Keywords
Glucagonoma; Neuroendocrine Tumors; Optic Neuropathy, Ischemic; Paraneoplastic Syndromes
Abbreviations
CT computed tomography; PON paraneoplastic optic neuropathy
INTRODUCTION
Pancreatic neuroendocrine tumours (PNETs) account for 5% of pancreatic tumours [1] and are malignant in 50-88% of cases [2]. PNETs can be functioning, i.e., with clinical manifestations due to hormonal hypersecretion, in about 30% of cases. The most frequent functioning PNETs are those related to hypersecretion of insulin and gastrin. Rarely, PNETs may be associated with VIPoma and glucagonoma symptoms [2].
The annual incidence of glucagonomas is about 0.01-0.1 cases/million [2]. This tumour develops at the expense of Langerhans alpha-cell islets, and is commonly unique and large-sized. Its clinical manifestations include necrolytic migratory erythema (NME), weight loss, diabetes mellitus, diarrhoea, anaemia, deep-vein thrombosis, onycholysis, hypolipidemia, hyperprotidemia, and dementia. Ophthalmological manifestations due to glucagonoma have very rarely been described.
The purpose of this report was to describe the case of a patient in whom a glucagonoma was discovered during the workup of a visual loss with bilateral scotoma that regressed after tumour resection, and to comprehensively review literature on glucagonoma-associated ophthalmological manifestations, with focus on their diagnosis and management.
CASE REPORT
A Sixty-five-year-old man, with past history of psoriasis, ischemic cardiopathy and familial history of colonic adenoma, consulted in 2011 because of progressive bilateral visual loss. The latter had begun on the left eye in March 2011 and became bilateral in November 2011. Initial ophthalmological examination in November 2011 showed visual acuity (VA) of 20/50 and 20/40, in the right (RE) and left eye (LE), respectively (Figure 1). Fluorescein angiogram was normal. The anterior segment and ocular tonus were also unremarkable. Ophthalmoscopy showed bilateral optic atrophy. Visual field examination revealed bilateral caeco-central scotoma (Figure 2). Visual evoked potentials showed no response to pattern stimulation. On optical coherence tomography, the retinal nerve fiber layer (RNFL) was reduced in the right nasal and left superior area, in both eyes the mean RNFL thickness was reduced. Electro-retinography was normal in both eyes. Overall, this ophthalmological examination was suggestive of central optic neuropathy. Metabolic deficiencies and toxic aetiologies were excluded (vitamins A, B1, B9, B12, zinc, protein and iron levels were normal). The cerebral magnetic-resonance imaging (MRI) was normal. In May 2011, concurrently with ophthalmological symptoms, the patient developed a type-2 diabetes mellitus and diarrhoea. In 18 months, the patient had an 11kg weight loss. Gastroscopy and colonoscopy were performed in October 2012 and were unremarkable. At that time, plasma glucagon level was 204 pmol/L (N: 17-51), chromogranin A 51ng/mL (N: 27-94), gastrin 14.1 pg/mL (N: 13-115), and VIP< 20 (N<60) (Figure 1). An abdominal computed tomography (CT) scan showed a hypervascularized, necrotic and calcified mass, localized in the isthmus and body of the pancreas, measuring 75 mm in diameter. In November 2012, itchy circular erythematous-squamous dermal lesions appeared on the back, with peripheral erythematous border, evoking NME (Figure 3). Glucagon-hypersecreting PNET was then evoked. Pathological examination of endoscopic-ultrasound-guided tumour biopsies showed a grade 2 well-differentiated PNET (proliferative index Ki-67 was 5%). No distant lesion was seen on MRI and chest CT-scan. Somatostatin-receptor scintigraphy showed intense PNET uptake with no evidence of dissemination. Octreotide LP 20 mg every 28 days was then given with symptomatic intent, yielding no significant efficacy on cutaneous lesions, asthenia, diabetes and ophthalmological disease. A pancreaticoduodenectomy (whipple procedure) was performed in February 2013. Pathological analysis showed an 80 mm well-differentiated NET with metastatic lymph-nodes and safe margins, grade 2 (proliferative index Ki67: 5%, mitotic index: 2 per 10 high power fields). Postoperative course was unremarkable. One month after the surgical procedure, the patient had regained 7kg, NME lesions and diarrhoea had resolved, and diabetes was well controlled with low insulin doses. On October 2013, glucagon plasma level normalized at 22pmol/L (Figure 1). Pre-operative ophthalmological evolution was marked by scotoma persistence, and a progressive worsening of VA (RE 20/200, LE 20/400 in November 2012). After surgery, VA improved rapidly: RE 20/25 in August 2013, 20/20 in October 2013 and 20/20 in March 2014; and LE 20/40 in August 2013, 20/40 in October 2013 and 20/40 in March 2014 (Figure 1). Postoperative ophthalmoscopy showed a decrease of the optic atrophy. Visual evoked potentials showed normal response and visual field examination became normal with scotoma disappearance (Figure 2). One year after the surgical procedure, VA had almost normalized in the right eye and remained stable in the left eye (RE 20/20, LE 20/40) (Figure 1). Regarding PNET, imaging follow-up included a yearly morphological examination by MRI or CT-scan. Eighteen months following surgery, the patient was alive, in good general health, without sign of tumour recurrence and no functioning sign.
Figure 1. Evolution of the plasma levels of chromogranin A and glucagon (left), and visual acuity (right), between before and after pancreatic surgery
(arrow), in a patient with glucagonoma-associated paraneoplastic optic neuropathy.
Figure 2. Automated kinetic perimetry : bilateral centrocaecal scotoma (2011), Normal visual field in both eyes (2014).
Figure 3. Typical NME lesions.
DISCUSSION
We described herein an exceptional case of glucagonoma-associated ophthalmological severe manifestations, with dramatic total and sustained relief after curative pancreatic surgery. In the literature, glucagonoma-associated ophthalmological manifestations have been inconstantly reported, with a very low incidence [3, 4, 5, 6, 7]. Nevertheless, glucagonomas are very rare PNETs and it is very hard to determine the precise incidence of their ophthalmological manifestations. The patient’s ophthalmological manifestations (subacute, bilateral, painless and progressive visual acuity loss with paracentral scotomas) were suggestive of optic nerve paraneoplastic syndrome, even more as it has significantly regressed after surgical resection of the pancreatic glucagonoma.
Paraneoplastic optic neuropathy (PON) is often part of complex paraneoplastic syndromes, with cognitive troubles, sensitive neuropathy or myelopathy. PON can also be isolated. PON has been reported to be associated with small cell lung cancer and rarely with B-cell lymphoma, uterine sarcoma, breast, prostate, nasopharyngeal, bronchial, papillary thyroid, non-small cell lung, and renal cell carcinoma [8].
Patients classically present with subacute, bilateral, painless, progressive vision loss. The optic nerve head may appear normal, oedematous, or atrophic. Visual fields may show paracentral scotomas, altitudinal defects and/or peripheral constriction. Bitemporal hemianopsia has also been described in patients in whom PON primarily affected the optic chiasm. T2-weighted MRI examination classically reveals hyper-intense signals in brain parenchyma, or optic nerves or spinal cord abnormalities, or may be normal.
To our knowledge, only 4 cases of glucagonoma-associated visual manifestations have been specifically reported to date (Table 1). The diagnosis of PON could not be confirmed for those cases, but their clinical presentation (i.e., VA loss, optic nerve atrophy and/or scotoma) was highly suggestive of optic neuropathy. The ophthalmological symptoms regressed progressively in all cases, as well as the other clinical symptoms of glucagonomas with the glucagonoma treatment (i.e., surgical removal, chemotherapy or somatostatin analogs) (Table 1).
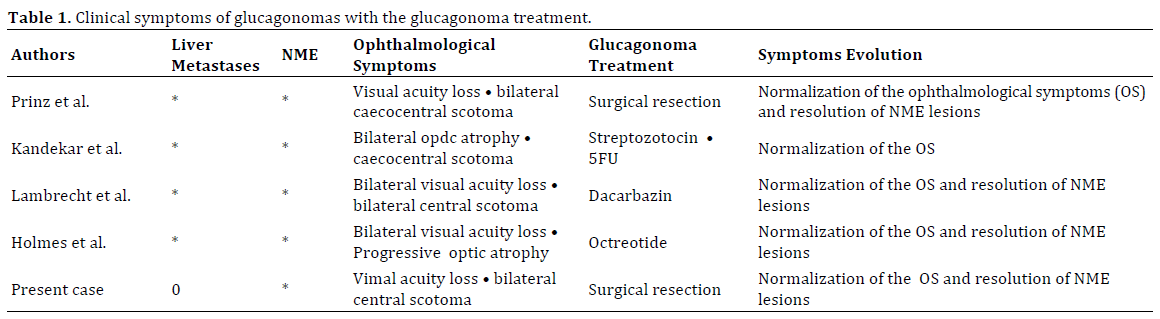
Hence, these optic neuropathies were very likely to be glucagonoma-associated PON. In a review reporting 21 patients with glucagonoma tumour, 3 of them had visual difficulties (14%) [7], that regressed after treatment of the glucagonoma. Moreover, two cases of non-functioning PNET have also been reported to be associated with visual manifestations [9, 10]. Ophthalmological symptoms regressed under somatostatin analogs in one case [9], whereas it did not totally resolve after surgery in the other case [10].
Two kinds of serum antibodies can be present in paraneoplastic optic manifestations: anti-CAR IgG in paraneoplastic optic retinopathy and anti-CRMP5 IgG in paraneoplastic optic neuropathy [8, 11, 12]. Collapsin response-mediating proteins (CRMP) are believed to regulate growth guidance cues during neurogenesis. Specifically, the CRMP-5 subtype is found in normal adult retina, optic nerve, and central and peripheral neurons. However, its physiological functions are still unknown [11, 12]. Besides, anti-CRMP5 serum antibodies, also called anti-CV2, are frequently found in the serum of patients affected with paraneoplastic neurological syndromes in general, and the ones affecting the optic nerve in particular [8]. Described as binding to neuronal (but not tumor) cytoplasm [13], and as oligodendrocyte-specific (anti-CV2) [14], each has been reported with paraneoplastic optic neuropathy. In our case, no anti-CRMP-5 antibody was found in the resected post-operative specimen. No patient’s serum was available.
Other aetiologies of optic neuropathy such as vascular pathologies (as arteriosclerosis or inflammatory diseases), nutritional and vitamin deficiencies or toxic causes were searched. The comprehensive evaluation of this case provided no other evidence of other causes. No auto-immune pathology was found. Electrolytes levels were normal (copper, magnesium, selenium, zinc). Vitamin A, E, and C levels were at the lower end of the normal range but not lower enough to explain the symptoms. Vitamin B9, B12, C, D and K1 levels were normal. Protein and albumin levels were normal at the beginning of the case.
In conclusion, this very rare case showed that PON can be associated with glucagonoma syndrome. PON could be an early symptom of the glucagonoma syndrome, as it can appear before NME. Patricians should be aware of the possible association of glucagonomas with PON and its regression after tumour resection.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Conflict of Interest
All authors declare no conflict of interest potentially interfering with this work.
References
- Koh YX, Chok AY, Zheng HL, Tan CS, Goh BK. A systematic review and meta-analysis of the clinicopathologic characteristics of cystic versus solid pancreatic neuroendocrine neoplasms. Surgery 2014; 156:83-96.e2. [PMID: 24878455]
- Jensen RT, Cadiot G, Brandi ML, de Herder WW, Kaltsas G, Komminoth P, Scoazec JY, et al. ENETS Consensus Guidelines for the management of patients with digestive neuroendocrine neoplasms: functional pancreatic endocrine tumor syndromes. Neuroendocrinology 2012; 95:98-119. [PMID: 22261919]
- Khandekar JD, Oyer D, Miller HJ, Vick NA. Neurologic involvement in glucagonoma syndrome: response to combination chemotherapy with 5-fluorouracil and streptozotocin. Cancer 1979; 44:2014-6. [PMID: 228832]
- Prinz RA, Badrinath K, Banerji M, Sparagana M, Dorsch TR, Lawrence AM. Operative and chemotherapeutic management of malignant glucagon-producing tumors. Surgery 1981; 90:713–719. [PMID: 6269242]
- Lambrecht ER, van der Loos TL, van der Eerden AH. Retrobulbar neuritis as the first sign of the glucagonoma syndrome. Int Ophthalmol 1987; 11 :13–15. [PMID: 2826358]
- Holmes A, Kilpatrick C, Proietto J, Green MD. Reversal of a neurologic paraneoplastic syndrome with octreotide (Sandostatin) in a patient with glucagonoma. Am J Med 1991; 91:434–436. [PMID: 1951389]
- Wermers RA, Fatourechi V, Wynne AG, Kvols LK, Lloyd RV. The glucagonoma syndrome. Clinical and pathologic features in 21 patients. Medicine (Baltimore) 1996; 75:53–63. [PMID: 8606627]
- Rahimy E, Sarraf D. Paraneoplastic and non-paraneoplastic retinopathy and optic neuropathy: evaluation and management. Surv Ophthalmol 2013 ; 58:430–458. [PMID: 23969019]
- Slamovits TL, Posner JB, Reidy DL, Thirkill CE, Keltner JL. Pancreatic neuroendocrine paraneoplastic optic neuropathy: confirmation with antibody to optic nerve and hepatic metastasis. J Neuroophthalmol 2013; 33:21–25. [PMID: 22926698]
- Li Destri G, Reggio E, Veroux M, Lanzafame S, Puleo S, Minutolo V. A rare cystic non-functioning neuroendocrine pancreatic tumor with an unusual presentation. Tumori 2006; 92:260–263. [PMID: 16869249]
- Yu Z, Kryzer TJ, Griesmann GE, Kim K, Benarroch EE, Lennon VA. CRMP-5 neuronal autoantibody: marker of lung cancer and thymoma-related autoimmunity. Ann Neurol 2001; 49:146–154. [PMID: 11220734]
- Cross SA, Salomao DR, Parisi JE, Kryzer TJ, Bradley EA, Mines JA, Lam BL, et al. Paraneoplastic autoimmune optic neuritis with retinitis defined by CRMP-5-IgG. Ann Neurol 2003; 54:38-50. [PMID: 12838519]
- Malik S, Furlan AJ, Sweeney PJ, Kosmorsky GS, Wong M. Optic neuropathy: a rare paraneoplastic syndrome. J Clin Neuroophthalmol 1992; 12:137–141. [PMID: 1328306]
- Honnorat J, Antoine JC, Derrington E, Aguera M, Belin MF. Antibodies to a subpopulation of glial cells and a 66 kDa developmental protein in patients with paraneoplastic neurological syndromes. J Neurol Neurosurg Psychiatry 1996; 61:270–278. [PMID: 8795598]




