Keywords
Chemotherapy, Adjuvant; Pancreatic Neoplasms; Radiotherapy, Adjuvant
INTRODUCTION
Although surgical resection is the only treatment modality that provides the potential for cure in patients with pancreatic adenocarcinoma, postoperative patients receiving no further treatment remain at a very high risk for local and distant relapse. Starting with the Gastrointestinal Tumor Study Group (GITSG) study [1] in 1985 and then followed by Whittington et al. [2] in 1991, improved survival has been demonstrated with adjuvant chemoradiotherapy. Over the subsequent years, multiple reports have evaluated the role of adjuvant therapy and have shown improved clinical outcomes, including overall survival, with adjuvant therapy when compared with surgery alone [3, 4, 5, 6]. Nonetheless, controversies abound regarding the exact role and benefit of adjuvant chemoradiotherapy [7, 8, 9, 10, 11, 12], and clinicopathological factors that may serve as predictive and/or prognostic variables are not well-defined [13, 14, 15, 16, 17, 18, 19]. In this retrospective analysis, we report the experience with adjuvant chemoradiation after pancreaticoduodenectomy or total pancreatectomy at the University of Pennsylvania and provide an analysis of commonly accepted clinicopathological factors to determine their prognostic value for favorable survival in this population.
METHODS
Study Population
We created a secure database of all pancreatic cancer patients consecutively treated at the Hospital of the University of Pennsylvania from 1981 to 2006. After cross-referencing with the Department of Radiation Oncology medical record system, a total of 91 patients with adenocarcinoma of the pancreas were identified that were treated with adjuvant chemoradiation, and represent the patient populations for this analysis.
Data Collection
All T and N stages were included; stage coding was by AJCC 7th edition criteria. Data collected included demographics (age, gender, race), location of pancreatic tumors (head vs. body/tail), and pathologic features (size, histologic grade, nodal status, and resection status). Microscopic versus gross residual disease was verified by careful review of both operative and pathology reports. Final pathological coding was confirmed with a pathologist specializing in gastrointestinal malignancies (E.E.F.). Time points included in this analysis consisted of dates of surgery, discharge and adjuvant treatment. Radiation Oncology Department clinic charts were reviewed to collect treatment details. Death dates were determined via the Social Security Death Index.
Treatment
Twelve surgeons performed all pancreatic resections at our institution during the study period. However, a single surgeon (E.F.R.) performed a majority (twothird) of these resections. The 30- and 60-day crude mortality rates for all resections of malignant lesions from the pancreaticoduodenobiliary tract during the study period were 1.8% and 3.4%, respectively (n=572).
The use of concurrent chemoradiotherapy in the postoperative setting became routine at the University of Pennsylvania in 1984, and therefore, only patients treated during or after 1984 are included. While detailed chemotherapy data were not available for some patients, documented records in the Radiation Oncology clinic notes confirmed that all patients in this report received a 5-FU-based regimen of concurrent chemoradiotherapy. Prior to 1986, our institutional policy was to treat patients with bolus 5-FU (500 mg/m2/day) on the first three and last three days of radiation. This regimen evolved to the use of a 96 h 5- FU infusion (1,000 mg/m2/day) during the first and fifth weeks of radiation. In 1991, the treatment policy changed to 5-FU by protracted infusion (250 mg/m2/day) continuously throughout the course of radiation. Patients who tolerated radiation and completed treatment with a performance status of 1 or 2 generally received maintenance chemotherapy after completion of adjuvant chemoradiotherapy with bolus 5-FU, 5-FU with low dose folinic acid, or gemcitabine. All patients were treated with high-energy (megavoltage) photons delivered with a linear accelerator, and CT-defined clinical target volumes routinely included adjacent nodal beds. Patients were treated to 48.6 or 50.4 Gy, but some patients with R1 or R2 resections were treated to higher doses (54.0, 59.4 or 63.0 Gy). Eighty-eight patients (96.7%) completed their prescribed radiation dose.
ETHICS
The secure database was created after approval from the University of Pennsylvania Institutional Review Board.
The written informed consent was obtained for all investigations made according to the usual clinical practice. The study protocol was approved by the institutional review committee. The study protocol conforms to the ethical guidelines of the World Medical Association Declaration of Helsinki.
STATISTICS
Overall survival was defined from the date of surgery to the date of death due to any cause, or censored at last patient contact. The 5-year overall survival rate was estimated by the Kaplan-Meier method and was reported together with the standard error (SE). The hazard ratio and statistical significance of each clinical factor was assessed by Cox regression analysis. To determine whether clinical factors were significant independent prognostic factors, multivariate modeling was performed using Cox regression analysis using a backward elimination selection strategy. Prior to modeling, tumor variables that were significant by univariate regression analysis (T stage, N stage, number of lymph nodes involved and resection status) were tested for collinearity by a linear trend test. These results were used to arrive at a parsimonious final model. All analyses were performed in SPSS version 17.0 (SPSS Inc., Chicago, IL, USA), and two-tailed P values less than 0.05 were considered statistically significant.
RESULTS
Patient and Disease Characteristics
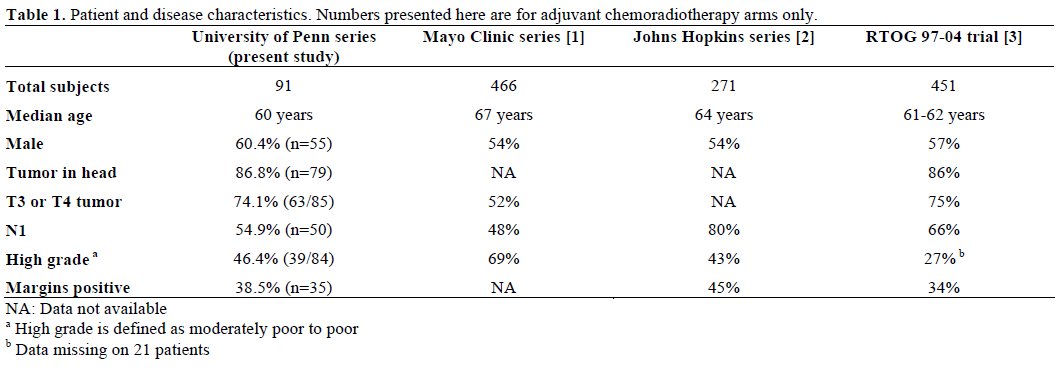
A comparison of these characteristics with other large series of pancreatic cancer patients treated with adjuvant chemoradiotherapy is presented in Table 1. Demographic and disease characteristics of the patients in this analysis are shown in Table 2. The majority of patients were Caucasian (72 patients, 79.1%); men comprised 60.4% of the study population (55 patients). The median age was 60 years. Tumors were predominately located in the head of the pancreas (79 patients, 86.8%). The majority (63 patients, 69.2%) were T3/T4 and over half (50 patients, 54.9%) had nodal involvement. High grade tumors (39/84 patients, 46.4%) and positive resection margins (35 patients, 38.5%) were seen in less than half of the cases.
Survival Outcomes
The median follow-up was 6.5 years for all patients. Of the 91 patients in the series, 64 (70.3%) are deceased. The median survival from the date of surgery was 2.3 years (95% confidence interval 1.5-3.2 years). The overall survival rate (±SE) at 2 and 5 years was 56.2±5.4% and 28.9±5.5%, respectively (Figure 1). For the 27 patients alive at last contact, the median followup was 2.8 years.
Figure 1. Overall survival after surgical resection for pancreatic adenocarcinoma. Median follow up was 6.5 years, and the median
overall survival was 2.3 years. Crosses represent censored patients.
Characteristics Associated with Survival
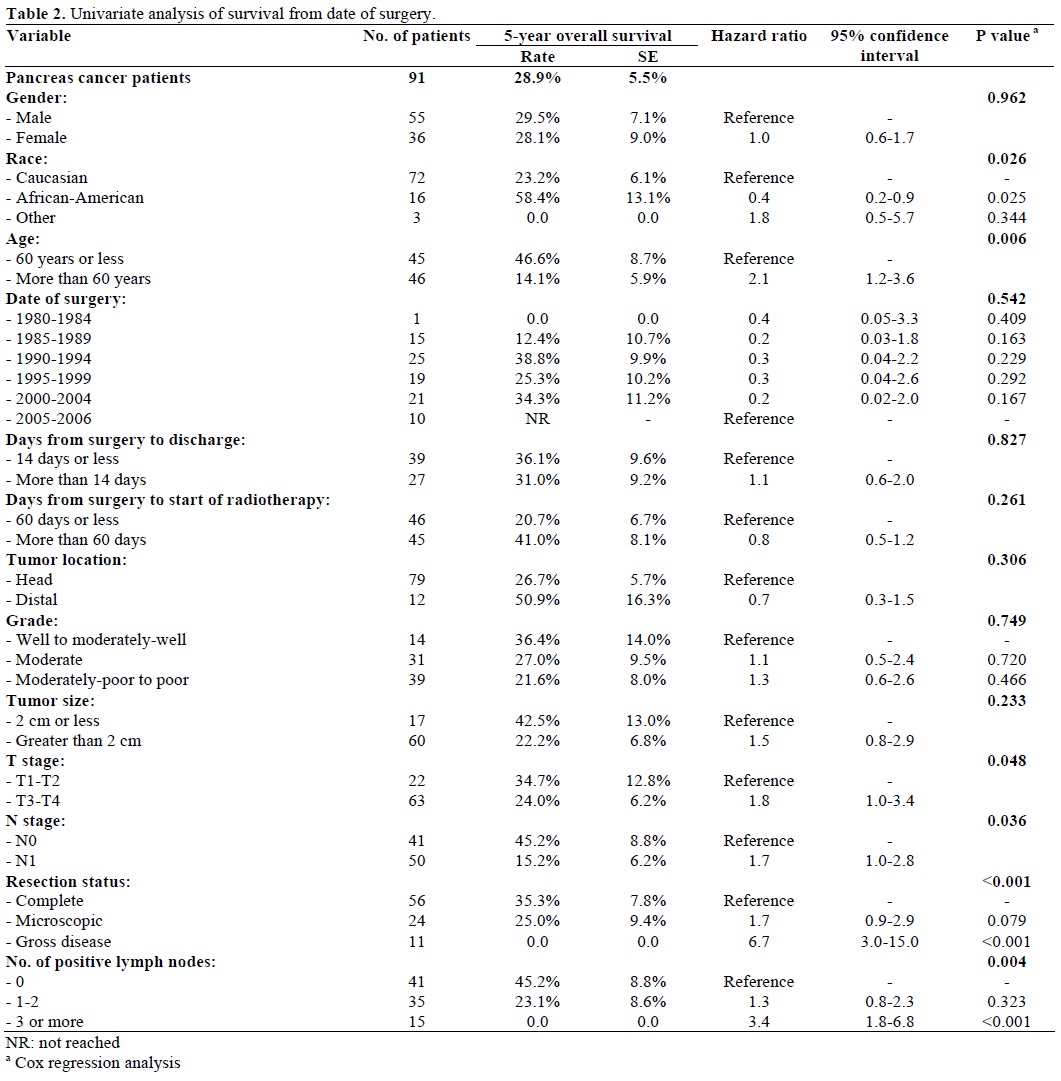
Gender was not significantly associated with overall survival (P=0.962), but race was (P=0.026), with 5- year overall survival rates (±SE) of 58.4±13.1% for African-American and 23.2±6.1% for Caucasian patients (Table 2). Age, dichotomized at the median (60 years), was also found to be significantly associated with overall survival (P=0.006). The 5-year overall survival rate for patients older than 60 years was 14.1±5.9% and for patients up to 60 years was 46.6±8.7%, with a corresponding hazard ratio (HR) of 2.1 (Figure 2a).
Figure 2. Overall survival after surgical resection for pancreatic
adenocarcinoma by age group (a.), number of positive lymph nodes
(b.), and resection status (c.).
Patients with T1-T2 lesions had significantly better overall survival than patients with T3-T4 lesions (5- year survival 34.7±12.8% vs. 24.0±6.2%, P=0.048). Both the American Joint Committee on Cancer (AJCC) nodal status (N1 vs. N0) (HR 1.7, P=0.036), and the number of positive lymph nodes showed a statistically significant association with overall survival. We defined cutoffs for number of positive lymph nodes as 0, 1-2 or more than 2. The 5-year overall survival rates for these three groups were 45.2±8.8%, 23.1±8.6% and 0%, respectively (P=0.004, Figure 2b). Resection status was also strongly associated with overall survival (P<0.001, Figure 2c). The 5-year overall survival rates were 35.3±7.8%, 25.0±9.4% and 0% for R0, R1 and R2 patients, respectively. Tumor location within the pancreas, histological grade and tumor size dichotomized at 2 cm were not significantly associated with overall survival.
Given ongoing improvements in surgical technique and perioperative care, we evaluated the impact of treatment era and stratified patients by 5-year increments according to year of surgery. There was no association between overall survival and study period (P=0.542). Five-year overall survival rates were consistently at or above 25% from 1990 onward. Duration of hospital stay and interval from surgery to the initiation of adjuvant therapy, each dichotomized at the median value, were also not significantly associated with survival (P=0.827 and P=0.261, respectively).
Multivariate Analysis
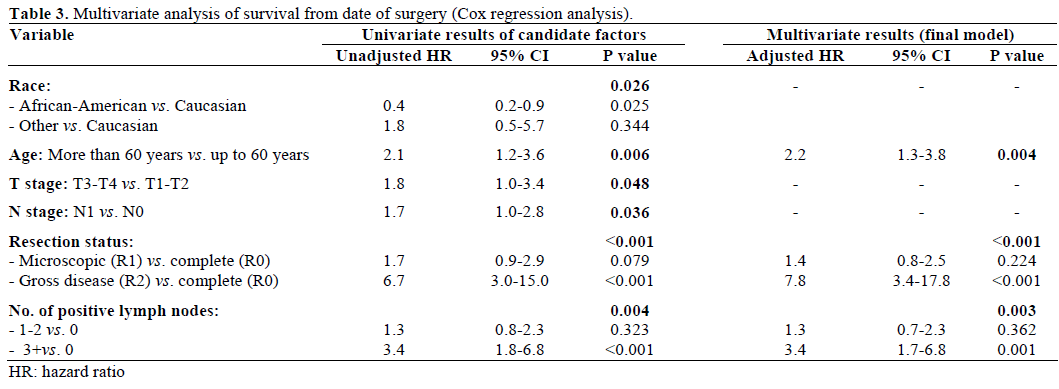
To determine whether the factors found to be significant in univariate analyses were independent prognostic factors, a multivariate analysis was undertaken, taking into account collinearity among variables. T stage was found to be strongly associated with resection status (P=0.003) and was thus not retained in the final model. There was a weak association between resection status and the number of positive lymph nodes (P=0.106) with a fewer nodepositive patients who had R0 resections. Resection status, age (dichotomized at 60 years) and the number of positive lymph nodes (in 3 groups, as defined earlier) were found to be independent predictors of survival from surgery (Table 3). Resection status stood out as the most strongly associated characteristic, with gross residual disease (R2) having an adjusted hazard ratio of 7.8 (95% CI: 3.4-17.8), when compared to no residual disease (R0).
DISCUSSION
Adjuvant Therapy Outcomes and Prognostic Variables
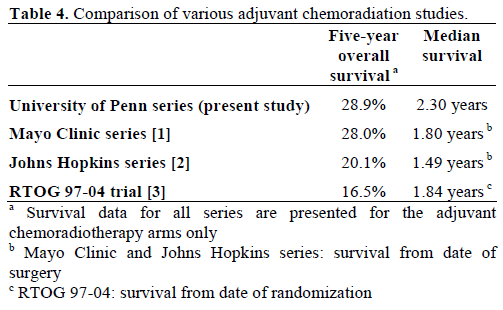
At the University of Pennsylvania, we have offered postoperative chemoradiotherapy routinely for over two decades to all patients with pancreatic cancer who have undergone potentially curative surgical resection. In 91 patients treated, a 5-year overall survival rate of 28.9% and a median survival of 2.3 years has been achieved. These results compare favorably with similar reports of postoperative adjuvant chemoradiotherapy, where 5-year overall survival rates range from 16.5% to 28.0% and median survival ranges from 1.49 to 1.84 years (Table 4). The EORTC study reported a 5-year overall survival rate of 20% and a median survival of 1.43 years for pancreatic head tumor patients [20]. In addition, the 5-year overall survival results reported by ESPAC-1 were 13% and 7% in patients who received postoperative chemoradiotherapy with or without maintenance chemotherapy, respectively [5]. Also, in the American College of Surgeons Oncology Group (ACOSOG) Z05031 multi-institutional phase II study, which continues to report some of the most favorable results presented to date, 89 patients treated with postoperative radiotherapy to 50.4 Gy with concurrent protracted venous infusion of 5-FU, cisplatin and interferon-alpha achieved a median survival time of 2.26 years [21, 22].
In an attempt to identify independent prognostic factors that may be associated with survival after adjuvant chemoradiotherapy, in univariate we found that gender, primary tumor location (pancreatic head versus distal site), and histologic grade, as well as race in the successive multivariate analysis, all failed to demonstrate associations with survival in this series. Our results, however, indicate that age (dichotomized at 60 years), resection status and number of positive lymph nodes were strongly, and independently, associated with survival. Although T stage and resection status were strongly associated, only resection status was retained in the final multivariate model and thus should be viewed as a superior predictor of survival. In most other major series, resection status, T and N stages, and tumor grade, in various combinations, are the variables that have been consistently shown to be associated with survival outcomes [5, 14, 15, 20]. While our results are similar, they indicate that resection status may be the primary determinant of outcomes, and that the number of positive lymph nodes may be a better prognosticator than a simple binary lymph node variable (N0 vs. N1). Keeping in line with this observation, the planned subset analysis by the ACOSOG Z05031 study also failed to identify a prognostic value for T1-T2 vs. T3- T4, tumor size (less than 3 cm), and nodal status [21]. Resection of T4 tumors is only partial by nature, and the lack of long term survivors with R2 resections emphasizes the importance of achieving complete resections when the intent is curative. Although not all series agree on the same age cutoff, we found that age less than 60 years was strongly associated with survival.
In our current report, 97% of patients were able to safely complete their prescribed radiation dose. We believe adequate nutritional support plays an important role and have provided a separate analysis from our experience elsewhere [23]. This includes close attention to nutritional concerns, including the common practice of leaving in place a feeding jejunostomy tubes by at least one surgeon (E.F.R.).
Study Limitations
The authors acknowledge that retrospective collection of data from a single institution limits interpretation of our findings. Many patients following resection sought their adjuvant therapy outside of our institution, and the long-term outcomes for these patients were not analyzed. Yet, it should be emphasized that our study population was inclusive of all patients who completed trimodality therapy at our institution with a broad age range (32-81 years) and included 11 patients with grossly positive margins and 10 patients with invasion of the superior mesenteric artery or celiac axis. There has long been a uniform policy to offer trimodality therapy to patients with both favorable and unfavorable pathologic factors, and this is easily identifiable in our dataset with inclusion of pT1N0 lesions with negative margins as well as pT4 lesions, which by definition have grossly positive margins. CA 19-9 levels, which have also been shown to be prognostic in other series, were not available for all of these patients due to the treatment era.
Ultimately, a prospective randomized trial of postoperative chemotherapy with and without radiation is needed to help resolve the controversy regarding the role of adjuvant therapy and prognostic variables for pancreatic cancers. A recently conducted randomized phase II/III study of adjuvant gemcitabine with and without radiation therapy for pancreatic cancer was reported. The study has not yet been unblinded and the pooled analysis (all patients combined) reported a 1- year overall survival of 79.4% [24]. Chemoradiation has largely been abandoned by European practitioners, but the Radiation Therapy Oncology Group (RTOG) has recently opened an intergroup trial to address this important question. Also, traditional prognostic and predictive variables may be supplemented with genetic profiles to determine radiosensitivity, and detection of patients with subclinical metastatic disease [25, 26, 27, 28].
CONCLUSION
Numerous institutions currently employ a strategy of trimodality therapy with postoperative chemoradiotherapy and the literature is now replete with suggestions of favorable outcomes with this treatment approach [1, 2, 14, 15, 20, 22, 29, 30, 31, 32, 33]. However, definitive information is lacking and until randomized trials establish uniformly accepted standards, results such as those presented in this report can continue to help guide treatment decisions in the adjuvant setting and provide further evidence for the efficacy of adjuvant chemoradiation following resection of pancreatic cancers. The results of this study also underscore the importance of resection status, number of involved lymph nodes and patient age as prognostic characteristics and they may be considered stratification variables for future postpancreatectomy adjuvant therapy trials.
Abbreviations
ACOSOG: American College of Surgeons Oncology Group; AJCC: American Joint Committee on Cancer; RTOG: Radiation Therapy Oncology Group
Conflicts of interest
The authors have no potential conflicts of interest
References
- Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvantcombined radiation and chemotherapy following curative resection.Arch Surg 1985; 120:899-903.
- Whittington R, Bryer MP, Haller DG, et al. Adjuvant therapy ofresected adenocarcinoma of the pancreas. Int J RadiatOncolBiolPhys 1991; 21:1137-43.
- Neuhaus HR, S. Post, K. Gellert, K. Ridwelski, H. Schramm, C.Zuelke, J. et al. CONKO-001: Final results of the randomized,prospective, multicenter phase III trial of adjuvant chemotherapywith gemcitabine versus observation in patients with resectedpancreatic cancer. J ClinOncol 2008; 26:LBA4504.
- Oettle H, Post S, Neuhaus P, et al. Adjuvant chemotherapy withgemcitabine vs observation in patients undergoing curative-intentresection of pancreatic cancer: a randomized controlled trial. JAMA2007; 297:267-77.
- Neoptolemos JP, Stocken DD, Friess H, et al. A randomized trialof chemoradiotherapy and chemotherapy after resection of pancreaticcancer. N Engl J Med 2004; 350:1200-10.
- Cardenes H, Powell, M, et al. E4201: Randomized phase IIstudy of gemcitabine in combination with radiation therapy versusgemcitabine alone in patients with locally advanced, unresectable,pancreatic cancer (LAPC): Quality-of-life (QOL) analysis. J ClinOncol 2009; 27:4627.
- Abrams RA. Comment on 'adjuvant therapy in pancreaticcancer: a critical appraisal'. Drugs 2007; 67:2481-5.
- Abrams RA, Lillemoe KD, Piantadosi S. Continuing controversyover adjuvant therapy of pancreatic cancer. Lancet 2001; 358:1565-6.
- Choti MA. Adjuvant therapy for pancreatic cancer--the debatecontinues. N Engl J Med 2004; 350:1249-51.
- Garofalo MC, Regine WF, Tan MT. On statistical reanalysis, theEORTC trial is a positive trial for adjuvant chemoradiation inpancreatic cancer. Ann Surg 2006; 244:332-3.
- Koshy MC, Landry JC, Cavanaugh SX, et al. A challenge to thetherapeutic nihilism of ESPAC-1. Int J RadiatOncolBiolPhys 2005;61:965-6.
- Oettle H, Neuhaus P. Adjuvant therapy in pancreatic cancer: acritical appraisal. Drugs 2007; 67:2293-310.
- Chang DK, Johns AL, Merrett ND, et al. Margin clearance andoutcome in resected pancreatic cancer. J ClinOncol 2009; 27:2855-62.
- Corsini MM, Miller RC, Haddock MG, et al. Adjuvantradiotherapy and chemotherapy for pancreatic carcinoma: the MayoClinic experience (1975-2005). J ClinOncol 2008; 26:3511-6.
- Herman JM, Swartz MJ, Hsu CC, et al. Analysis of fluorouracilbasedadjuvant chemotherapy and radiation afterpancreaticoduodenectomy for ductal adenocarcinoma of thepancreas: results of a large, prospectively collected database at theJohns Hopkins Hospital. J ClinOncol 2008; 26:3503-10.
- Fortner JG, Klimstra DS, Senie RT, et al. Tumor size is theprimary prognosticator for pancreatic cancer after regionalpancreatectomy. Ann Surg 1996; 223:147-53.
- Geer RJ, Brennan MF. Prognostic indicators for survival afterresection of pancreatic adenocarcinoma. Am J Surg 1993; 165:68-72.
- Neoptolemos JP, Stocken DD, Dunn JA, et al. Influence ofresection margins on survival for patients with pancreatic cancertreated by adjuvant chemoradiation and/or chemotherapy in theESPAC-1 randomized controlled trial. Ann Surg 2001; 234:758-68.
- Wenger FA, Peter F, Zieren J, et al. Prognosis factors incarcinoma of the head of the pancreas. Dig Surg 2000; 17:29-35.
- Klinkenbijl JH, Jeekel J, Sahmoud T, et al. Adjuvantradiotherapy and 5-fluorouracil after curative resection of cancer ofthe pancreas and periampullary region: phase III trial of the EORTCgastrointestinal tract cancer cooperative group. Ann Surg 1999;230:776-82.
- Picozzi VJ, Traverso LW, O'Reilly EM, Greeno E, Martin RC,Wilfond LS, et al. Z05031: Report on a multicenter, phase II trial foradjuvant therapy of resected pancreatic cancer using cisplatin, 5- FU,and alpha-interferon. J ClinOncol 2008; 26:Abstract 4505.
- Picozzi VJ, Kozarek RA, Traverso LW. Interferon-basedadjuvant chemoradiation therapy after pancreaticoduodenectomy forpancreatic adenocarcinoma. Am J Surg 2003; 185:476-80.
- Wilson VC, Guo M, Hampshire M, O'Dwyer P, Sun W, DrebinJ, et al. aggressive supportive care improves outcomes in thecombined modality treatment of pancreatic and duodenal cancer. IntJ RadiatOncolBiolPhys 2008; 69:S278-9.
- Van Laethem J, Hammel P, Mornex F, Azria D, Van TienhovenG, Peeters M, et al. Adjuvant chemotherapy alone versuschemoradiation after curative resection for pancreatic cancer :feasibility results of a randomised EORTC/FFCD/GERCOR phaseII/III study (40013/22012/0304). J ClinOncol 2008; 26:Abstract4514.
- Berger AC, Garcia M Jr, Hoffman JP, et al. Postresection CA19-9 predicts overall survival in patients with pancreatic cancertreated with adjuvant chemoradiation: a prospective validation byRTOG 9704. J ClinOncol 2008; 26:5918-22.
- Boeck S, Schulz C, Stieber P, et al. Assessing prognosis inmetastatic pancreatic cancer by the serum tumor marker CA 19-9:pretreatment levels or kinetics during chemotherapy? Onkologie2007; 30:39-42.
- Boeck S, Stieber P, Holdenrieder S, et al. Prognostic andtherapeutic significance of carbohydrate antigen 19-9 as tumormarker in patients with pancreatic cancer. Oncology 2006; 70:255-64.
- Ferrone CR, Finkelstein DM, Thayer SP, et al. PerioperativeCA19-9 levels can predict stage and survival in patients withresectable pancreatic adenocarcinoma. J ClinOncol 2006; 24:2897-902.
- Further evidence of effective adjuvant combined radiation andchemotherapy following curative resection of pancreatic cancer.Gastrointestinal Tumor Study Group. Cancer 1987; 59:2006-10.
- Regine WF, Winter KA, Abrams RA, et al. Fluorouracil vsgemcitabine chemotherapy before and after fluorouracil-basedchemoradiation following resection of pancreatic adenocarcinoma: arandomized controlled trial. JAMA 2008; 299:1019-26.
- Sohn TA, Yeo CJ, Cameron JL, et al. Resected adenocarcinomaof the pancreas-616 patients: results, outcomes, and prognosticindicators. J GastrointestSurg 2000; 4:567-79.
- Whittington R, Neuberg D, Tester WJ, et al. Protractedintravenous fluorouracil infusion with radiation therapy in themanagement of localized pancreaticobiliary carcinoma: a phase IEastern Cooperative Oncology Group Trial. J ClinOncol 1995;13:227-32.
- Yeo CJ, Abrams RA, Grochow LB, et al.Pancreaticoduodenectomy for pancreatic adenocarcinoma:postoperative adjuvant chemoradiation improves survival. Aprospective, single-institution experience. Ann Surg 1997; 225:621-33.



