Image - (2017) Volume 1, Issue 2
Renal Cell Carcinoma with Gastric and Paratracheal Metastases
Rodrigues AN*, Pranavan G and Gananadha S
Department of General Surgery, The Canberra Hospital, 77 Yamba Drive, Garran, Australia
*Corresponding Author:
Rodrigues AN
Department of General Surgery
The Canberra Hospital, 77 Yamba Drive
Garran, ACT 2605, Australia
Tel: +61402902282
E-mail: Nicole.rodrigues@act.gov.au
Received date: May 05, 2017; Accepted date: May 06, 2017; Published date: May 08, 2017
Citation: Rodrigues AN, Pranavan G, Gananadha S. Renal Cell Carcinoma with Gastric and Paratracheal Metastases. J Clin Gastroenterol Hepatol 2017, 1:2. doi: 10.21767/2575-7733.10000i15
Abstract
Renal cell carcinoma (RCC) has been known metastasize to almost all organ systems [1], however gastric metastasis is rare, with 50 cases reported in the literature to date [2]. There are also few reports of Para-tracheal RCC metastases. Here we describe a case of a 73-year-old patient with disseminated metastatic renal cell carcinoma (RCC) with gastric metastasis and a large para-treacheal deposit resulting in tracheal invasion and compression.
Description
Renal cell carcinoma (RCC) has been known metastasize to almost all organ systems [1], however gastric metastasis is rare, with 50 cases reported in the literature to date [2]. There are also few reports of Para-tracheal RCC metastases. Here we describe a case of a 73-year-old patient with disseminated metastatic renal cell carcinoma (RCC) with gastric metastasis and a large para-treacheal deposit resulting in tracheal invasion and compression.
The RCC was initially resected in 2009 with a right partial nephrectomy, followed by a complete right nephrectomy in 2014 after tumour recurrence. He had stable disease on Pazopanib, however presented in August 2016 with melena, and was found to have a large polypoid lesion at the gastric greater curvature on gastroscopy (Figure 1). This was revealed to be an ulcerated metastatic RCC deposit on histopathology. He underwent a distal gastrectomy in September 2016 and was commenced on Sunitinib. PET-CT also showed a suspicious large left para-tracheal mass (Figures 2 and 3), and despite the chemotherapy, had grown on a subsequent CT in January 2017, with tracheal deviation and invasion causing haemoptysis and stridor. After multidisciplinary consultation, he decided for palliative treatment and died due to acute respiratory distress 5 days later.
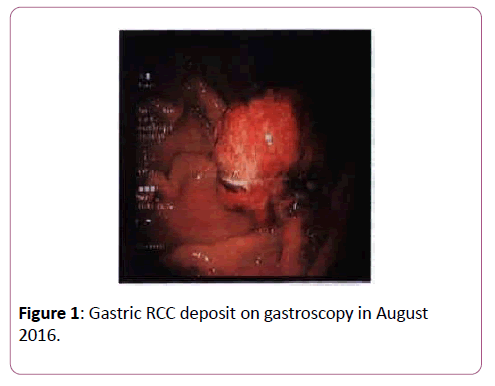
Figure 1:Gastric RCC deposit on gastroscopy in August 2016.
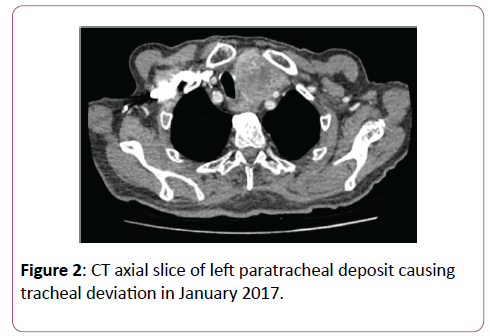
Figure 2:CT axial slice of left paratracheal deposit causing tracheal deviation in January 2017.
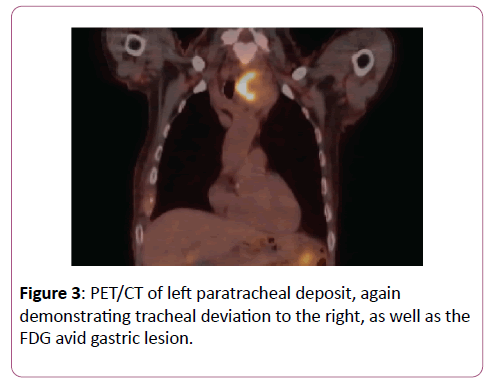
Figure 3:PET/CT of left paratracheal deposit, again demonstrating tracheal deviation to the right, as well as the FDG avid gastric lesion.
References
- Maldazys JD, DeKernion JB (1986) Prognostic factors in metastatic renal carcinoma. Journal of Urology136:376-379.
- Akay E, Kala M, Karaman H (2016) Gastric metastasis of renal cell carcinoma 20 years after radical nephrectomy. Turk J Urol 42:104-107.

