Keywords
Anaphylaxis; Bronchial Spasm; Cisplatin; Exanthema; Hypersensitivity; oxaliplatin; Pancreatic Neoplasms; Skin Tests
Abbreviations
GemOx: gemcitabine and oxaliplatin
INTRODUCTION
Gemcitabine (Gemzar®, Eli Lilly, Indianapolis, IN, USA) is the only standard chemotherapy approved by the US Food and Drug Administration (FDA) for the treatment of advanced pancreatic cancer [1]. Many studies have sought more effective gemcitabine-based combination therapies, but most of them showed no statistical significance in survival data. However, a recent meta-analysis has suggested that the platinum salts oxaliplatin and cisplatin, in combination with gemcitabine, can lead to improved survival in patients with pancreatic cancer, especially those with a good performance status [2, 3].
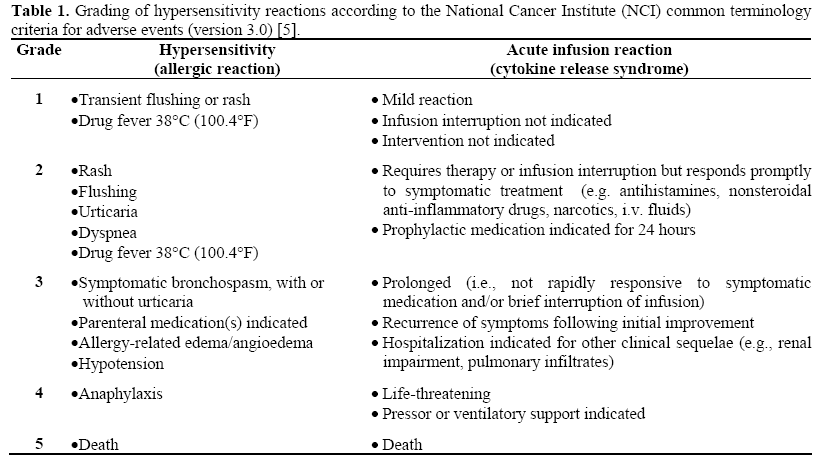
In the administration of these more aggressive platinum regimens, there is potential risk that the patients will experience common toxicities, including hypersensitivity reactions. The overall incidence of oxaliplatin and cisplatin hypersensitivity reactions can reach up to 20%, with a 2-4% incidence of grade 3 or 4 reactions, based on different literature, and can include pruritus, bronchospasm, erythema, and hypotension, in addition to other adverse effects [4, 5] (Table 1). There are a few options to prevent hypersensitivity reactions, such as premedication with steroids and antihistamines, prolonged infusion time, and desensitization [4]. Another option to continue with a platinum-based therapy is to rechallenge with a different platinum salt, but the hazardous potential of cross-reactivity leads to the necessity of intradermal skin tests in determining future therapy. If a test is negative, then the continuation of platinum chemotherapy can occur [6].
We present a patient with advanced pancreatic cancer and prior hypersensitivity reaction to oxaliplatin who successfully underwent a switch in platinum therapy. He was able to receive eight complete cycles of gemcitabine and cisplatin at our institution without developing a hypersensitivity reaction.
CASE REPORT
A 58-year-old white male with an unremarkable past medical history presented with nausea, vomiting, and a 9 kg weight loss in February of 2007. An ultrasound of the abdomen revealed multiple masses in the liver. A CT scan further confirmed, in addition to the liver lesions, several dozen subcentimeter nodules throughout both lungs, and small scattered mediastinal lymph nodes. A CT scan-guided biopsy of one of the liver masses revealed pathology consistent with infiltrating adenocarcinoma; the tumor was cytokeratin 7 (CK7) and 20 (CK20) positive, CEA positive, and CA 19-9 rarely positive. Given the presumptive diagnosis of adenocarcinoma of unknown primary seemingly from the gastrointestinal tract, the patient had an MRI and MRCP of the abdomen performed, with no remarkable results. Work-up was completed with an upper and lower endoscopy, endoscopic ultrasound, and PET scan, which all were unable to locate a primary site.
Assuming a pancreaticobiliary origin, based on the immunohistochemistry of malignancy, the patient was started on a biweekly treatment with gemcitabine and oxaliplatin (GemOx) [7]. The regimen consisted of a 30- minute infusion of gemcitabine (1,000 mg/m2) followed by 2-hour infusion of oxaliplatin (100 mg/m2). He was premedicated with intravenous (i.v.) ondansetron (8 mg) and dexamethasone (10 mg), as well as i.v. push lorazepam (0.5 mg) to prevent nausea and vomiting. He was also given i.v. magnesium sulfate (1 g) and calcium glutonate (1 g) before and after oxaliplatin infusion, in order to reduce potential neurotoxicities [8]. Therapy was tolerated well, with only one instance of vomiting and grade 1 transient neuropathy during the first cycle, as well as grade 1 intermittent fatigue, and grade 1 hypersensitivity to cold within the first week of the fourth cycle.
Just a few minutes before the end of infusion for the fifth cycle of oxaliplatin, the patient developed erythema on his face and neck. He also stated that his lips felt numb, without eating or drinking anything cold. The infusion was immediately stopped, and i.v. diphenhydramine (25 mg) and dexamethasone (10 mg) were given. The patient had no shortness of breath, and vitals were stable. As the erythema spread down his neck, back, chest and lower abdomen with significant confluence as well as periorbital edema, he was further treated with i.v. famotidine (20 mg) and additional diphenhydramine (25 mg). The patient was then transported to the emergency room via ambulance. He was observed over a 24-hour period and discharged the next day on dexamethasone and diphenhydramine, in stable condition.
To prevent peri-oral anesthesia and grade 1 hypersensitivity reaction, it was decided to prolong the infusion over 4 hours, with additional premedications including an increase in dexamethasone (20 mg), plus i.v. diphenhydramine (50 mg) and famotidine (20 mg). The only adverse reaction was a grade 1 hypersensitivity to cold lasting up to a week. The seventh cycle was also administered without complication. Then during the eighth cycle, 30 minutes into the 4-hour infusion of oxaliplatin running at 135 mL/h (27 mg), the patient was noted to have grade 2 facial flushing and grade 4 shortness of breath at rest, and the infusion was stopped immediately. The patient complained of dyspnea and chest tightness (both grade 1), and his lips appeared slightly cyanotic. He received additional i.v. push diphenhydramine (50 mg), dexamethasone (20 mg), famotidine (20 mg), and subcutaneous administration of epinephrine (0.5 mg). Within 15-20 minutes the symptoms had resolved, except for grade 1 rigors, for which i.v. push meperidine hyrochloride (25 mg) was given with relief. The patient was observed for the next three hours, and discharged home with his family. The hypersensitivity reaction was graded as a 3.
After a severe hypersensitivity reaction (grade 3 or higher), the only option to continue oxaliplatin treatment would be desensitization [4, 9, 10]. However, due to the potential fatality and subsequent issues (i.e. the need for an intensive care unit bed), other options were pursued. The patient’s excellent response to the GemOx regimen (partial response: 48% decrease in tumor, including disappearance of all lung nodules; CA 19-9 dropped from 52.3 to 34.4 U/mL (reference range 0-37 U/mL) warranted the consideration of using another platinum salt, such as cisplatin [11].
In order to rule out the possibility of platinum cross-reactivity, a cisplatin skin test was administered on the patient, 0.04 mL intradermally on the volar surface of the arm. The result was negative and so he was treated 75 minutes later with the new regimen of gemcitabine (1,000 mg/m2) and cisplatin (50 mg/m2). The gemcitabine was administered over 30-minute infusion followed by a 1-hour infusion of cisplatin; premedications included ondansetron (16 mg), dexamethasone (20 mg), lorazepam (0.5 mg); also, 3-hour cisplatin hydration (1,000 mL) infusion was given before chemotherapy with mannitol (12.5 g), magnesium sulfate (2 g), and potassium chloride (20 mEq) as per institutional guidelines.
The patient’s tumor size continued to decrease by an additional 14% since starting the gemcitabine and cisplatin therapy, and CA 19-9 further dropped to 28 U/mL. This is the first case reported for a successful rechallenge of cisplatin for a metastatic pancreatic cancer patient with hypersensitivity reaction to oxaliplatin.
DISCUSSION
For advanced pancreatic cancer, many combination chemotherapy trials incorporating gemcitabine, cisplatin, 5-FU, oxaliplatin, or irinotecan generally show improved outcomes in objective response rates, but there has been little or no improvement in overall survival in phase III trials [12].
Despite two randomized studies [7, 11], a recent pooled analysis of two randomized trials showed improved survival in patients with pancreatic cancer, especially those with a good performance status [2]. Additional authors have suggested that the optimal treatment for pancreatic cancer involves gemcitabine in combination with platinum salts, as well as fluoropyrimidines or erlotinib, based on meta-analysis and logical considerations [13]. Overall, the combination therapies are recommended for those patients with a good performance status. As our patient presented with good status (Eastern Cooperative Oncology Group: ECOG=0), we decided to go forward with the more aggressive regimen of GemOx.
The difficulty of treating some patients with the gemcitabine/platinum chemotherapy comes from the increased risk of toxicities, such as hypersensitivity reactions. An hypersensitivity reaction is defined as an unexpected reaction that cannot be explained by the known toxicity profile of the chemotherapeutic agent [14]. Oxaliplatin hypersensitivity reactions are prevalent in about 10-12% of patients, but incidence ranges from 1-19% based on the literature, while severe (grade 3/4) reactions occur in about 1-3% patients [3, 15, 16, 17]. The range of symptoms includes flushing, alterations in heart and blood pressure, bronchospasm, back pain, chest discomfort, fever, rash, pruritus, erythema, and nausea [18]. Cisplatin causes similar types of reactions, as well as facial edema, anxiety, cough, and dyspnea [19]. Its incidence is not as widely documented, but occurs in about 5-20% of patients, with a higher chance of reaction if administered with another chemotherapeutic agent [20]. For the platinum agents, hypersensitivity reactions usually occur after multiple treatments, around six cycles [21].
around six cycles [21]. Cross-hypersensitivity reactions can be serious complications of platinum agents. However, experience in gynecologic oncology suggests that there seems to be no general cross-reactivity to cisplatin in patients who developed hypersensitivity reaction to carboplatin. However, such data is scarce in patients with gastrointestinal tumors, such as pancreas.
The pathophysiology of these hypersensitivity reactions is not well understood, but it is thought that the majority of them are consistent with an immediate type I reaction, possibly mediated by drug-specific IgE [22]. The platinum agents, their metabolites, and vehicles may also induce mast cell or basophil degranulation directly, resulting in responses that are indistinguishable from IgE-mediated allergic reactions [23]. It is also postulated that platinum salts could bind to major histocompatibility complex class 2 molecules and act as superantigens causing lymphocyte activation, with several predisposing factors as suspects [4]. A past history of adverse drug reaction, geographic origin, HLA phenotype, or cigarette smoking could influence individual hypersensitivity to platinum salts [4].
When hypersensitivity reactions do occur, there are few options which allow the continuation of a platinum-based therapy. Additional pretreatment, consisting of corticosteroids and antagonists of histamine type 1 and 2 receptors, has subdued future reactions with mixed results in oxaliplatin, and very few times in cisplatin regimens. The prolonging of infusion time has proved a little more effective in preventing future hypersensitivity reactions. Finally, the process of desensitization has allowed oxaliplatin and cisplatin to continue in the regimens, by administering serial dilutions of the platinum salt in a gradual dose escalation, along with additional premedications. For oxaliplatin hypersensitivity reactions, the addition of calcium gluconate and magnesium sulfate was previously reported to have good effect in the desensitization process. However, recent release of preliminary results of the Combined Oxaliplatin Neuropathy Prevention Trial (CONCEPT) study warns about the use of calcium gluconate and magnesium sulfate reducing the efficacy of oxaliplatin [24].
If the patient still develops a hypersensitivity reaction after desensitization, there may be the option of substituting a different platinum salt into the regimen. A negative intradermal skin test for the particular platinum is a reliable indicator for an effectual rechallenge, but it has only been used a few times for the use of switching platinum therapy [25, 26, 27]. Up to date, there has only been one study that initiated a rechallenge of cisplatin after a hypersensitivity reaction to oxaliplatin. Leguy-Seguin et al. describe three patients who experienced hypersensitivity reaction due to oxaliplatin and were subsequently treated with cisplatin after testing negative to the cisplatin intradermal skin test [27]. In all three cases, there was no report of drug related adverse reaction. Unfortunately, the subjects' primary cancer types were not disclosed, so the impact of this chemotherapeutic method cannot be fully realized.
Our case report presents what we believe to be the first successful rechallenge of cisplatin to a metastatic pancreatic cancer patient with hypersensitivity reaction to oxaliplatin. Although there is always a possibility of cross-reactivity, the reintroduction to platinum-based therapy can be considered in a supervised environment if the patient has already experienced a good objective response. Skin tests offer a simple procedure to direct these decisions, and our patient has benefited from such a strategy. Therefore, future studies are warranted to validate the role of intradermal skin test and safety of substituting a platinum agent.
Conflict of interest
The authors have no potential conflicts of interest
References
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as firstline therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15:2403-13. [PMID 9196156]
- Heinemann V, Labianca R, Hinke A, Louvet C. Increased survival using platinum analog combined with gemcitabine as compared to single-agent gemcitabine in advanced pancreatic cancer: pooled analysis of two randomized trials, the GERCOR/GISCAD intergroup study and a German multicenter study. Ann Oncol 2007; 18:1652-9. [PMID 17660491]
- Saif MW, Kim R. Role of platinum agents in the management of advanced pancreatic cancer. Expert Opin Pharmacother 2007; 8:2719-27. [PMID 17956194]
- Saif MW. Hypersensitivity reactions associated with oxaliplatin. Expert Opin Drug Saf 2006; 5:687-94. [PMID 16907658]
- National Cancer Institute. Common Terminology Criteria for Adverse Events v3.0. (CTCAE). Publish date August 9, 2006.
- Markman M, Zanotti K, Peterson G, Kulp B, Webster K, Belinson J. Expanded experience with an intradermal skin test to predict for the presence or absence of carboplatin hypersensitivity. J Clin Oncol 2003; 21:4611-4. [PMID 14673050]
- Louvet C, Labianca R, Hammel P, Lledo G, Zampino MG, André T, et al. Gemcitabine in combination with oxaliplatin compared with gemcitabine alone in locally advanced or metastatic pancreatic cancer: results of a GERCOR and GISCAD phase III trial. J Clin Oncol 2005; 23:3509-16. [PMID 15908661]
- Wrzesinski SH, McGurk ML, Donovan CT, Ferencz TM, Saif MW. Successful desensitization to oxaliplatin with incorporation of calcium gluconate and magnesium sulfate. Anticancer Drugs 2007l; 18:721-4. [PMID 17762403]
- Goldberg A, Confino-Cohen R, Fishman A, Beyth Y, Altaras M. A modified, prolonged desensitization protocol in carboplatin allergy. J Allergy Clin Immunol 1996; 98:841-3. [PMID 8876561]
- Meyer L, Zuberbier T, Worm M, Oettle H, Riess H. Hypersensitivity reactions to oxaliplatin: crossreactivity to carboplatin and the introduction of a desensitization schedule. J Clin Oncol 2002; 20:1146- 7. [PMID 11844841]
- Heinemann V, Quietzsch D, Gieseler F, Gonnermann M, Schönekäs H, Rost A, et al. Randomized phase III trial of gemcitabine plus cisplatin compared with gemcitabine alone in advanced pancreatic cancer. J Clin Oncol 2006; 24:3946-52. [PMID 16921047]
- Saif MW. Pancreatic cancer: is this bleak landscape finally changing? Highlights from the '43rd ASCO Annual Meeting'. Chicago, IL, USA. June 1-5, 2007. JOP. J Pancreas (Online) 2007; 8:365-73. [PMID 17625289]
- Xie DR, Liang HL, Wang Y, Guo SS, Yang Q. Meta-analysis on inoperable pancreatic cancer: a comparison between gemcitabine-based combination therapy and gemcitabine alone. World J Gastroenterol 2006; 12:6973-81. [PMID 17109519]
- Shepherd GM. Hypersensitivity reactions to chemotherapeutic drugs. Clin Rev Allergy Immunol 2003; 24:253-62. [PMID 12721396]
- Brandi G, Pantaleo MA, Galli C, Falcone A, Antonuzzo A, Mordenti P, et al. Hypersensitivity reactions related to oxaliplatin (OHP). Br J Cancer 2003; 89:477-81. [PMID 12888815]
- Siu SW, Chan RT, Au GK. Hypersensitivity reactions to oxaliplatin: experience in a single institute. Ann Oncol 2006; 17:259-61. [PMID 16282245]
- Gowda A, Goel R, Berdzik J, Leichman CG, Javle M. Hypersensitivity Reactions to oxaliplatin: incidence and management. Oncology (Williston Park) 2004; 18:1671-5. [PMID 15648298]
- Thomas RR, Quinn MG, Schuler B, Grem JL. Hypersensitivity and idiosyncratic reactions to oxaliplatin. Cancer 2003; 97:2301-7. [PMID 12712487]
- Koren C, Yerushalmi R, Katz A, Malik H, Sulkes A, Fenig E. Hypersensitivity reaction to cisplatin during chemoradiation therapy for gynecologic malignancy. Am J Clin Oncol 2002; 25:625-6. [PMID 12478013]
- Shlebak AA, Clark PI, Green JA. Hypersensitivity and cross-reactivity to cisplatin and analogues. Cancer Chemother Pharmacol 1995; 35:349-51. [PMID 7828281]
- Markman M. Toxicities of the platinum antineoplastic agents. Expert Opin Drug Saf 2003; 2:597-607. [PMID 14585068]
- Stahl M, Köster W, Wilke H. Reaction after oxaliplatin--prevention with corticosteroids? Ann Oncol 2001; 12:874. [PMID 11484969]
- Zanotti KM, Markman M. Prevention and management of antineoplastic-induced hypersensitivity reactions. Drug Saf 2001; 24:767-79. [PMID 11676304]
- Hochster HS, Grothey A, Childs BH. Use of calcium and magnesium salts to reduce oxaliplatinrelated neurotoxicity. J Clin Oncol 2007; 25:4028-9. [PMID 17664456]
- Porzio G, Marchetti P, Paris I, Narducci F, Ricevuto E, Ficorella C. Hypersensitivity reaction to carboplatin: successful resolution by replacement with cisplatin. Eur J Gynaecol Oncol 2002; 23:335-6. [PMID 12214738]
- Gottlieb MJ, Nelson B, Perry W. Utility of skin test for allergy to carboplatin or cisplatin. J Allergy Clin Immunol 1998; 101:S139.
- Leguy-Seguin V, Jolimoy G, Coudert B, Pernot C, Dalac S, Vabres P, Collet E. Diagnostic and predictive value of skin testing in platinum salt hypersensitivity. J Allergy Clin Immunol 2007; 119:726-30. [PMID 17258305]

