Lip Seng Lee1, Sung Hwan Lee2, 3, and Chang Moo Kang2, 3*
1Department of General Surgery, Changi General Hospital, Singapore
2Department of Hepatobiliary and Pancreatic Surgery, Yonsei University College of Medicine, Seoul, Korea
3Department of Pancreaticobiliary Cancer Clinic, Yonsei Cancer Center, Severance Hospital, Seoul, Korea
- *Corresponding Author:
- Chang Moo Kang
Department of Hepatobiliary and Pancreatic Surgery
Yonsei University College of Medicine
50-1 Yonsei-Ro, Seodaemun-Gu
Seoul 120-752, South Korea
Phone + 82-2228-2153
E-mail cmkang@yuhs.ac
Received: March 16th, 2015 Accepted: April 28th, 2015
Keywords
Gastrectomy; Pancreaticoduodenectomy
The number of patients with periampullary cancer who require pancreatoduodenectomy (PD) after radical gastrectomy for gastric cancer is small but growing. Early detection of gastric cancer from national screening programs, more aggressive surgical approaches for radical gastrectomy, a deeper understanding of tumor biology, and better efficacy of postoperative adjuvant treatment have resulted in longer survival [1]. Improved survival will increase the probability for a second primary cancer to occur [2]. If periampullary cancer occurs in patients with previous radical gastrectomy for gastric cancer, PD should be the standard treatment. PD itself, a complex procedure associated with a high incidence of postoperative morbidity, will only be more complex in patients with previous radical gastrectomy. Consequently, pancreatic surgeons need to be aware of intra-abdominal anatomic changes in patients with previous radical gastrectomy for gastric cancer, and be prepared for these challenging complex procedures.
We have already described the complexity of PD as a second operation in patients with radical subtotal gastrectomy [2], offering several technical tips. First, understanding adhesion of the pancreas to the subhepatic area of the left hepatic lobe leading to upward traction of the pancreas can help surgeons identify the altered pancreas anatomy more easily. Second, taking extra care during dissection of the major vessels of the celiac trunk branches can help to avoid injury to them, because there is little soft tissue left around these vessels to buffer the electric insult during Bovie dissection. Third, the SMV and pancreatic neck portion at the inferior surface of the pancreas should be identified first for safe anatomical dissection in order to avoid the extensive adhesion at the superior border of the pancreas where extensive lymph node dissection at the hepatoduodenal ligament previously took place. Fourth, because there is no more remnant stomach for pancreatico-gastrostomy (PG) reconstruction, a familiarity with pancreatico-jejunostomy (PJ) reconstruction is needed. Finally, Roux-en-y fashioned reconstruction with an intact, functioning previous gastrojejunostomy can be recommended in patients with previous gastrojejunostomy (Billroth type II).
As for PD following radical total gastrectomy (RTG), only a handful of case reports have been published [3-6]. There is no standardized method for reconstruction after PD in a patient with previous total gastrectomy. Moreover, there is a risk of afferent loop syndrome after using the same afferent jejunal limb for reconstruction of PJ and hepatico-jejunostomy (HJ) [3, 6]. After a RTG, Rouxen- Y esophagojejunal reconstruction is usually carried out to preserve duodenal and jejunal continuity with an aim towards minimizing postgastrectomy functional disturbance.
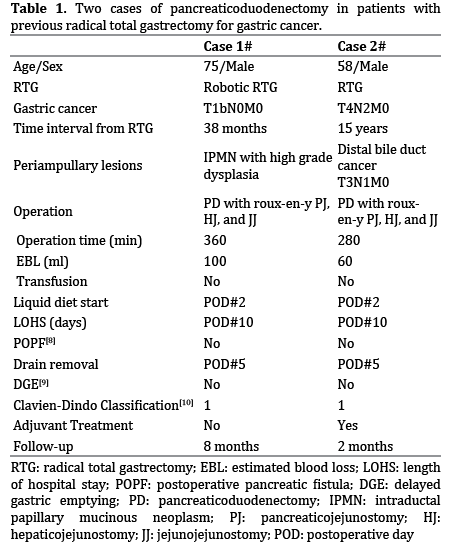
We recently experienced two cases of periampullary cancer following RTG for gastric cancer. Both cases were identified during the follow up of the gastric cancer with computed tomography (CT) scans. Upon identifying the lesions, magnetic resonance imaging (MRI) scans were performed to further characterize them and positron emission tomography-CT (PET-CT) scans also showed the tumors’ metabolic activity. Both patients consented for surgery based on the imaging findings. When performing PD in those cases, the previous esophago-jejunostomy (EJ) was maintained, and a new Roux-en-y reconstruction was made by resecting only the afferent loop (Figure 1a). The distal jejunum was used for the PJ and HJ reconstruction and formation of a new distal jejunojejunostomy (Figure 1b) located at 40cm from the HJ. Doi et al. [6] reported a similar reconstruction method with the previous EJ preserved, but the order of anastomosis was different from ours (choledochojejunotstomy-pancreaticojejunostomyjejunojejunostomy). Interestingly, Noguchi, et al. [7] chose the same reconstruction technique, and reported no significant postoperative complications. We also observed no complications during postoperative recovery (Table 1). Therefore, reconstruction using Roux-en-y with a previous EJ intact appears to be safe and simple compared with other approaches [1, 6]. However, there have been few reports about the reconstruction of PD after previous RTG, and further investigation from multiple centers is needed to define the optimal method.
Figure 1. a. Pancreatoduodenectomy with the afferent jejejunal loop resected and the previous esophago-jenunostomy maintained. b. A new Roux-en-y
reconstruction by using the distal jejunum for the pancreaticojejunostomy and hepaticojejunostomy and formation of a new jejunojejunostomy distally.
In conclusion, periampullary cancer as a second primary is becoming more common due to longer survival from early detection and aggressive treatment of gastric cancer. PD after a RTG is rare, but challenging. Therefore, pancreatic surgeons need to understand the complexity of the operation and potential techniques to increase the likelihood of a safe outcome for the patient. PD with reconstruction using Roux-en-y PJ, HJ, and distal JJ with previous EJ preserved can be one option when considering PD in patients with previous RTG.
Acknowledgment
The authors would like to express special thanks to Dong- Su Jang (Medical Illustrator, Medical Research Support Section, Yonsei University College of Medicine, Seoul, Korea) for his excellent illustrations in the papers.
Conflicting Interest
The authors had no conflicts of interest
References
- Yamamoto M, Rashid OM, Wong J. Surgical management of gastric cancer: the East vs. West perspective. J Gastrointest Oncol 2015; 6: 79-88. [PMID: 25642341]
- Kim SH, Hwang HK, Kang CM, Lee WJ. Pancreatoduodenectomy in patients with periampullary cancer after radical subtotal gastrectomy for gastric cancer. Am Surg 2012; 78: E164-167. [PMID: 22524749]
- Yokoyama S, Sekioka A, Ueno K, Higashide Y, Okishio Y, Kawaguchi N, Hagihara T, Yamada H, et al.Pancreaticoduodenectomy following total gastrectomy: a case report and literature review. World J Gastroenterol 2014; 20: 2721-2724. [PMID: 24627609]
- Oida T, Kano H, Mimatsu K, Kawasaki A, Kuboi Y, Fukino N, Kida K, Amano S. Jejunal scarf-covering method in pancreaticojejunostomy after total gastrectomy. Case Rep Gastroenterol 2012; 6: 472-477. [PMID: 22855663]
- Mizuno S, Isaji S, Ohsawa I, Kishiwada M, Hamada T, Usui M, Sakurai H, Tabata M. Pancreaticoduodenectomy with resection of the splenic artery and splenectomy for pancreatic double cancers after total gastrectomy. Preservation of the pancreatic function via the blood supply from the posterior epiploic artery: report of a case. Surg Today 2012; 42: 482-488. [PMID: 22068672]
- Doi R, Fujimoto K, Imamura M. Effects of preceding gastrectomy on the outcome of pancreatoduodenectomy. J Gastrointest Surg 2004; 8: 575-579. [PMID: 15239994]
- Noguchi K, Okada K, Kawamura H, Ishizu H, Homma S, Kataoka A. Operative procedure for pancreatoduodenectomy in a patient who had previously undergone total gastrectomy, distal pancreatectomy, and splenectomy. Am Surg 2012; 78: 103-105. [PMID: 22369814]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, et al. International Study Group on Pancreatic Fistula D. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138: 8-13. [PMID: 16003309]
- Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, et al. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007; 142: 761-768. [PMID: 17981197]
- Lee KG, Lee HJ, Yang JY, Oh SY, Bard S, Suh YS, Kong SH, Yang HK. Risk factors associated with complication following gastrectomy for gastric cancer: retrospective analysis of prospectively collected data based on the Clavien-Dindo system. J Gastrointest Surg 2014; 18: 1269-1277. [PMID: 24820136]


