Keywords
Hepatectomy; Pancreatic Carcinoma; surgery
INTRODUCTION
Despite improved outcomes for many cancer patients over the past several decades, pancreatic carcinoma (PC) remains one of the most devastating and highly lethal malignancies, with a 5-year survival rate of only 6.9% in Japan [1]. Specifically, the prognosis of patients who have metastatic disease is extremely poor. Liver is the most common site of distant metastasis from PC, followed by the peritoneum and lung [2]. As the presence of liver metastasis has been regarded to be a sign of disseminated disease, surgery for liver metastatic PC has been discouraged, even if the disease is technically resectable. Thus, therapeutic approach towards liver metastatic PC almost entirely consists of chemotherapy.
In other fields of oncological surgery, most commonly in colorectal cancer, benefits of resection for liver metastases has been established. Even patients with multiple bilobar metastases can sometimes be successfully treated with liver resection with ablative therapy, two-step surgery or portal vein embolization [3]. This progress depends to a large extent on the introduction of novel chemotherapeutic agents that has considerably contributed to increasing response rates, resectability rates and survival.
Since gemcitabine was approved for the treatment of PC in 2001, gemcitabine monotherapy has been the only standard treatment for advanced PC. Recently newer agents such as S-1, nab-paclitaxel, erlotinib and regimens such as FOLFIRINOX have become available with increasing expectation for better response rates and extended survival [4-7]. Nevertheless, the overall median survival for PC patients with metastatic disease still remains less than 1 year. Given such an aggressive biology of PC, multimodal approach is needed to further improve outcomes.
There have been reports suggesting that surgery may also be a treatment of choice for selected patients with liver metastases from PC, particularly for those with a solitary tumor [8,9]. However, it is likely that a certain proportion of patients with multiple liver tumors can benefit from aggressive surgery, provided that durable disease control is obtained by chemotherapy.
We herein review our series of 8 PC patients with multiple liver metastases (MLM) who underwent adjuvant surgery after objective response to combination chemotherapy.
PATIENTS AND METHODS
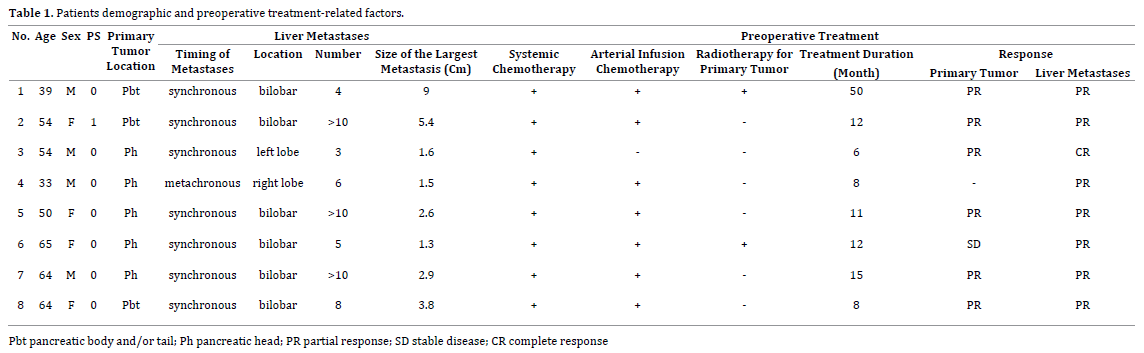
Between February 2011 and May 2014, 8 patients underwent adjuvant surgery for locally resectable PC with MLM in our institute. The patients included 4 males and 4 females, and their mean age was 53 years (range: 33-65 years). Details of the patients are given in Table 1. The primary tumor was located in the pancreas head in 5, and in the body or tail in 3. Seven (88%) of the 8 patients had synchronous MLM. One patient with metachronous MLM exhibited hepatic recurrence 8 months after primary surgery (T3N1M0; R0; pathological stage: IIB) followed by 6 months of systemic adjuvant chemotherapy with gemicitabine. Six patients (75%) had bilobar involvement; 3 of them suffered from more than 10 metastatic foci in their liver. Patients with extrahepatic metastatic disease, such as peritoneal disease, were not included. All patients received systemic combination chemotherapy, and 7 of the patients were also given hepatic arterial infusion chemotherapy. Radiotherapy for primary pancreatic lesion was applied in 2 patients.
Combination Chemotherapy
Depending on the clinical setting, we have conducted modified chemotherapy using gemcitabine and S-1 in combination with docetaxel and carboplatin for metastatic or unresectable PC patients. These cytotoxic agents were administered with itraconazole, a commonly used antifungal that inhibits Hedgehog pathway, P-glycoprotein, and angiogenesis [10]. On day 1, the starting doses of intravenous gemcitabine, docetaxel, and carboplatin were 1,000 mg/m2, 35 mg/m2, and 4 mg·min−1·mL−1 (area under the curve), respectively. S-1 was administered at 80 mg/m2 orally from day 1 to day 3. An oral itraconazole solution was also administered at a daily dose of 400 mg (days −2 to 2). This regimen was repeated every 2 weeks. When distant metastases predominantly involve the liver, hepatic artery infusion reservoir was implanted and thereafter carboplatin and gemcitabine was administered intraarterially. Chemotherapy dose reduction and/or dose delay were properly employed in response to toxicity. Briefly, the dose of docetaxel was reduced by 5 mg/m2 for subsequent cycles if grade 4 neutropenia was observed. Granulocyte colony stimulating factor was administered according to the manufacturer’s recommendations until the absolute neutrophil counts recovered. If grade 3-4 thrombocytopenia occurred, the carboplatin dose in the next cycle was reduced by 10%. The doses of gemcitabine, S-1 and itraconazole were fixed in principle.
Details of the therapeutic options were given to the patients, and the treatment was started after informed consent. The antitumor responses were evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1 [11].
Adjuvant Surgery
Patients were considered for adjuvant surgery if significant decrease in size and number of metastases without appearance of new lesions was obtained with chemotherapy for a sufficient period of time. However, candidates for surgery were carefully selected by evaluating patients’ age and their general condition. Each patient was counseled on the procedure and the alternative therapeutic options, and gave written informed consent before the surgery.
STATISTICS
Overall survival was calculated from the date of chemotherapy initiation as well as from the date of adjuvant surgery until the patients succumbed to any cause or until the last follow-up. Survival distributions were estimated by the Kaplan–Meier method.
RESULTS
Responses and Toxicities to Preoperative Combination Chemotherapy
The median follow-up time from initiation of chemotherapy to adjuvant surgery in all 8 patients was 11 (range 6-50) months. Among 7 patients with synchronous disease, partial response (PR) as documented by CT imaging of the primary tumor was observed in 6 patients and stable disease in 1 patient. With regard to the liver tumors, 1 patient achieved complete response (CR) and all the remaining 7 had PR. Examples of CT images demonstrating PR in primary and metastatic lesions were shown in Figure 1.
Figure 1. Contrast enhance CT demonstrating pancreas head carcinoma
(arrowheads) with multiple liver metastases before (left) and after (right)
systemic combination chemotherapy with hepatic arterial infusion (case
No. 5).
During the course of preoperative treatment, grade 3 or 4 neutropenia and thrombocytopenia were noted in 8 (100%) and 5 (63%) of the patients, respectively. No patient experienced febrile neutropenia. Non-hematologic toxicities, such as peripheral neuropathy, were grade 2 or less.
Perioperative Data and Adjuvant Surgery
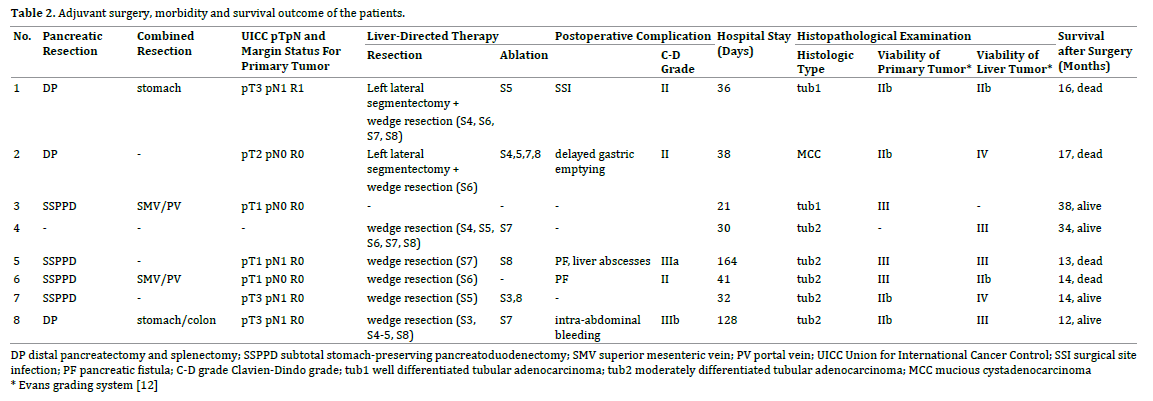
One patient underwent liver resection alone for metachronous disease. Except for 1 patient in whom liver metastases had radiological CR, 6 patients with synchronous disease underwent simultaneous pancreatic and liver resection. Surgical resection of the primary tumor involved a subtotal stomach-preserving pancreatoduodenectomy (n=4) and distal pancreatectomy with splenectomy (n=3). Combined organs resection included gastric wedge resection and/or partial transverse colon resection. Vascular reconstruction was required in 2 patients. Accordingly, local tumor free (R0) resection margins could be achieved in 6 (86%) of the 7 patients. The distribution of liver resection procedures is listed in Table 2, all patients underwent minor liver resections, with the most common procedure being a wedge resection. Six patients underwent concomitant liver resection and radiofrequency ablation, while 1 patient underwent resection alone. The median operative time of the 8 patients was 521 (range 450–606) min, and the median intraoperative blood loss was 1232 (range 430–1800) mL. Five (63%) patients had a total of 6 postoperative complications: International Study Group on Pancreatic Fistula (ISGPF) grade B pancreatic fistula (n=2); wound infection (n=1); delayed gastric emptying (n=1); liver abscesses (n=1) and intra-abdominal bleeding (n=1). One patient who developed sudden intra-abdominal bleeding from the liver resection surface at postoperative day 21 consequently required surgical intervention. There was no postoperative hospital death or death related to surgical procedure. The median length of hospital stay was 36 (range 21–164) days. Chemotherapy was resumed for all patients after they had recovered from surgery, and was continued as long as the disease is controlled with manageable toxicity.
Histopathological Findings
All resected tumors were histopathologically proved to be invasive exocrine PC (8 tubular adenocarcinomas and 1 mucinous cystadenocarcinoma). The tumor viability of the primary pancreatic lesion, as judged by the Evans grading system [12], was grade IIb in 4 patients and grade III in 3. The resected liver specimens on the other hand were identified as grade IIb in 2 patients, grade III in 3 and grade IV in 2 (Table 2). Thus, all of the patients had at least 50% of tumor cell destruction. Chemotherapy-associated liver steatosis and sinusoidal injury was confirmed in 4 and 3 patients, respectively.
Survival Outcome
With a median follow up of 29 months (range, 20-66 months), 4 of 8 patients died of recurrent disease, 2 are alive with disease and 2 remain disease free. All the 8 patients survived 1 year or more from adjuvant surgery, with a median postoperative survival of 17 months (range: 12-38 months). As a result, an estimated overall survival at 2- and 3-years from initiation of chemotherapy reached 86% and 54%, respectively (Figure 2).
Figure 2. Survival of the patients after initiation of chemotherapy. An
estimated 2- and 3-year overall survival was 86% and 54%, respectively.
DISCUSSION
In the present study, we enrolled PC patients with MLM who received combination chemotherapy and following adjuvant surgery. It should be noted that surgery in our series was not necessarily intended to be curative, but rather designed to remove all or as much of the residual tumor as possible, as part of a multimodal treatment.
For patients who have locally advanced or metastatic PC, palliative resection has usually been contraindicated due to its poor prognosis and high morbidity [13,14]. However, considering that many resectable PC patients who undergo a “curative” resection die of recurrent cancer, that indicates the presence of residual micrometastasis at the time of resection, most pancreatic resection for PC can be considered as a palliative surgery. Several series in the literature have demonstrated a survival benefit of palliative resection in comparison to palliative bypass surgery [15-17]. Bockhorn et al. [15], for example, reported that prolonged survival was achieved even when pancreatic resection ended in R2 status, as compared with bypass procedures (Median survival: 11.5 vs. 7.5 months). These findings suggest that tumor debulking surgery may be justified in a carefully selected population.
Currently, experience with surgery for liver metastatic PC are only limited to a few patients. Takada et al. [18] in 1997 showed no improvement of survival despite aggressive surgery for PC with MLM, although in their study liver resection was performed without preoperative chemotherapy. Their result was underlined by the study of Gleisner et al. [19] who found no survival benefit of concomitant resection of PC with single liver metastases compared to a palliative procedure. In contrast, a metaanalysis of 3 case reports and 18 studies including 103 patients has shown that overall survival in cases with one or few liver metastases which are concomitantly resected was comparable to cases without evidence of metastases [9]. In an analysis of 15 patients who underwent surgery for isolated liver metastases, Zanini et al. [20] recently reported that median overall survival was significantly higher in patients with metachronous metastases than in those with synchronous disease (11.4 vs 8.3 months). The survival outcome of our series seemed to be more favorable than that reported in previous studies, wherein patients with multiple and/or synchronous liver metastases did not benefit from resection. However, considering the profile of our 2 patients who survived more than 2 years after adjuvant surgery with no evidence of recurrence; in one patient 3 metastatic liver tumors had disappeared on radiologic evaluation after successful preoperative chemotherapy, and in another patient metachronous MLM was resected 17 months after pancreatoduodenectomy for the primary tumor, it was speculated that probability of long-term survival after surgery for liver metastatic PC greatly depends on the metastatic tumor volume and timing of metastases.
With continuous progress in the field of abdominal surgery, pancreatic resection with synchronous liver resection seems technically feasible nowadays. However, relatively high surgical morbidity following pancreatectomy, especially pancreatic fistula, remains an unsolved problem. A synchronous liver resection carries the additional risk of bile leakage, hemorrhage, or abscess formation in the dead space. Major hepatectomy with pancreatoduodenectomy is usually indicated for the resection of advanced biliary malignancies and associated with high morbidity and mortality, leading to an underestimation of the survival benefit of surgery [21]. We avoided major hepatectomies but instead applied thermal ablation for deep located tumors to preserve liver parenchyma and thereby to reduce the risk of serious postoperative complications such as liver failure. Combined intra-operative ablation and resection is also proposed to treat extensive colorectal liver metastases [22]. In the current study, 1 patient who had undergone pancreatoduodenectomy with concomitant ablative therapy developed late-onset liver abscesses, although they were treatable with antibiotics and percutaneous drainage. The increased risk of developing liver abscess after ablative therapy or after hepatic arterial infusion chemotherapy in patients undergoing enterobiliary anastomosis cannot be ignored [23, 24]. Occurrence of major postoperative complications, which can sacrifice patient quality of life and can cause significant delay in resuming chemotherapy, may outweigh the potential benefit of surgery. Careful patient observation, early recognition and treatment of postoperative complication are mandatory, especially in this clinical situation.
It remains to be proven whether adjuvant surgery can prolong survival in PC patients with MLM compared to chemotherapy alone. In the current study, all resected primary tumor contained varying numbers of viable appearing tumor cells even after chemotherapy given for a sufficiently long duration. In a series of 135 PC patients treated with chemoradiation followed by pancreatectomy, Chun et al. [25] demonstrated that major pathological response at time of surgical resection was associated with improved overall survival. It is likely that patients with residual viable cancer after adequate non-surgical treatment may benefit from adjuvant surgery, even in those with metastatic liver lesions. To elucidate the efficacy of adjuvant surgery, however, prospective controlled trials are required.
Adjuvant surgery is still an individual approach for selected patients only, as there is a selection bias in our study, such as good responders to chemotherapy and relatively young patients in good general condition. However, our results indicate that liver metastatic PC may not necessarily be a contraindication to surgery, even in cases involving multiple liver lesions. Multimodal approach consisting of combination chemotherapy and surgery may offer a chance for selected patients to gain valuable survival time. We hope future progress in non-surgical treatments will broaden surgical indication for this dismal disease, with resultant improvement in survival.
Conflicting Interest
The authors declare that they have no conflicts of interest.
References
- Kuroda T, Kumagi T, Yokota T, Seike H, Nishiyama M, Imai Y, Inada N, et al. Improvement of long-term outcomes in pancreatic cancer and its associated factors within the gemcitabine era: a collaborative retrospective multicenter clinical review of 1,082 patients. BMC Gastroenterol 2013; 13: 134. [PMID: 24256464]
- Yachida S, Iacobuzio-Donahue CA. The pathology and genetics of metastatic pancreatic cancer. Arch Pathol Lab Med 2009; 133: 413-22. [PMID: 19260747]
- Clark ME, Smith RR. Liver-directed therapies in metastatic colorectal cancer. J Gastrointest Oncol 2014; 5: 374-87. [PMID: 25276410]
- Ueno H, Ioka T, Ikeda M, Ohkawa S, Yanagimoto H, Boku N, Fukutomi A, et al. Randomized phase III study of gemcitabine plus S-1, S-1 alone, or gemcitabine alone in patients with locally advanced and metastatic pancreatic cancer in Japan and Taiwan: GEST study. J Clin Oncol 2013; 31: 1640-8. [PMID: 23547081]
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, Seay T, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013; 369: 1691-703. [PMID: 24131140]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, Au HJ, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer : a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol 2007; 25: 1960-6. [PMID: 17452677]
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, Adenis A, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364: 1817-25. [PMID: 21561347]
- Buc E, Orry D, Antomarchi O, Gagnière J, Da Ines D, Pezet D. Resection of pancreatic ductal adenocarcinoma with synchronous distant metastasis: is it worthwhile? World J Surg Oncol 2014; 12: 347. [PMID: 25407113]
- Michalski CW, Erkan M, Hüser N, Müller MW, Hartel M, Friess H, Kleeff J. Resection of primary pancreatic cancer and liver metastasis: a systematic review. Dig Surg 2008; 25: 473-80. [PMID: 19212120]
- Tsubamoto H, Sonoda T, Yamasaki M, Inoue K. Impact of combination chemotherapy with itraconazole on survival for patients with recurrent or persistent ovarian clear cell carcinoma. Anticancer Res 2014; 34: 2007-14. [PMID: 24692739]
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: 228-47. [PMID: 19097774]
- Evans DB, Rich TA, Byrd DR, Cleary KR, Connelly JH, Levin B, Charnsangavej C, et al. Preoperative chemoradiation and pancreaticoduodenectomy for adenocarcinoma of the pancreas. Arch Surg 1992; 127:1335-9. [PMID: 1359851]
- Gillen S, Schuster T, Friess H, Kleeff J. Palliative resections versus palliative bypass procedures in pancreatic cancer--a systematic review. Am J Surg 2012; 203: 496-502. [PMID: 21872208]
- Tol JA, Eshuis WJ, Besselink MG, van Gulik TM, Busch OR, Gouma DJ. Non-radical resection versus bypass procedure for pancreatic cancer - a consecutive series and systematic review. Eur J Surg Oncol 2015; 41: 220-7. [PMID: 25511567]
- Bockhorn M, Cataldegirmen G, Kutup A, Marx A, Burdelski C, Vashist JK, Mann O, et al. Crossing the Rubicon: when pancreatic resection with curative intent ends in an R2 status. Impact of "desmoplastic pseudo-pancreatitis" and anatomical site of irresectability. Ann Surg Oncol 2009; 16:1212-21. [PMID: 19225843]
- Lillemoe KD, Cameron JL, Yeo CJ, Sohn TA, Nakeeb A, Sauter PK, Hruban RH, et al. Pancreaticoduodenectomy. Does it have a role in the palliation of pancreatic cancer? Ann Surg 1996; 223: 718-25. [PMID: 8645045]
- Wang SE, Shyr YM, Su CH, Chen TH, Wu CW. Palliative pancreaticoduodenectomy in pancreatic and periampullary adenocarcinomas. Pancreas 2012; 41: 882-7. [PMID: 22286381]
- Takada T, Yasuda H, Amano H, Yoshida M, Uchida T. Simultaneous hepatic resection with pancreato-duodenectomy for metastatic pancreatic head carcinoma: does it improve survival? Hepatogastroenterology 1997; 44: 567-73. [PMID: 9164539]
- Gleisner AL, Assumpcao L, Cameron JL, Wolfgang CL, Choti MA, Herman JM, Schulick RD, et al. Is resection of periampullary or pancreatic adenocarcinoma with synchronous hepatic metastasis justified? Cancer 2007; 110: 2484-92. [PMID: 17941009]
- Zanini N, Lombardi R, Masetti M, Giordano M, Landolfo G, Jovine E. Surgery for isolated liver metastases from pancreatic cancer. Updates Surg 2015; 67: 19-25. [PMID: 25702263]
- Ebata T, Yokoyama Y, Igami T, Sugawara G, Takahashi Y, Nimura Y, Nagino M. Hepatopancreatoduodenectomy for cholangiocarcinoma: a single-center review of 85 consecutive patients. Ann Surg 2012; 256: 297-305. [PMID: 22750757]
- Karanicolas PJ, Jarnagin WR, Gonen M, Tuorto S, Allen PJ, DeMatteo RP, D'Angelica MI, et al. Long-term outcomes following tumor ablation for treatment of bilateral colorectal liver metastases. JAMA Surg 2013; 148: 597-601. [PMID: 23699996]
- Elias D, Di Pietroantonio D, Gachot B, Menegon P, Hakime A, De Baere T. Liver abscess after radiofrequency ablation of tumors in patients with a biliary tract procedure. Gastroenterol Clin Biol 2006; 30: 823-7. [PMID: 16885864]
- Hashimoto A, Nishiofuku H, Tanaka T, Sho M, Anai H, Nakajima Y, Kichikawa K. Safety and optimal management of hepatic arterial infusion chemotherapy after pancreatectomy for pancreatobiliary cancer. AJR Am J Roentgenol 2012; 198: 923-30. [PMID: 22451562]
- Chun YS, Cooper HS, Cohen SJ, Konski A, Burtness B, Denlinger CS, Astsaturov I, et al. Significance of pathologic response to preoperative therapy in pancreatic cancer. Ann Surg Oncol 2011; 18: 3601-7. [PMID: 21947697]



