Keywords
Coping responses; Hispanic youth; Anxiety; Acculturative stress; Ambiguous situations
Introduction
Relationship of coping responses and anxiety symptoms in Hispanic youth
Anxiety is one of the most common experiences amongst youth; however, previous research is scarce regarding how youth cope with anxiety-provoking situations. The available research on child anxiety and coping has been predominately conducted with white, non-Hispanic children. The current study is an attempt to expand this literature to examine how Hispanic youth manage daily stressors and provide a better understanding of their experience of anxiety.
Child and adolescent anxiety
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), states that general anxiety includes symptoms of excessive worry that may be associated with restlessness, fatigue, difficulty concentrating, irritability, muscle tension, and sleep disturbances [1]. The literature suggests that there is a high prevalence of anxiety symptoms and disorders in the Hispanic youth population. One study with 281 youth explored anxiety in 12 to 19-year-old Hispanic youth and found that 29% met the threshold for clinical levels of anxiety [2]. Another study examined the difference in the rate of anxiety symptoms across three groups (i.e. Mexican, Hispanic, and European Americans) in a community sample. Results indicated that Mexicans and Hispanics reported more general worry symptoms than European American youth [3]. Another sample explored acculturative stress and anxiety in a sample of Hispanics, Caucasians, and African-American youth. The results showed that Hispanics experienced higher levels of acculturative stress and also demonstrated more anxiety symptoms that included social anxiety, physiological symptoms, and worrisome thoughts [4]. Overall, the literature suggests a high prevalence of anxiety symptoms in the Hispanic population, which highlights the need to explore the way Hispanic youth can manage these symptoms.
Cultural factors affecting anxiety in Hispanic youth
The current estimate of Hispanic youth under the age of 18 in the U.S. Hispanic population is approximately 33% [5]. A common experience faced by youth in this population is acculturative stress. Acculturative stress stems from challenges that individuals from Hispanic or other ethnic minority backgrounds face when attempting to adapt to lifestyles in the United States or dominant culture [6]. Some of the experiences Hispanic youth may struggle to adapt to include immigration, new language, new schools and academic system, peers, family, and social and economic factors [7]. Although studies have provided valuable data on the experiences of the growing Hispanic youth minority in the United States and their relationship to anxiety, the literature does not address the manner in which this population copes with acculturative stress.
Theoretical Considerations of Coping in Youth
Children encounter stressful situations in everyday life and coping plays a significant role in dealing with these experiences adaptively. Coping is defined as, “constantly changing cognitive and behavioral efforts to manage specific external and/or internal demands that are appraised as taxing or exceeding the resources of the person” [8] (p.141). Thus, coping is a process that changes according to the context and demands encountered in the environment. A number of models have been proposed to conceptualize and explain the process of coping. These models help capture the ways in which children deal with everyday stressors.
In particular, Lazarus and Folkman [8] developed the cognitive theory of coping. In this theory they propose that mental processes influence stress, and appraisal and coping act as a mediating process to reduce stress. Psychological stress is, “a particular relationship between the person and environment that is appraised by the person as taxing or exceeding his/her resources and endangering his or her well-being” [8] (p.19). Once an individual encounters stress or changes in the environment, they engage in a process of evaluating the situation’s level of threat. This process, which is vital to human survival, is referred to as cognitive appraisal. After cognitive appraisal of the situation is made, then coping takes place. Coping is the action in response to the individual’s appraisal in order to reduce stress.
Lazarus and Folkman proposed two general dimensions to conceptualize coping: problem-focused coping and emotion-focused coping. Problem-focused coping refers to how one views a situation, generates solutions, and decides on a course of action to solve the problem. For example, an adolescent with an upcoming speech may view the situation as anxiety-provoking, then generate several options on how to handle it such as, write the speech the morning it is due, practicing several times, or pretending to be sick the day of the speech. Then, the adolescent would choose a solution. Emotion-focused coping, on the other hand, is directed at efforts that are put forth to decrease emotional distress and no direct action is initiated at solving the problem. For example, a child might start crying after getting a bad grade from the teacher. In other words, the response serves to express the emotion that was triggered by the event. This two-dimensional model emphasized the assessment of the specific functions of coping. Meaning that, the model looks at each coping response and the purpose the response serves for the individual. Although the framework was originally used on adult populations, other researchers have effectively applied it to children. For example, Compas, Malcarne, and Fondacaro [9] coded 130 responses provided by young adolescents on a coping questionnaire by deciding if the response was emotion-focused or problem-focused coping. The results from the study showed that 6th-8th grade students increased the use of emotion-focused coping at each grade level and problem-focused remained consistent. The increase in emotion-focused coping could be explained by these strategies becoming more fully developed as youths learn to cope with social experiences and environmental stressors, which occur during the natural developmental process. This study provided evidence that Lazarus and Folkman’s [8] model could be useful with younger age groups.
Another model that has received support in the coping literature conceptualizes coping as approach or avoidant responses [10]. Approach coping, which is similar to problem-focused coping, “reflects active cognitive and behavioral efforts to define and understand the situation and to resolve or master a stressor by seeking guidance and engaging in problem-solving activity” [11] (p.36). On the other hand, avoidant coping refers to efforts that are used to avoid feeling or thinking about the stressful situation or get away from the threat. Compas et al. [12] concluded in their review of the literature that problem-focused, emotion-focused, approach, and avoidant coping are widely accepted approaches to categorize children’s coping. However, later reviews have suggested a lack of consensus on coping models and have yielded approximately 400 different categories, which have been used to examine children’s coping [13]. Given that each model proposes different constructs, there has been a great amount of confusion amongst the coping literature. In general, both two-dimensional models, problem-focused coping versus emotion-focused coping as well as approach coping versus avoidant coping, have been widely accepted in the coping literature, and continue to be used in empirical research examining children’s coping responses. In this research study, these two-dimensional models will be considered for evaluating youth’s coping in a minority sample.
Coping and anxiety
Research examining the relationship between coping and anxiety has been conducted in multiple settings, including medical settings, community samples, and psychiatric populations in a variety of countries. Coping in youth has been evaluated widely within medical settings, given that medical conditions or procedures elicit anxiety in children [14,15]. In a recent study, Compas et al. [16] examined how 153 children from the ages of 5 to 17 years old coped with cancer using the Responses to Stress Questionnaire-Pediatric Cancer Version. The results indicated that disengagement coping (e.g., avoidance, denial, wishful thinking) was related to symptoms of anxiety. The study provided evidence that avoidant coping is associated with anxiety; however, the results may not be generalizable to all children given the specific nature of the stress encountered by the children in the study.
Additional studies have examined the relationship between general negative life stressors, coping, and anxiety. One study conducted with 9 to 11-year-old children assessed coping strategies after a negative life event using a self-report coping questionnaire. The authors reported that 131 anxiety-disordered children who had been exposed to negative life events (i.e. expelled from school, committed a crime, family substance abuse, etc.) utilized more maladaptive (e.g., rumination, self-blame, catastrophizing, and acceptance) coping responses when compared to 452 nonanxious children [17]. Another study, which examined coping in an ethnically diverse sample, including African-American and Caucasian children, found that experiencing negative life events was significantly associated to anxiety [18]. In this study, African- American youth reported having more negative life events than Caucasian children. In addition, having experienced more negative life events was associated with more passive coping (i.e., avoidant coping). This study suggests that minority youth may be at risk for maladaptive coping and anxiety given that they tend to experience more negative life stress.
In addition to avoidant coping, support-seeking strategies have been associated with anxiety in children. One study with 270 children aged 8 to 11 with social anxiety demonstrated a positive association between internalizing, problem-solving, distraction, and seeking support coping [19]. Similarly, Vierhaus and Lohaus [20] conducted a longitudinal study that followed children for approximately 3 years. They found that support seeking coping strategies had significant direct paths to anxiety. Additionally, another study examined coping and coping efficacy, which refers to people’s evaluation of their ability to cope with stressors effectively [21]. They found that both avoidance and support seeking coping strategies were significantly associated with anxiety, whereas coping efficacy is negatively related to anxiety symptoms. Although these studies were conducted with a community sample, an important limitation is that the studies were not conducted in the United States. Thus, it is still unclear how children from the U.S. cope with everyday stressors, as well as what type of coping responses are related to anxiety in this population.
The role of situational and emotional factors in youth coping
The coping literature has also focused on situational and emotional factors that may influence coping responses. A study conducted with 8 to 13-year-old youth (n=1,123) who completed a German Coping Questionnaire found that developmental changes existed in the way children cope with different situations [22]. In particular, emotion-focused coping strategies (minimization and distraction/recreation) decreased in adolescence, whereas problem-focused strategies (situational control, positive self-instructions, and social support) were stable throughout early and middle adolescence. Examining situation-specific coping strategies showed that both children and adolescents used situational control, passive avoidance, rumination, and aggression when dealing with interpersonal stressors. When encountering academic stressors, they used more support seeking strategies. Situation-specific coping is helpful for explaining differences in coping strategies when dealing with internal versus external stressors; however, understanding the relationship of situation-specific coping strategies with anxiety symptoms was not addressed in this study. Therefore, a need exists to investigate the relationship between situation-specific coping and anxiety symptoms in children.
Another investigation examined whether emotion-eliciting situations influenced coping responses in youth. Vierhaus & Lohaus [20] investigated children’s coping responses to 4 emotion-specific scenarios (i.e., anger or anxiety) in a sample of 432 children. An example of an anxiety-evoking situation included, “The morning before taking a hard test you are sitting alone at the breakfast table. You feel uneasy at the thought of the test ahead and you lost your appetite.” On the other hand, an anger-evoking situation example included, “There are specific areas in which you are dissatisfied with your personal competencies. You have a desire to improve upon these competencies.” The children were asked if they would or would not use any of the 15 coping items that were listed, and if so, the child picked a response. The results indicated that in response to the anxiety-evoking scenario, children chose a coping pattern that was not directly goal-oriented, but focused on palliative, avoidant, and social seeking support coping, whereas the anger-evoking scenario was associated with externalizing emotional coping [20].
In another recent study, ambiguous situations (two situations related to anxiety, two situations about social phobia, and two situations related to specific phobia) were used to examine the relationship between cognitive variables, coping, and anxiety in a sample of 118 children, ages 7-13 [23]. Respondents’ coping responses were assessed by asking them to report their level of concern in response to the situation, to generate and explain proposed solutions, and decide on the similarity between a list of possible cognitions and their own thoughts. Additional measures regarding cognitive errors, threat-related interpretation bias, and anxiety-related control were used to identify low and high vulnerability groups. The results indicated that youth who comprised the high cognitive vulnerability group displayed more anxiety symptoms, emotional problems, and reported significantly higher use of avoidant strategies than children from the low cognitive vulnerability group.
In summary, the findings from previous research support that certain coping strategies, including avoidant, seeking support, and disengagement coping are associated with anxiety symptoms in children. A main limitation of most of the studies presented is that the findings were based on self-report questionnaires to assess for coping responses. In a review of the literature, Compas et al. [12] also found that the majority of studies used self-report questionnaires to capture coping responses of children. The limitation of the close-ended approach to collecting children’s coping responses is that it may not actually correspond to the way children respond or cope in a real-life situation. It provides a more limited perspective of coping than if children were asked to respond to different scenarios in an open-ended fashion. However, Compas and colleagues [12] also suggested that the open-ended scenarios tend to be unrealistic. Thus, there is room for improvement in the current measurement of coping strategies. Additionally, the recent literature that focuses on coping and anxiety in children has been conducted in foreign countries, which limits generalizability to children within the United States. Thus, future research is needed to determine how ethnically diverse youth in the U.S. cope with every day experiences, which may involve a high number of stressful situations, as well as how these two variables interact to lead to anxiety.
With the aim to expand research on the relationship between coping and anxiety symptoms in Hispanic children, the current study focused on the theoretical framework which categorizes coping responses into the broad categories of problem- versus emotion-focused [8], as well as approach versus avoidant responses. Specific coping strategies empirically developed by Ayers [24] within each broad category were used to guide this research study with a sample of diverse middle school children. This study used ambiguous scenarios for children to answer how they would respond to the situations. First, the study examined the prevalence of endorsement of each coping category based on contextual and situational characteristics. Second, the relationship of each coping response with anxiety symptoms was examined. The following hypotheses were proposed: 1) Emotion-focused strategies will be related to anxiety symptoms, such that youth with higher anxiety symptoms will utilize more emotion-focused strategies than youth with low anxiety symptoms; 2) The use of problem-solving strategies will not be associated with anxiety symptoms, such that youth with low anxiety will utilize more problem-focused strategies than youth with high anxiety symptoms; 3) Maladaptive coping strategies will be associated with anxiety symptoms, such that youth with high anxiety will utilize more maladaptive strategies than youth with low anxiety symptoms. Finally, the interactions between coping responses and acculturative stress and their relationship to anxiety was explored in this Hispanic sample of youth.
Methods
Participants
Participants included 288 middle school students ranging in age from 10 to 16 years old (mean age = 12.17, SD = 1.03). The sample had a distribution of 64.6% female and 35.4% male. Nearly all (95.1%) participants identified as Hispanic. The majority of the participants lived in low-income households (60.7 % below $39,000 per year), with 14.9% of households reporting an income between $40,000 and $54,999, and 15.4% over $55,000 per year. The most common language spoken at home was Spanish (64.6%), though the majority of participants reported that they were born in the United States (60.4%).
Procedure
This study was approved by the Institutional Review Board of Nova Southeastern University and Miami-Dade County Schools. The current study used a secondary dataset that was collected in the 2014-2015 school year. A de-identified data set containing the demographic information and the variables of interest were provided to the principal investigator. Prior to the data analyses, data coding of responses to three situations was conducted. This study’s advisor met with two independent coders that included the principal investigator of the study and an independent research assistant in order to train them on the coding system. Using a manual adapted from Ayers’s [24] work, coders learned the operational definitions for each coping category and coded responses given to each ambiguous situation. Details of the coding system are included below. Over a month and half-time period there were three different occasions during which coders coded cases independently. In order to assess reliability, both researchers coded 58% of the cases and the full research team including the two researchers and the study advisor discussed discrepancies. Inter-rater reliability of the coding was determined to be acceptable (kappa =0.67).
Coding system
The coding system derived from Ayer’s [24] coping research consisted of coping categories conceptualized from Lazarus and Folkman’s model, along with Billings and Moos’ model of coping. The present study’s coding system contained 16 coping categories divided into three broad categories. In the first broad category, problem-focused coping strategies involved direct attempts to solve or deal with the problem by implementing a solution and included direct problem-solving, redirection of attention to present-moment, seeking support problem-focused, cognitive decision making, and cognitive restructuring. The second broad category involved emotion-focused coping strategies, which deal with the problem by regulating affect elicited by the situation. Emotion-focused coping strategies included affect regulation, seeking support emotion-focused, expressing feelings, distracting cognitions, and resigned acceptance. The final category was maladaptive coping responses, which included strategies that are inappropriate attempts to deal with the situation or that do not deal with the problem in a constructive manner including, externalizing behavior, worrying or catastrophizing, behavioral avoidance, cognitive avoidance, and lack of problem-solving. Although cognitive avoidance and behavioral avoidance were originally included in the emotion-focused coping category, based on research indicating that these are inappropriate attempts to deal with a situation [21], they were moved into the maladaptive coping category.
Measures
Demographic information: A parent report questionnaire assessed the child’s age, race, and SES. Information on SES acquired yearly income in households, parental education, and occupation. Language spoken in the home was also assessed.
Anxiety: The Revised Children’s Anxiety and Depression Scale [25] includes 47-items to assess children’s report of symptoms of anxiety and depression. Participants rated how often they experience each symptom on a 4-point Likert scale (i.e., never, sometimes, often, always) scores can be computed for subscales for symptoms of depression, panic, obsessive compulsive, generalized anxiety, separation anxiety, and social anxiety were computed. A total anxiety score, which is created by summing the subscales of anxiety, was used in this study. Chorpita et al. [25] showed good reliability and internal consistency (ranged from α = 0.65-0.82) in a sample of 246 children and adolescents aged 8-18 years.
Coping: A short version of the Children’s Opinions of Everyday Life Events-Revised [26] was used to measure children’s coping in response to three ambiguous hypothetical situations of common everyday occurrences. Each ambiguous situation described a common scenario involving a peer situation (i.e., birthday party invitation), a school situation (i.e., teacher calling out a student), and personal harm in the home setting (i.e., noise in the house) to assess children's coping responses. Coping responses were evaluated by asking the child to list what he or she would actually do to deal with the situation. Responses were categorized as problem-focused, emotion-focused, and maladaptive responses using the coding system described before. Suarez-Morales & Bell [26] provided internal consistency coefficients for the COELE-R that ranged from 0.80-0.71.
Acculturative stress: Acculturative stress was measured using the Acculturative Stress Inventory for Children [27]. The ASIC is a 12-item questionnaire composed of two factors. The first factor includes 8 items that assess perceived discrimination and the second factor with 4 items measure immigration-related experiences. Participants were asked to rate how much they have been affected by acculturation-related stressors on a Likert scale with 6 ratings: 0=doesn’t apply, 1=doesn’t bother me much to 5=bothers me a lot. Suarez-Morales and colleagues [27] found adequate reliability for the total scale score (α =0.82), which was the score used in the present study.
Data analysis
Data was analyzed using the latest version of Statistical Package for Social Science (SPSS) software. Descriptive statistics including the mean scores and standard deviations were computed for continuous variables, including total anxiety and acculturative stress scores. A Pearson-moment correlation was calculated for these variables. A frequency score was computed for the subcoping categories, representing the percentage of children that endorsed each coping strategy across the three scenarios (Table 1). Next, the sub-categories were combined into the three broad categories, emotion-focused, problem-focused, and maladaptive, and a frequency score was obtained for each situation and summarized in Table 1.
| COELE-R Situation 1 |
COELE-R Situation 2 |
COELE-R Situation 3 |
| Category |
Frequency |
% |
Category |
Frequency |
% |
Category |
Frequency |
% |
| AR |
4 |
1.4 |
AR |
9 |
3.1 |
AR |
5 |
1.7 |
| BA |
11 |
3.8 |
BA |
1 |
0.3 |
BA |
5 |
1.7 |
| CA |
28 |
9.7 |
CA |
1 |
0.3 |
CA |
17 |
5.9 |
| CDM |
3 |
1.0 |
CDM |
7 |
2.4 |
CR |
4 |
1.4 |
| CR |
11 |
3.8 |
CR |
21 |
7.3 |
DA |
1 |
0.3 |
| DA |
3 |
1.0 |
DA |
1 |
0.3 |
DC |
2 |
0.7 |
| DC |
1 |
0.3 |
DC |
2 |
0.7 |
DPS |
99 |
34.4 |
| DPS |
141 |
49.0 |
DPS |
90 |
31.3 |
EB |
1 |
0.3 |
| EB |
14 |
4.9 |
EB |
6 |
2.1 |
EF |
2 |
0.7 |
| EF |
11 |
3.8 |
EF |
3 |
1.0 |
LPS |
10 |
3.5 |
| LPS |
10 |
3.5 |
LPS |
8 |
2.8 |
RA |
4 |
1.4 |
| RA |
42 |
14.6 |
RA |
88 |
30.6 |
RAA |
48 |
16.7 |
| RAA |
1 |
0.3 |
RAA |
1 |
0.3 |
SS-EF |
2 |
0.7 |
| SS-PF |
2 |
0.7 |
SS-EF |
1 |
0.3 |
SS-PF |
58 |
20.1 |
| W |
6 |
2.1 |
SS-PF |
11 |
3.8 |
W |
30 |
10.4 |
| |
|
|
W |
38 |
13.2 |
|
|
|
| PF EF MAL |
158 91 69 |
54.8 21.2 24.0 |
PF EF MAL |
130 104 54 |
45.1 36.1 18.8 |
PF EF MAL |
209 16 63 |
72.6 5.6 21.9 |
Note: AR = Affect Regulation; BA = Behavioral Avoidance; CA = Cognitive Avoidance; CDM = Cognitive Decision Making; CR= Cognitive Restructuring; DA = Distracting Action; DC = Distracting Cognition; DPS = Direct Problem Solving; EB = Externalizing Behavior; EF = Expressing Feeling; LPS = Lack of Problem Solving; RA = Resigned Acceptance; RAA = Redirection of Attention; SS-EF = Support Seeking Emotion-Focused; SS-PF = Support Seeking Problem-Focused; W = Worry; EF = Emotion-Focused; MAL = Maladaptive; PF = Problem-Focused
Table 1: Frequencies for coping subcategories and broad coping categories for each situation.
To examine the relationship between anxiety and coping, two groups were created using the mean of anxiety from the RCADS, with low anxiety defined as scores below the mean and high anxiety as scores above the mean. Using the two anxiety groups, a chi-square analysis for each situation was conducted to determine if the distribution of coping responses differed by group. Finally, hierarchical multiple regression analyses were performed for each situation to test whether coping responses (problem-focused, emotion-focused, maladaptive coping) predicted anxiety symptoms after controlling for acculturative stress, as well as to examine the interaction between coping and acculturative stress.
Results
The means and standard deviations for the main study measures were as follows for total anxiety scores (M=30.59, SD=18.84) and total acculturative stress scores (M=10.10, SD=8.09). The bivariate Pearson-moment correlation between acculturative stress and anxiety was statistically significant, r=0.51, p<0.01. As summarized in Table 1, coping responses were reviewed and found that the majority of the sample endorsed the sub-category, direct problem- solving, strategies involving actions that reduce the likelihood of the anticipated threat, ranging from 31.3% to 49.0% of responses for each situation. Also, resigned acceptance, doing nothing about the problem, was the second most endorsed coping response in situation 1 (14.6%) and situation 2 (30.6%). In situation 3, which focused on potential threat, seeking support problem-focused, going to find a parent, was the second most endorsed response. When reviewing the broad categories, problem-focused coping in situation 1 (54.9%), situation 2 (45.1%), and situation 3 (72.6%) was the most mentioned category. Maladaptive coping responses followed behind for situations 1 (24.0%) and 3 (21.9%), and emotion-focused in situation 2 (36.1%).
Three chi-square analyses were performed to determine if there were differences in coping for the high anxiety group and low anxiety group for each situation. The first analysis conducted using a social situation (situation 1), revealed a non-significant difference in the distribution of coping categories across the two anxiety groups, X2 (2) = 2.72, ns. Similarly, coping responses were not significantly different between the two anxiety groups in a school situation (situation 2), X2 (2) = 4.45, ns. The last chi-square analysis examined the relationship between coping and anxiety in a home environment situation (situation 3) and also revealed non-significant results, X2 (2) = 1.96, ns. Figures 1A-C depicts the distribution of each coping category for high and low anxiety groups per situation.
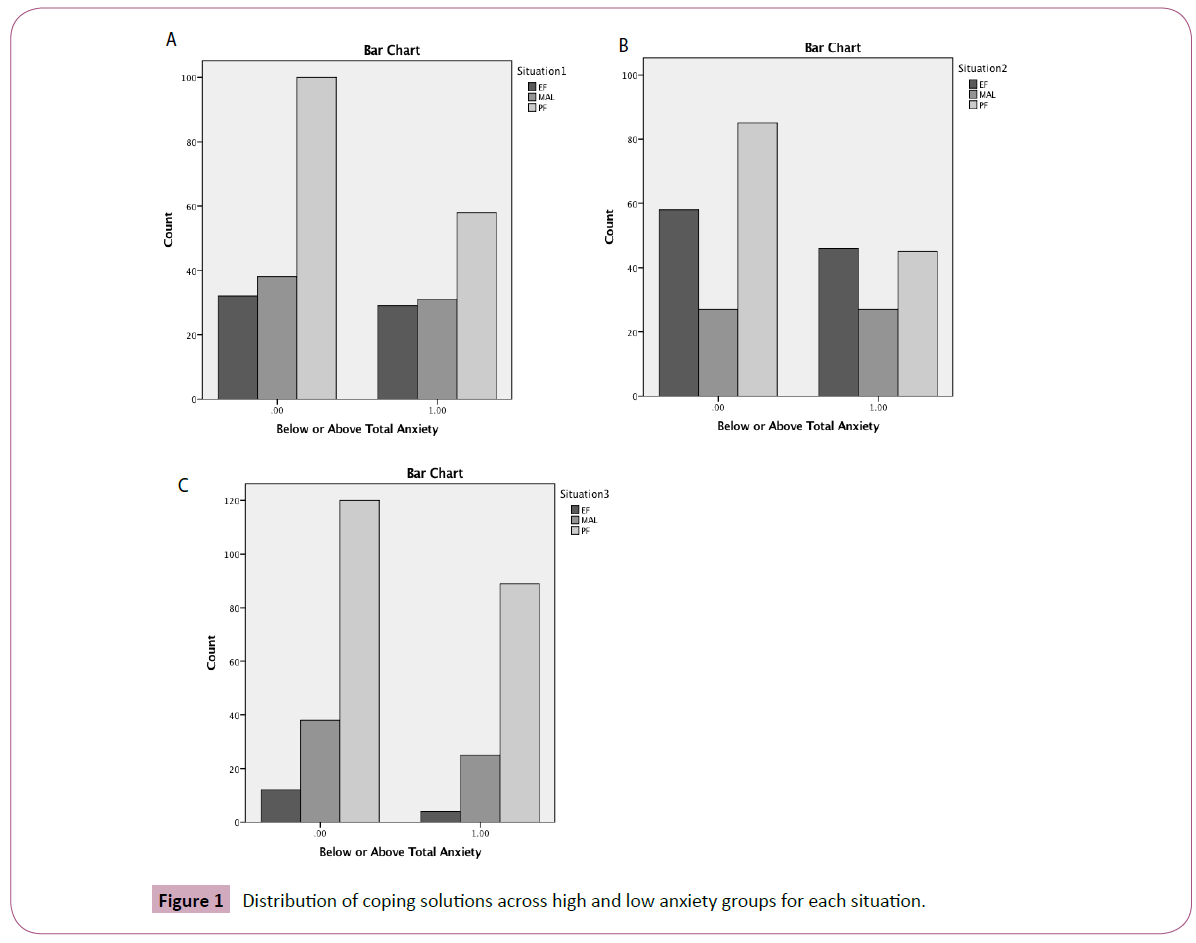
Figure 1: Distribution of coping solutions across high and low anxiety groups for each situation.
Next, three hierarchical regressions were conducted to determine whether acculturative stress and coping categories, and their interaction predicted total anxiety symptoms in each situation of the COELE-R. For all three regressions corresponding to each situation, acculturative stress and coping variables (problem-focused, emotion-focused, and maladaptive coping) were entered in the first step of the regression. In step 2, interactions between acculturative stress and emotion-focused and acculturative stress and maladaptive coping were entered. Table 2 presents findings for each model.
| |
Situation 1 |
Situation 2 |
Situation 3 |
| R2 |
0.353* |
0.344* |
0.343* |
| ASIC |
0.592 |
0.583 |
0.584 |
| EF |
0.027 |
|
-0.013 |
| PF |
-0.082 |
-0.023 |
-0.013 |
| MAL |
|
0.024 |
|
| R2Δ |
0.001 |
0.006 |
0.004 |
| EF x ASIC |
0.040 |
|
-0.037 |
| MAL x ASIC |
-0.021 |
0.025 |
0.089 |
| PF x ASIC |
|
0.148 |
|
| TOTAL R2 |
0.353* |
0.350* |
0.347* |
Note: *p < 0.01. ASIC = Acculturative Stress Scale for Children; EF = Emotion-Focused; PF = Problem-Focused; MAL = Maladaptive
Table 2: Summary of hierarchical regression analyses for acculturative stress and coping variables to predict anxiety (N=288).
For situation 1, Step 1 of the model was significant, F (3, 283) = 51.36, p<0.01, and was responsible for 35.3% of the variance in total anxiety score. Step 2 was also significant, F (5, 281) = 30.71, p<0.01, but the variance accounted for by the interaction terms did not significantly contribute to the overall model (R2 Δ = .001, p =0.84). When examining individual predictors, only acculturative stress was significantly associated with anxiety (β = 0.59, p<0.01). The coping variables and the interactions between the coping variables and acculturative stress were not significantly related to anxiety (β = -0.08-0.04, ns).
For situation 2, the model was significant at Step 1, F (3, 283) = 49.48, p<0.01, and explained 34.4% of the variance in total anxiety scores. Step 2 was also significant, F (5, 281) = 30.29, p<0.01, but the variance accounted for by the interaction terms did not significantly contribute to the overall model (R2Δ =0.006, p=0.27). When reviewing individual predictors, again only acculturative stress was significantly associated with anxiety (β = 0.58, p<0.01). Again, coping variables and the interactions between coping variables and acculturative stress were not significantly predictive of anxiety symptoms (β = -0.02-0.15, ns).
Last, for Situation 3, the model at Step 1 of the regression significantly predicted anxiety, F (3, 283) = 49.19, p<0.01. This step accounted for 34.3% of the variance in total anxiety scores. The model at Step 2 was also significant F (5, 281) = 29.83, p<0.01, but the variance accounted for by the interaction terms did not significantly contribute to the overall model (R2Δ = 0.004, p=0.43). When reviewing individual predictors, again only acculturative stress was a significant predictor (β = 0.58, p<0.01). Coping variables and the interactions between coping variables and acculturative stress were not significantly predictive of anxiety symptoms (β = -0.04-0.09, ns).
Discussion
The present study explored the relationships among coping strategies, acculturative stress, and anxiety symptoms in a sample of Hispanic youth. Prior to data analyses, youth’s responses to common everyday situations were examined by using two empirically supported theoretical models [8,10], as well as empirically derived coping strategies described in the coping literature [24]. The current study aimed to determine whether specific coping responses are related to anxiety symptoms in Hispanic youth. Contrary to previous findings [23,20], coping responses did not differ between groups or show a relationship to anxiety in this study. A possible explanation for the lack of findings is that the coping categories utilized to code the open-ended responses of the COELE-R are empirically validated with Caucasian populations and not with ethnic minority populations.
To our knowledge, no other study has examined coping with Hispanic populations, and perhaps the categories used in this study are not sensitive to the experiences or coping responses utilized by this population. Another methodological issue that may explain the null findings is that the COELE-R uses ambiguous situations with open-ended responses and most research that examine coping in youth rely on questionnaires. The open-ended response method was used in this study to discover how youth would actually cope in a situation, as opposed to being forced to pick from a limited list of coping responses; thus, allowing for a more realistic way of interpreting coping in everyday situations. With that being said, perhaps, ambiguous situations did not provide a clear indication to the youth of a need to cope with a stressful situation, which is a central tenet of the theory of coping [8]. This issue highlights an important caveat in the current body of literature regarding coping; namely that there is very limited research that has examined ambiguous situations with openended coping responses. Therefore, future research is needed to examine the validity and reliability of this measurement method to assess youth coping. In addition, potential significant relationships between coping and anxiety may have not been revealed in the current study due to cultural factors that have not been considered in the current theoretical models of coping. Thus, future research should aim to elucidate the cultural mechanisms of coping to develop a proper understanding of coping in diverse children.
Emotion-focused coping in relation to anxiety
While there is evidence that supports relationships between specific coping responses and anxiety in the literature, emotion-focused coping shows inconsistent findings. As mentioned earlier, emotion-focused coping are efforts put forth to decrease emotional distress that have no direct action at solving the problem. The first hypothesis of this study, stating that youth with higher levels of anxiety symptoms will use more emotionfocused coping strategies than youth with lower levels of anxiety symptoms, was not supported. However, one study conducted by Lewis and colleagues [18] showed that passive coping (i.e. avoidant coping, emotion-focused in nature) was not associated with anxiety in African American youth. This is interesting, given that the current study also examined coping in a minority population, in this case Hispanic youth; therefore, it is possible that the empirically supported coping models are not a one size fits all for diverse youth. Another explanation to the findings could be that other variables may have influenced coping strategies. For example, coping efficacy, which refers to one’s perception of whether a stressor is manageable or unmanageable, was a partial mediator between coping responses and anxiety symptoms in previous research [21]. Therefore, it is possible that a latent variable, such as coping efficacy, could have impacted the results. Exploration of potential mediators and moderators may be a next valuable step in research to understand the relationship between coping and anxiety.
Problem-focused coping in relation to anxiety
The second hypothesis stated that problem-solving strategies would not be associated with anxiety symptoms, such that youth with low anxiety will engage in more problem-focused coping than youth with high anxiety symptoms. Our results found no association between problem-focused coping and anxiety, as demonstrated by no differences in the use of this coping strategy between high and low anxious groups. Possibly, Hispanic youth cope in a similar way despite their symptoms of anxiety, as direct problem solving was the most endorsed sub-category for all situations. Furthermore, since youth in general used directed problem-focused solutions in this sample, the lack of findings may be an artifact of this sample being from the community, in which youth may not show clinical levels of anxiety. For instance, even when high and low anxiety groups were selected and evaluated in this sample, the high anxiety group was not high enough to meet the clinical threshold.
The literature on problem-focused coping and anxiety has also reported mixed findings. Lewis and colleagues [18] found a positive relationship of active coping (i.e. problem-focused coping) and anxiety in a community sample of African-American and Caucasian youth. These findings are inconsistent with most of the literature on childhood coping and anxiety [14,21]. In light of the mixed findings in the literature, it less surprising that the current study found no association between problem-focused coping and anxiety. These findings, however, highlight the need to continue to conduct researchers with ethnic minority samples to better understand the relationship between problem-focused coping and anxiety.
Maladaptive coping in relation to anxiety
To address the last hypothesis, the present study expected that maladaptive coping strategies will be associated with anxiety symptoms, such that youth with high anxiety will utilize more maladaptive strategies than youth with low anxiety symptoms. However, no differences in the use of maladaptive coping strategies were found between the groups in this sample. This finding is not consistent with previous literature [23] that found maladaptive coping strategies to have a relationship with anxiety symptoms. Again, the current study was not able to distinguish differences in coping responses between the high and low anxiety groups. As mentioned before, there may be multiple possible explanations for these findings, including the lack of evidence supporting the coping models for Hispanic youth or the use of a community sample, in which clinical levels of anxiety are not significantly manifested.
Acculturative stress influence on coping and anxiety
Although the hypotheses regarding coping and anxiety were not supported, it appears that acculturative stress played a significant role in this study. Acculturative stress is a relevant factor in the lives of Hispanic youth and is associated with symptoms of anxiety [2-4]. Consistent with previous literature, the current study found that acculturative stress significantly predicted symptoms of anxiety in Hispanic youth. However, when examined in the light of coping responses, acculturative stress was not found to interact with different coping responses to predict anxiety. Findings suggest that examining situations that elicit acculturative stress, rather than everyday general situations, may possibly provide a better understanding of how Hispanic youth cope. Therefore, future research should incorporate the use of more culturally-relevant situations to study the relationship between coping and anxiety in Hispanic samples.
Coping responses by situations
There are very few studies that examine the type of situation as it relates to coping and anxiety; however, there are no studies that use a Hispanic youth sample. Usually research combines coping responses across situations giving the research more power to detect differences. Given evidence suggesting that youth vary in their way they cope depending on the situation, this study examined each situation separately. It was found that both high and low anxious groups used similar coping strategies; however, the strategies do seem to vary by situation. The type of coping strategy used in each situation was examined using the distribution of each broad coping category for each situation. This question was not addressed directly in the present study, but it provides for more knowledge on the way Hispanic youth cope. In situation 1, youth were presented with how to cope during a social situation; the majority of responses the youth utilized were problem-focused. This suggests that youth were more likely to approach another peer in efforts to solve the problem. In situation 2, involving a teacher requesting that the child stays after class, youth utilized both problem-focused and emotion-focused coping. Interestingly, when an authority figure was present, coping responses became mixed. Some research with Hispanic samples has found that the impact of authority figure (i.e. teacher/parent) may influence coping responses, given that this population is known to rely heavily on family support as well as be highly compliant with authority figures [2]; thus, youth may feel like they have to resort to emotion-focused strategies to cope with a situation involving being called on by the teacher. With that being said, it’s not surprising that in situation 3, a potential threat within the home, resulted in the use of problem-focused coping, more specifically direct problem solving and support seeking strategies. The results found in this study with Hispanic youth remained consistent with literature on Hispanic family dynamics and coping responses.
Limitations of the Present Study
The results of the current study should be interpreted with caution due to several limitations. First, self-report measures were utilized in the study assessing anxiety symptoms and acculturative stress, which may be biased due to under-reporting. In the future, additional reports should be obtained from other informants, such as parents or teachers, to corroborate the child’s reports. Additionally, a methodological limitation may exist on the use of an appropriate assessment measure of coping with Hispanic youth given the lack of valid measures for measuring coping in this population. The current study attempted to use an open-ended approach to assess coping, but the categories used to judge the type of proposed responses may also be insensitive to the realities of ethnic minorities, in particular Hispanic youth. Therefore, it is still in question what measurement tools work best at assessing coping with Hispanic minority youth (i.e. Likert scale or open-ended responses). In addition, the lack of findings in the study may be attributed to using a sample from the community, where children do not exhibit clinical levels of anxiety. Lastly, this is the first known study examining Hispanic populations; therefore, there has been no replication or prior literature guiding research with this population.
Implications and Future Directions
The findings of the present investigation emphasize the importance of considering more targeted research on how Hispanic youth handle and manage stress. As demonstrated by the current study, coping responses may not be universal to all ethnic groups. Therefore, modifying coping models to consider cultural factors that may affect Hispanic youth and other ethnic minority groups could improve the knowledge of coping mechanisms and the current understanding of their relationship to anxiety symptoms.
Future studies should aim to examine coping responses in Hispanic youth to decipher the potential associations with anxiety symptoms. Currently, empirically supported coping models have been validated on predominately Caucasian populations; therefore, studies should focus on creating a coping model that is applicable to the Hispanic youth population. Also, there is a need to examine coping responses by situations that are often encountered by youth in the United States. Acknowledging different coping responses in context can provide professionals directions on clinical interventions with Hispanic youth. Understanding ethnic differences with regards to coping responses and their relationship to anxiety can inform culturally sensitive preventative efforts and interventions in order to aid this vulnerable ethnic minority population.
References
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders (5th Edn). Washington, DC: Author, p: 128.
- Potochnick SR, Perreira KM (2010) Depression and anxiety among first-generation immigrant Latino youth.J Nerv Ment Dis198: 470-477.
- Varela RE, Sanchez-Sosa J, Biggs BK, Luis TM (2008) Anxiety symptoms and fears in Hispanic and European American children: cross-cultural measurement equivalence. J Psychopathol Behav Assess30: 162.
- Suarez-Morales L, Lopez B (2009) The impact of acculturative stress and daily hassles on pre-adolescent psychological adjustment: examining anxiety symptoms.J Prim Prev 30: 335-349.
- https://www.census.gov/population/hispanic/data/2013.html
- Berry JW, Kim U, Minde T, Mok D (1987) Comparative studies of acculturative stress. Int Migr Rev 21: 491-511.
- Cervantes RC, Cordova D (2011) Life experiences of Hispanic adolescents: developmental and language considerations in acculturation stress.J Community Psychol 39: 336-352.
- Lazarus RS, Folkman S (1984) Stress, appraisal, and coping. New York: Springer, p: 456.
- Compas BE, Malcarne VL, Fondacaro KM (1988) Coping with stressful events in older children and young adolescents.J Consult Clin Psychol 56: 405-411.
- Billings AG, Moos RH (1981) The role of coping responses and social resources in attenuating the stress of life events. J Behav Med4:139-157.
- Ebata AT, Moos RH (1991) Coping and adjustment in distressed and healthy adolescents.J Appl Dev Psychol 12: 33-54.
- Compas BE, Connor-Smith J, Saltzman H, Thomsen AH, Wadsworth ME (2001) Coping with stress during childhood and adolescence: problems, progress, and potential in theory and research.Psychol Bull 127: 87-127.
- Skinner EA, Edge K, Altman J, Sherwood H (2003) Searching for the structure of coping: a review and critique of category systems for classifying ways of coping.Psychol Bull 129: 216-269.
- Compas BE, Boyer MC, Stanger C, Colletti RB, Thomsen AH, et al. (2006) Latent variable analysis of coping, anxiety/depression, and somatic symptoms in adolescents with chronic pain. J Consult Clin Psychol 74: 1132-1142.
- Miller SM, Roussi P, Caputo GC, Kruus L (1995) Patterns of children's coping with an aversive dental treatment.Health Psychol 14: 236-246.
- Compas BE, Desjardins L, Vannatta K, Young-Saleme T, Rodriguez EM, et al. (2014) Children and adolescents coping with cancer: self- and parent reports of coping and anxiety/depression.Health Psychol 33: 853-861.
- Legerstee JS, Garnefski N, Jellesma FC, Verhulst FC, Utens EM (2010) Cognitive coping and childhood anxiety disorders. Eur Child Adolesc Psychiatry 19: 143-150.
- Lewis KM, Byrd DA, Ollendick TH (2012) Anxiety symptoms in African-American and Caucasian youth: relations to negative life events, social support, and coping.J Anxiety Disord 26: 32-39.
- Wright M, Banerjee R, Hoek W, Rieffe C, Novin S (2010) Depression and social anxiety in children: differential links with coping strategies.J Abnorm Child Psychol 38: 405-419.
- Vierhaus M, Lohaus A (2009) Children's perception of relations between anger or anxiety and coping: continuity and discontinuity of relational structures.Soc Dev 18: 747-763.
- Thorne KJ, Andrews JJW, Nordstokke D (2013) Relations among children's coping strategies and anxiety: the mediating role of coping efficacy.J Gen Psychol 140: 204-223.
- Hampel P, Petermann F (2005) Age and gender effects on coping in children and adolescents. J Youth Adolesc 34: 73-83.
- Marques T, Pereira AIF, Barros L, Muris P (2013) Cognitive vulnerability profiles of highly anxious and non-anxious children.Child Psychiatry Hum Dev 44: 777-785.
- Ayers TS, Sandler IN, West SG, Roosa MW (1996) A dispositional and situational assessment of children's coping: testing alternative models of coping.J Pers 64: 923-958.
- Chorpita BF, Yim L, Moffitt C, Umemoto LA, Francis SE (2000) Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale.Behav Res Ther 38: 835-855.
- Suarez-Morales L, Bell D (2006) Relation of childhood worry to information-processing factors in an ethnically diverse community sample.J Clin Child Adolesc Psychol 35: 136-147.
- Suarez-Morales L, Dillon FR, Szapocznik J (2007) Validation of the acculturative stress inventory for children.Cultur Divers Ethnic Minor Psychol 13: 216-224.

