review of literature. Int J CritillnInj Sci 1: 157-160.
- Kataria SP, Garg M, Marwah S, Sethi D(2012) Acute abdomen by gossypiboma. Ann Trop Med Public Health 5:511-513.
- Auquo ME, Ogbu N,Udosen J, Ekpo R, Agbor C,et al. (2006) Acute abdomen from gossypiboma: A case series and review of literature. Nig J Sur Research 8: 174-176.
- Tzeng JE, Wei CK, Chang SM, Lin CH(2006) Surgical Gauze pseudoturmour (Gauzoma)-A case report. Tsu Chi Med J 18:49-51.
- Mehmet K, Halil II(2010) A new complication of retained surgical gauze: Development of malignant fibrous histiocytoma-report of a case with a literature review. W Jsurgoncol10:139.
- Aziz SM, Ali C, Omer U, Vedat B, Cetin K, et al. (2010) Gossypiboma: Retained surgical sponge after a gynecologicprocedure. Case reports in medicine.
- Arikan S, Kocakusak A(2015) Retained textile foreign bodies: Experience of 27 years. Acta med Port 28:494-500.
- Ukwenya AY, Dogo PM, Ahmed A, Nmadu PT(2006) The retained surgical sponge; following laparatomy, forgotten at surgery, often forgotten at diagnosis. Our experience. Nig J Sur Res 8:164-168.
- Hariharan D, Lobo DN(2013) Retained surgical sponges, needles and instruments. Ann R Coll Surg Engl 95: 87-92.
- Aminian A (2008) Gossypiboma: a case report. Cases J1:220.
- Gencosmanoglu R, Inceoglu R(2003) An unusual cause of small bowel obstruction: Gossypiboma-case report. BMC surgery 3:6.

