Keywords
cancer referral guidelines, computer software, general practice, proforma, referral letters, triage
Introduction
In most developed countries, there is limited access to specialists. This varies from place to place, such that in some countries, patients are able to schedule an appointment with a specialist without needing to consult a generalist first. Self-referral is possible in North America for example for some US specialties (e.g. gynaecology, podiatry, dermatology and depending on some situations, cardiology, neurology, rheuma-tology and orthopaedics).1 However, general prac-titioners (GPs) or family physicians play a ‘gatekeeper’ role for many other specialties and in many other countries with some evidence of reduced costs as a result of this policy.2 Specialists must then schedule appropriate appointments to see the referred patients. In Western Australia, where this study was conducted, data published by the Health Department demonstrated a 27.7% increase in the demand for new outpatient appointments and an 18.5% increase in the demand for all outpatient appointments from 2007 to 2011.3 In some cases, this meant patients having to wait weeks and occasionally months for a specialist appointment depending on the perceived risk of serious pathology from the information recorded in the referral letter.
Patients present to GPs with undifferentiated illness such that the cause of disease may be in the physical, social and or psychological domains.4 Different GPs select different proportions of their patients for referral to specialists.5 The reasons for referral may include the need to establish a diagnosis or for treat-ment, support and or for advice. In some cases, the reason for referral is for a routine surgical procedure in other cases the reasons for referral are more complex and may include a request for specialist input to reassure a patient that the symptoms should not cause concern. Symptoms suggestive of life-limiting con-ditions, such as cancer are much more common than the incidence of such conditions in practice.6 In other words, of those patients referred to specialists most are diagnosed with benign or self-limiting problems rather than cancer.
The process of seeking a specialist opinion in most cases involves writing a letter of referral. Few cases involve a telephone conversation between the GP and the specialist and rarer still, despite technological advances, are email or videoconferencing used as a prelude to a specialist consultation. In other words, the process of communication at the interface between general practice and hospital has remained unchanged for decades. Yet letter writing is not formally taught in undergraduate or postgraduate medical courses, and even when technology is deployed computerised referral documents are often little more than ‘word’ docu-ments with few decision support functions.
It has been frequently reported that referral letters contain few details and are penned to request an appointment rather than offering a comprehensive clinical summary with a list of differential diagnosis.7 Consequently, one might speculate that the frustra-tion experienced by specialists who prioritise cases that can safely wait for specialist advice may be related to the lack of information about clinical signs and symptoms.
There has been limited success in improving the relay of information from primary care to hospital specialists. Evidence suggests that the dissemination of guidelines is not suffcient to increase the throughput of appropriate data from primary care.8 The process of referral, the need to include clinical details as part of the process, offers an opportunity to intervene with the increasing power and prevalence of computers to assist in the generation of documents or records.
We aimed to investigate how the amount of rel-evant information contained in referral letters impacts on the confidence of specialists when scheduling appointments for patients referred before and after the introduction of a computerised interactive referral proforma.
Methods
The study was approved by the Curtin Human Re-search Ethics committee (RD-54–08).
A ‘Referral Writer’ (RW) software was developed in 2008 with reference to GPs in a series of standardised patient consultations.9 The software consists of a proforma that selects the relevant patient from the doctors’ clinical software system and pre-populates that patient’s medication details and administrative information (e.g. Medicare number, date of birth and address) onto the referral letter. The software then requests the doctor to choose one of six specialties for the referral:
1 urology
2 breast
3 gynaecology
4 upper gastrointestinal (upper GI)
5 colorectal
6 respiratory.
The doctor is finally invited to enter details about the patient’s clinical condition, including his or her signs and symptoms and examination findings. The process of writing the referral could be completed in most cases with less than a dozen key strokes on the computer and within two minutes. The relevant items of history and examination were previously identified in a Delphi process by a group of GPs and specialists, published in a peer-reviewed journal and available on a website.10,11 The proforma was developed to process patient refer-rals for any condition relevant to the above specialties; not just cancer. Therefore, a patient who was being referred for a procedure, such as a vasectomy could also be referred on the same proforma that might be used for someone presenting with haematuria. The software was programmed with algorithms based on published cancer referral guidelines, such that when a patient’s signs and symptoms as entered at the time of referral match guidelines for recommended urgent referral, a referral letter is produced on the relevant template and the GP is alerted to the patient’s high risk for cancer.12 The RW included the capacity to popu-late demographic and other administrative fields from the existing clinical software system including the address, medications, allergies and past medical his-tory for referred patients.
The study consisted of two phases.
• Before the RW: For three months, the participating GPs were asked to obtain consent from patients to allow access to their referral letters. The consent included access to the specialist diagnosis.
• After the RW: The practitioners were invited to use the RW software to refer patients to the specialists. Patients referred using the RW consented for a researcher to access their referral letter. As in the phase before the RW we recorded the diagnosis of each patient referred to the specialists.
1 he information relayed in each letter was scored by a research associate with medical training before and after the RW with reference to a published measure of the amount of rel-evant clinical information in the referral letters for these six specialties.11 The letters were scored for the amount of relevant information on an excel database which automatically calculated the percentage score for each letter. Therefore it was possible to compare letters in one specialty against another.
2 The referral letters collected for this study were then anonymised and reviewed independently before and after the RW by two specialists in each field blind to the aims of the study. They were asked the questions listed in Figure 1.
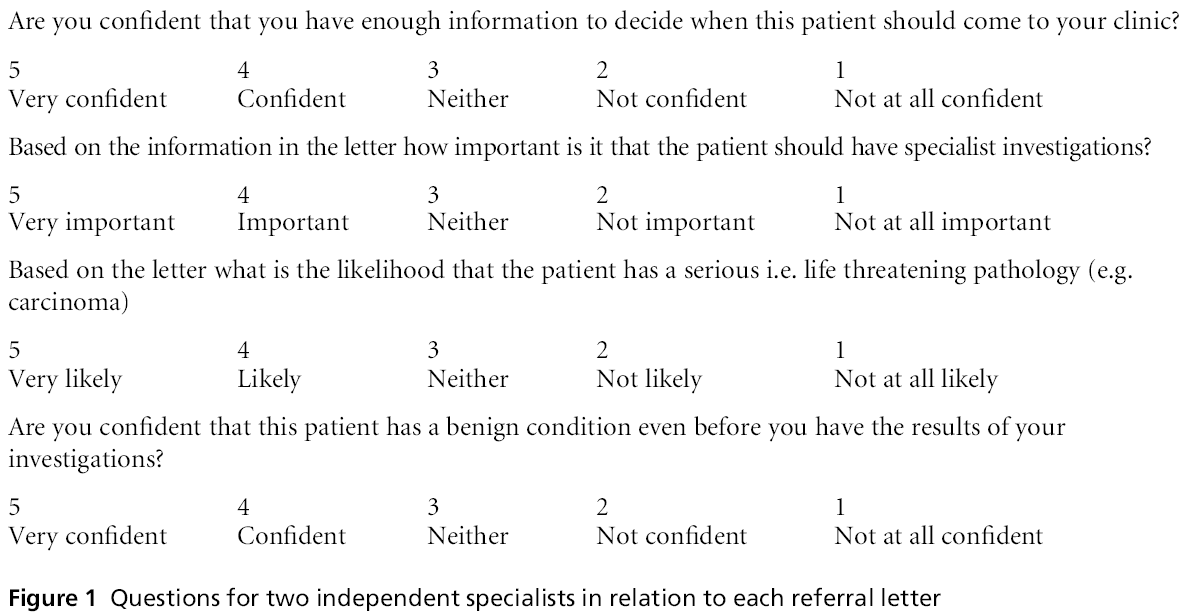
Figure 1: Questions for two independent specialists in relation to each referral letter
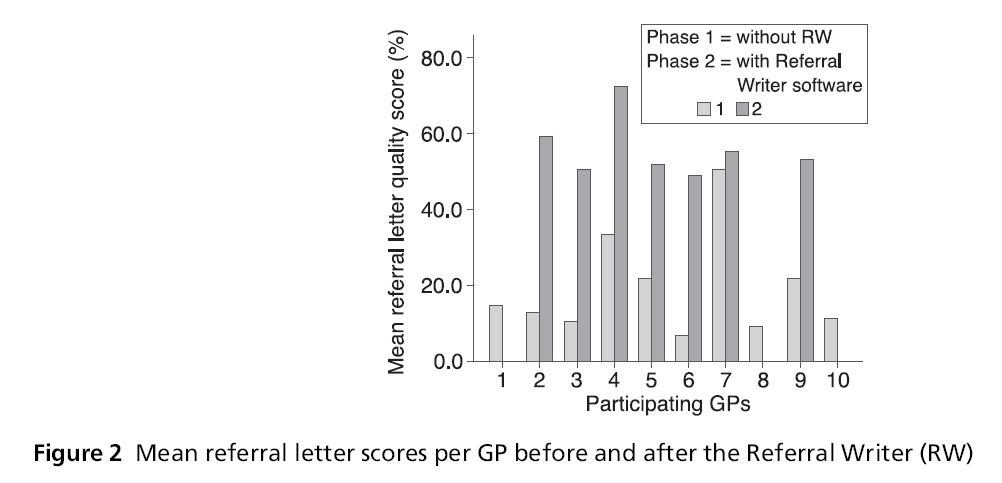
Figure 2: Mean referral letter scores per GP before and after the Referral Writer (RW)
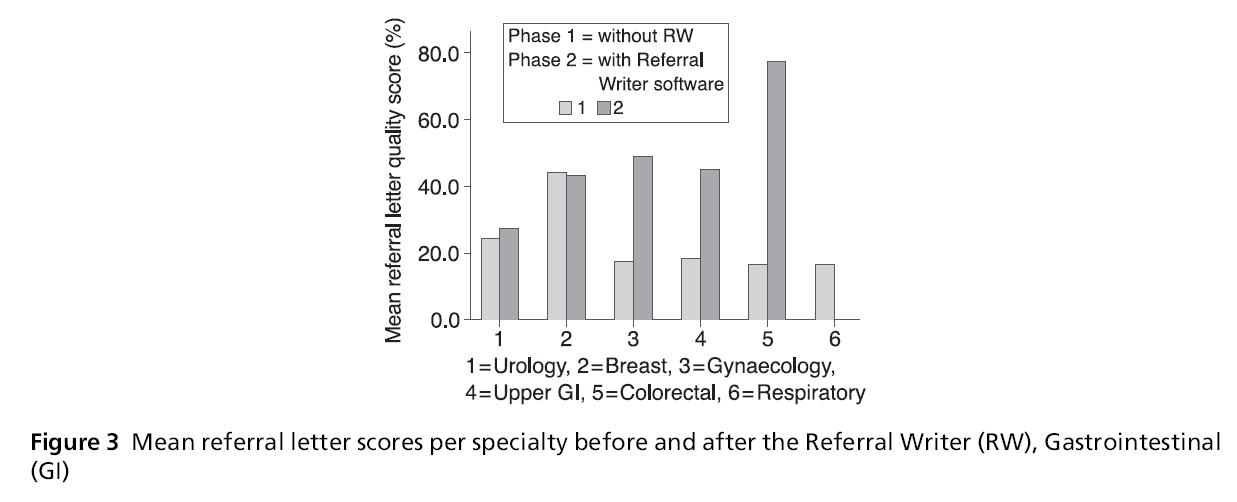
Figure 3: Mean referral letter scores per specialty before and after the Referral Writer (RW), Gastrointestinal (GI)
A list of 50 general practices who had previously expressed an interest in research conducted by the team was contacted. Ten practices were recruited in metropolitan Perth. The practitioners at each of the ten practices were briefed by members of the team, ten practitioners, one from each practice, agreed to par-ticipate and seven individual GPs completed both phases of the study. Fifty six referral letters were penned before the RW (three months) and 48 letters after the RW (four months). The ‘after’ phase lasted a month longer as one month was allowed for prac-titioners to become familiar with the software.
Results
Each GP referred a mean of 5.6 patients (range (1,14) before the RW and 4.8 patients range (0,14) after. The mean number of letters per specialty referred before the RW was 9.3, range (3,20) and 8 letters, range (0,18) after the RW. There were no referrals to respiratory physicians in the second phase of the study. The amount of clinical information relayed after the RW per GP was significantly better than before the RW. Mean score before the RW was 18.9%, mean score after was 56%, mean difference = 37%, 95% CI 43– 30%, P <0.001.
The amount of relevant information relayed per specialty was significantly greater after the RW than before the RW for gynaecological referrals, mean difference 30%, 95% CI 25–35%, P <0.001. Similarly upper GI referrals, mean difference = 25%, 95% CI 8-42%, P<0.008 and lower GI referrals, mean difference = 61%, 95% CI 55–68% P <0.001.
There was a significant difference in how the inde-pendent specialists assessed the referral letters before and after the RW. In 91% of cases both assessors after the RW were confident or very confident that they had enough information to decide when the patient should come to their clinic. There was a trend towards consensus on which patients had a benign or poten-tially life threatening condition after the RW and a significantly greater, albeit modest proportion of cases, where there was agreement between both assessors that a patient had a benign condition even before they had been seen at the clinic (see Table 1).
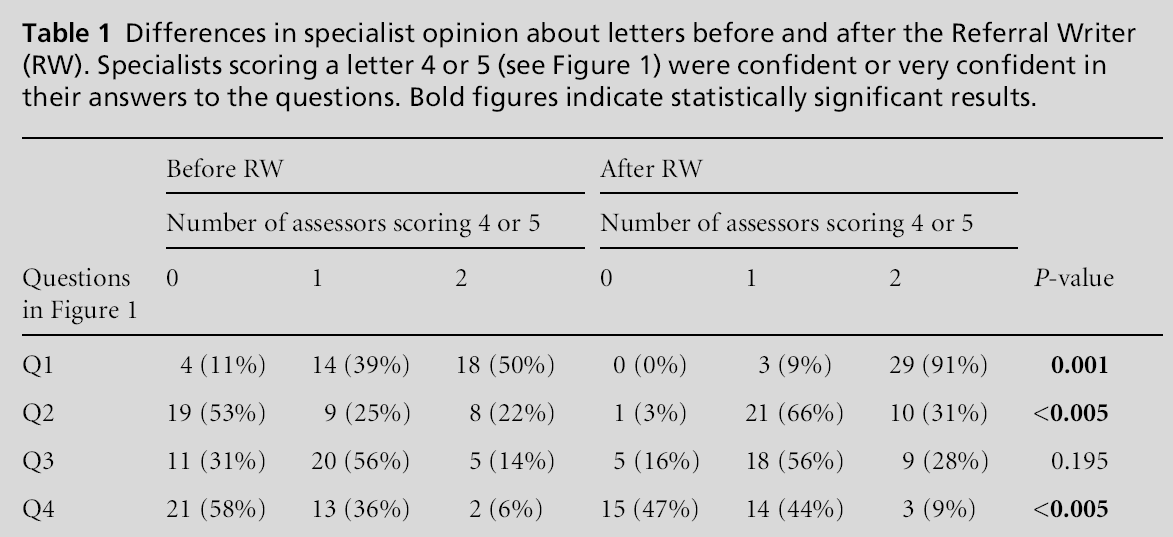
Table 1: Differences in specialist opinion about letters before and after the Referral Writer (RW). Specialists scoring a letter 4 or 5 (see Figure 1) were confident or very confident in their answers to the questions. Bold figures indicate statistically significant results.
The data on diagnoses were categorised into four groups: 1 No diagnosis yet, 2 Cancer, 3 Benign but significant pathology and 4 No data. Four cancers were diagnosed before and two after the RW. Differences in the proportion in each diagnostic group before and after the RW were not significant (Fisher’s Exact test, P= 0.25). Differences in the scores for the referral letters between each diagnostic category were not significant for any category either before or after the RW.
Discussion
The amount of relevant clinical information relayed to specialists in referral letters increased substantially after the introduction of the RW. This was the case for the majority of GPs who participated in the project and was especially true for gynaecological and gastro-intestinal referrals. These specialty referrals also ac-counted for the majority of referrals in this study. As anticipated relatively few patients were diagnosed withPreliminary evidence for the value of comprehensive referral letters 43 cancer. The specialists were more likely to agree about which patients required a specialist opinion when the RW was used. Specialists were also more confident about when to schedule appointments for patients referred using the RW.
These data are in broad agreement with the findings of previous research in which the amount of informa-tion relayed was deemed to have a significant impact on scheduling of appointments in a variety of spe-cialties.13–15 The importance of this issue is underlined
in circumstances in which patients have no access to specialists other than via their GP. This is all the more relevant in the context of conditions where the prog-nosis is dependent on any potential delay in diagnosis and treatment. Whilst there was no evidence, in this study, for a link between the amount of clinical infor-mation relayed with or without the RW and the final diagnosis, it is possible that letters that do not contain all the available information will lead to patients being inappropriately triaged and consequently having a delayed diagnosis and poorer prognosis.16 The im-portance of good communication at the interface between primary and secondary care has many bene-fits to the patient not least the assurance that in the unfortunate circumstances in which advanced disease is diagnosed it reflects the natural history of some aggressive conditions that present with minimal symp-toms rather than a failure to communicate on the part of their GP.17
This study had several limitations; the RW was adopted by practising GPs within their routine clinical practice and was applied to patients who were referred for the multiplicity of reasons stated in the introduc-tion to this paper. There were some data to indicate that the RW in its current iteration was not readily accepted by some participants. Firstly, three prac-titioners, who offered limited relevant clinical information before the RW did not submit any referrals after the RW was introduced. Secondly, overall, the number of referrals made after the RW was smaller than the number before the RW was deployed. It is possible that there were fewer patients who needed referral in the RW phase of the study. However, it is more likely that GPs did not use the RW when making all referrals in this phase. The RW did not improve the amount of relevant information relayed in the case of referrals to urology or breast clinics.
Participants in this pilot study were volunteers and therefore potentially unrepresentative of colleagues generally. Recruitment to the study was a challenge as only a relatively small proportion of those who were invited to participate agreed to join the study. This may have reflected a variety of issues including con-cern about introducing stand-alone software on to practice servers, a feeling that doctors already wrote adequate referral letters and the lack of time and remuneration for research. Finally in this small study, given the modest number of cancers diagnosed, we were unable to find evidence for an association be-tween three factors namely; the amounts of infor-mation relayed; the ability to prioritise cases and a diagnosis of cancer. This supports the assumption that it is not possible to confidently say which patients are likely to have cancer based on even a relatively large amount of information relayed by a GP.
The data in this study offer some evidence for the value of interactive computer referral proformas such as the RW in improving the utility of referral letters when patients are referred for a specialist opinion. We conclude that standardising and using electronic communications to refer may facilitate rational sched-uling of specialist appointments.
In response to the growing demand for specialist appointments noted in our introduction to this study, there is limited data here to support the deployment of letter writing software. A significant finding was the lack of evidence that even comprehensive letters might identify patients at high risk of cancer. This suggests that one solution is greater access for all patients to specialist services, an expansion of specialist clinics and perhaps greater direct access for GPs to specialist investigations. However we have no data to support this view and more research is warranted.
Conclusions
Comprehensive referral letters, which facilitate the relay of important elements of the history and exam-ination, may help to ensure that the patient is seen by the right specialist at the right time. They do not however allow the specialist to confidently identify which cases are likely to have cancer. There is a need for much more objective assessment of patients for referral such as near patient tests to help GPs to identify patients who are at risk of life threatening pathologies and then include that data in their referral letters.
Acknowledgementss
Mr Ian Peters for technical support with the Referral Writer. Dr Kerryn Butler-Henderson for adminis-trative support. We thank Jessica Hewitt and Deepa Sriram for support in preparing the manuscript and Wendy Chan She Ping-Delfos and Zaminah Khadaroo for coordinating the study. We owe a debt of thanks to the general practitioners who generously gave their time in completing this study.
References
- Forrest CB and Reid RJ. Passing the baton: HMOs0 influence on referrals to specialty care. Health Aff (Millwood) 1997;16(6):157–62.
- Delnoij D, Van Merode G, Paulus A and Groenewegen P. Does general practitioner gatekeeping curb health care expenditure? J Health Serv Res Policy 2000;5(1):22–6.
- Department of Health, Western Australia. Outpatient Quarterly Activity, WA Metropolitan Hospitals: June 2011 Quarter. Perth: Performance Reporting Branch, Per- formance Activity and Quality Division, Department of Health 2011.
- Phillips WR and Haynes DG. The domain of family practice: scope, role, and function. Family Medicine 2001;33(4):273–7.
- O0 Donnell CA. Variation in GP referral rates: what can we learn from the literature? Family Practice 2000; 17(6):462–71.
- Hamilton W. Cancer diagnosis in primary care. British Journal of General Practice 2010;60(571):121–8.
- Jiwa M, Coleman M and McKinley RK. Measuring the quality of referral letters about patients with upper gastrointestinal symptoms. Postgraduate Medical Journal2005;81(957):467–9.
- Hill VA, Wong E and Hart CJ. General practitioner referral guidelines for dermatology: do they improve the quality of referrals? Clinical and Experimental Derma- tology 2000;25(5):371–6.
- Jiwa M, McKinley RK, Spilsbury K, Arnet H and Smith M. Deploying a clinical innovation in the context of actor-patient consultations in general practice: a prelude to a formal clinical trial. BMC Medical Research Method 2009;9:54.
- Jiwa M, Deas K, Ross J, Shaw T, Wilcox H and Spilsbury K. An inclusive approach to raising standards in general practice: working with a ‘community of practice’ in Western Australia. BMC Med Res Methodol. 2009;9:13
- Cancer Learning. Primary Care Referral Toolkit. Avail-able from www.cancerlearning.gov.au/find/primary_ care.php (accessed September 2010)
- National Collaborating Centre for Primary Care. Referral Guidelines for Suspected Cancer in Adults and Children. London: Royal College of General Practi-tioners. 2005.
- Webb JB and Khanna A. Can we rely on a general practitioner’s referral letter to a skin lesion clinic to prioritize appointments and does it make a difference to the patient0 s prognosis? Annals of the Royal College of Surgeons 2006;88(1):40–5.
- Aljarabah MM, Borley NR, Goodman AJ and Wheeler JM. Referral letters for 2-week wait suspected colorectal cancer do not allow a 0 straight-to-test0 pathway. Annals of the Royal College of Surgeons 2009;91(2):106–9.
- Shaw I, Smith KM and Woodward ML. A letter of consequence: referral letters from general practitioners to secondary mental health services. Qualitative Health Research 2005;15(1):116–28.
- Iversen, LH Antonsen S, Laurberg S and Lautrup MD. Therapeutic delay reduces survival of rectal cancer but not of colonic cancer. British Journal of Surgery 2009; 96(10):1183–89.
- Wattacheril J, Kramer JR, Richardson P, Havemann BD, Green LK, Le, A and El-Serag HB. Lagtimes in diagnosis and treatment of colorectal cancer: determinants and association with cancer stage and survival. Alimentary Pharmacology & Therapeutics 2008;28(9):1166–74.
Funding
The West Australian Cancer and Palliative Care Re-search Network.
Ethical Approval
This study received Ethical Approval from Human Research Ethics Committee (HREC) at Curtin Uni-versity (RD-54–08). The participants signed an informed consent form as an acceptance to take part in the study. The referral letters produced in this study were anonymised and reviewed.
Peer Review
Not commissioned, externally Peer Reviewed.
Conflicts of Interest
The authors acknowledge no potential conflict of interest associated with the above mentioned manu-script.

