Keywords
Animals; Catheter Ablation; Pancreas; Swine
Abbreviations
RF: radiofrequency; RFA: radiofrequency ablation
INTRODUCTION
Over the last decade radiofrequency energy has become increasingly accepted for the ablation of solid parenchymal tumours [1, 2, 3], in particular liver tumours [4, 5]. In contrast to the liver, where tumour-bearing tissue will be surrounded by normal hepatic parenchyma, the pancreas is surrounded by structures such as the duodenum and common bile duct and concerns regarding the risks for causation of thermal injury to these structures have limited the use of radiofrequency for non-resectable pancreas tumours. We recently reported the development of an ex-vivo model of radiofrequency ablation of the porcine pancreas [6]. In this model, thermal injury was recognizable by conventional histologic methods and was also characterized by loss of tissue oxidative enzyme activity measured as loss of nicotinamide adenine dinucleotide (NADH) activity [6].
Contemporary probe design permits the creation of a spherical area of ablation. The extent of ablation is influenced by the thermal efficiency and characteristics of the delivery system and also by factors intrinsic to the tissue such as impedance and the cooling effect (known as the ‘heat-sink’) of nearby visceral circulation.
The aim of this study is to explore the feasibility for modulation of radiofrequency ablation by variations in probe temperature and duration of ablation and further to examine the effect of simulated portal venous circulation in this ex-vivo porcine model.
METHODS
Specimen Retrieval, Sample Preparation and Set-up of Ex-Vivo Radiofrequency Ablation Apparatus
This process is described in detail elsewhere [6]. In brief, 30 healthy 6-month-old pigs undergoing sacrifice in a commercial abattoir were used. The intact pancreas with visceral attachments was retrieved from a commercial abattoir within half an hour of the animal being sacrificed (no animals were sacrificed for the purpose of the study and tissues that were used were otherwise to be discarded). The specimen was brought immediately to the laboratory in a clean, non-sterile plastic container. No preservation was used. The specimen was placed on a metal tray attached to the earth plate of the radiofrequency (RF) applicator. A point of ablation was chosen in the head of pancreas (cranial pancreas) where it is closely attached to the duodenum. This point is equidistant (2 cm) from the inferior border of first part of duodenum and the common bile duct. The centre of ablation was marked with an indelible marker pen prior to insertion of the probe. The probe was inserted for 3 mm into the pancreas at the selected point and secured in place using an external Jclamp. A Starburst XL multi-array probe (RITA Systems Inc., Mountain View, CA, USA) bearing seven individual probe-tip thermal sensors was used for radiofrequency ablation. Probe arrays were deployed to achieve an ablation diameter of 2 cm. During application of radiofrequency energy voltage (power delivered and power used), impedance, and individual array-tip temperatures were continuously monitored. These parameters were displayed on a laptop computer screen during ablation and recorded in real-time mode.
After ablation, biopsies were taken from the ablated area including part of the duodenum, bile duct and portal vein. For each experiment a control biopsy of non-ablated pancreas was taken from the tail of the gland. Biopsies were immediately snap frozen in liquid nitrogen and stored at -70°C until specimen preparation. Paired haematoxylin and eosin (H&E) and nicotinamide adenine dinucleotide (NADH) stained specimens were prepared as described previously [6].
Simulated Portal Perfusion
A haemofiltration machine (BSM-22 SC, Hospal, Medolla, Italy) was used to simulate portal circulation. The portal vein was identified cephalic to the pancreas and the superior mesenteric vein at the inferior border of the gland. All tributaries were carefully ligated with 2-0 vicryl (Ethicon, Edinburgh, UK) taking care not to narrow the lumen of the vein. The infra-pancreatic superior mesenteric vein was then intubated with plastic haemodialysis tubing which was ligated in place. The cephalic opening (portal vein) was similarly cannulated and the tube secured by ligature. The portal vein was then perfused using normal (non-buffered) saline at 37°C. A pulsed flow rate of 100 mL/min was maintained at a pressure of 100 mmHg.
Ablation Protocols
In this model, a maximal ablation diameter of 2 cm can be achieved. Keeping a constant 2 cm ablation diameter, the effects of variation in final target (tissue) temperature and in duration of ablation were evaluated. All experiments were repeated five times at each setting (variation in temperature or duration of ablation) with a new specimen being used for each experiment.
a) Variation in Target Temperature
In prior studies, a target temperature of 100°C with duration of ablation of 10 minutes was associated with complete ablation of pancreatic parenchyma but was associated with evidence of thermal injury to the common bile duct and portal vein [6]. In order to assess optimal temperature-duration combinations these experiments examined first a stepwise reduction in target temperature from 100°C to 80°C in 10°C intervals whilst maintaining the duration of ablation constant at 10 minutes. At all set temperatures, experiments were repeated on 5 separate pancreata. The tissue target temperature of 80°C was established as a minimal temperature as previous experiments had indicated that there was no effect of ablation at lower temperatures.
b) Variation in Duration of Ablation
The effect of more prolonged ablation at the minimal temperature at which an effect of ablation could be observed (80°C) was examined. The effect of a shorter period of ablation was then examined separately (for these experiments a target temperature of 90°C was selected).
Effect of Simulated Portal Perfusion
Setting ablation diameter at 2-cm, target temperature at 90°C and duration of ablation at 10 minutes, the effect of simulated portal flow on ablation was examined.
Principal Outcomes
There were two main outcomes for this study. First, the study aimed to define the optimum temperature and time for causing effective ablation in this model and to identify whether this optimum temperature/time combination was associated with evidence of injury to peri-pancreatic structures - principally the duodenum, bile duct and portal vein. Second, the study aimed to assess whether simulated portal circulation affected ablation.
Assessment of Outcome
All histologic preparations were examined by a histopathologist who was unaware of the intervention undertaken. All effects of ablation were assessed using loss of NADH activity. In previous studies, this group has demonstrated that this is a reliable and sensitive means of assessing ablation. Conventional haematoxylin and eosin preparations were also made of all slides as recognition of thermal injury to peripancreatic viscera was clearly seen, when present, in these slides.
ETHICS
The pancreata used in the study were retrieved from the animals sacrificed in commercial abattoir. No animals were sacrificed for the purpose of the study and tissues that were used were otherwise to be discarded. Therefore, ethics committee approval was not necessary.
DATA ANALYSES
Quantitative and semi-quantitative histological injury scores have been used to assess thermal injury by several groups (including this group) but can be criticized for categorisation of continuously variable parameters and are not reliably validated for assessment of thermal ablation of pancreatic and peri-pancreatic tissue. Accordingly, data are presented in a factual descriptive format: either the tissue in question was normal or there was evidence of injury on both H&E and NADH preparation. The extent of injury is not further quantitated.
RESULTS
Effects of Variation in Target Temperature (Table 1).
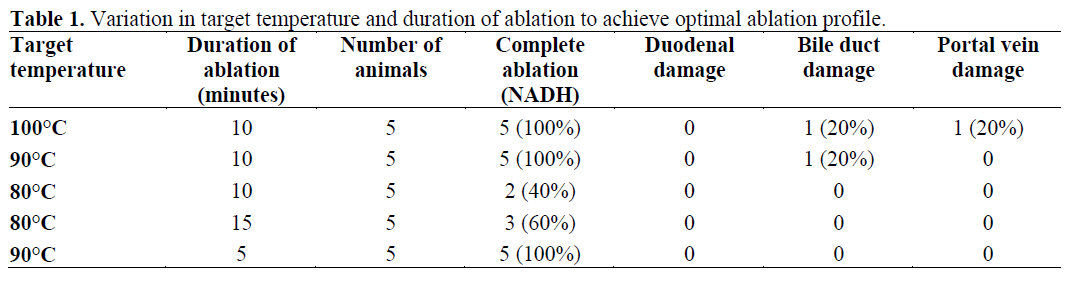
Complete ablation of pancreatic parenchyma was noted at a target temperature of 100°C for 10 minutes. At this setting there was evidence of thermal injury to the common bile duct in one animal and similarly the portal vein in one animal. The normal appearances of the porcine bile duct are seen in Figure 1a (H&E) and an NADH preparation is seen in Figure 1b. Thermal injury to the bile duct was characterized by disaggregation of biliary epithelium with oedema of the subepithelial tissues on H&E staining (Figure 2a) and loss of oxidative enzyme activity in epithelial and subepithelial tissues on NADH staining (Figure 2b).
Figure 1. Normal common bile duct. a. H&E stain
(magnification x40). Note preservation of normal
ductal epithelium. b. NADH stains (magnification
x40). Preservation of oxidative enzyme activity in
ductal epithelium.
Figure 2. Ablated common bile duct. a. H&E stain
(magnification x20). Note the disaggregated biliary
epithelium and oedema of the subepithelial tissues. b. NADH stains (magnification x20). Note loss of
oxidative enzyme activity in epithelial and
subepithelial tissues.
The normal appearances of the porcine portal vein are seen in Figures 3a (H&E) and 3b (NADH). Thermal injury to the portal vein was characterized by loss of endothelial lining and the presence of oedema in the muscle layer on H&E staining (Figure 4a) and loss of oxidative enzyme activity in the endothelial layer along with patchy preservation of smooth muscle on NADH staining (Figure 4b).
Figure 3. Normal portal vein. a. H&E stain
(magnification x20). Muscularized vein with
preservation of endothelial lining. b. NADH stain
(magnification x20). Preservation of oxidative enzyme
activity in the endothelium and smooth muscle.
Figure 4. Ablated portal vein. a. H&E stain
(magnification x20). Loss of endothelial lining and
presence of oedema in the muscle layer. b. NADH
stains (magnification x20). Loss of oxidative enzyme
activity in the endothelial layer and patchy preservation
of smooth muscle.
At a target temperature of 90°C for 10 minutes, pancreatic ablation was complete and there was no damage to the portal vein, but thermal injury to the bile duct was evident in one animal. The target temperature of 80°C was associated with evidence of ablation in 2 of 5 (40%) of animals.
Effects of Variation in Duration of Ablation
At 80°C increase in the duration of ablation from 10 to 15 minutes was associated with evidence of ablation in 3 (60%) as compared to 2 (40%) animals. The additional duration of ablation was not associated with any evidence of injury to peri-pancreatic structures. A shorter duration of ablation was also examined. For these experiments 90°C was selected as this was the lowest temperature associated with consistent evidence of ablation. This combination of temperature/duration of ablation was associated with complete ablation in all 5 animals with no evidence of injury to peripancreatic structures. The duodenum was unaffected in all experiments on both H&E and NADH (figures 5a and 5b). At all temperatures, all layers including mucosa, muscularis mucosa, Brunner’s glands and muscularis propria were well preserved.
Figure 5. Normal duodenum. a. H&E stain
(magnification x4). All the layers including mucosa,
muscularis mucosa, Brunner’s glands and muscularis
propria are well preserved. b. NADH stains
(magnification x4). All the layers including mucosa,
muscularis mucosa, Brunner’s glands and muscularis
propria show preservation of oxidative enzyme
activity.
Effects of Simulated Portal Perfusion
Complete ablation was noted in all the 5 animals with portal perfusion at the target temperature of 90°C and duration of 10 minutes (Table 2). Thermal injury to the portal vein was not seen in any animal. These results were not different from those in animals without simulated portal circulation.

DISCUSSION
Although the practice of thermal ablation of solid tumours is now well-established, there are well-recognised site-specific risks associated with ablation of pancreatic tumours. Any injury to the duodenum, bile duct or portal vein in a patient with nonresectable disease may lead to a lethal outcome. In order to explore the feasibility of radiofrequency ablation of the pancreas this study has evaluated the thermal kinetic profile of the ablation effect. At the outset, it must be emphasised that these results apply to an exvivo, non-tumour bearing, porcine model and that direct extrapolation of these results to man is not possible. However, when set in the context of the complete dearth of information on radiofrequency ablation of the pancreas in man, the results of the studies provide some guidance. First, the relation between target temperature and effect of ablation mirrors the effects seen in human liver tumours. Specifically, the optimal temperature for ablation of hepatic parenchymal tumours in man is 90°C and this derives from ex-vivo hepatic studies.
The optimum duration of ablation in clinical practice will be determined by the size of the tumour. In practice, small tumours (less than 3 cm) are likely to be resected and thus ablation will see clinical use in larger nonresectable pancreatic tumours where a more prolonged ablation time may be required. This study establishes that in an ex-vivo setting a minimal duration of 5 minutes is required to produce a 2 cm ablation. Thermal ablation is function of the intrinsic properties of the tissue and extrinsic thermal kinetic parameters. The main intrinsic factors affecting the effectiveness of ablation are tissue impedance and the proximity of large calibre vessels causing ‘heat sink’. It is well recognised that simulation of portal vein flow in an ex-vivo setting is problematic: flow rates of 1,500 mL/min seen in man cannot readily be duplicated. Ideally, an in-vivo animal experimentation setting should be used for this type of study but there is no large animal model of pancreatic cancer. In this study, the presence of flow in the portal vein did not affect ablation nor was there any effect of ablation on the portal vein. In conclusion, this study establishes that at temperature settings comparable to those currently in use for the ablation of human liver tumours, radiofrequency ablation produces consistent evidence of injury to pancreatic parenchyma in this ex-vivo porcine model. As in the clinical setting, the ablation is temperature and duration-dependent and in this model, an optimal temperature of 90°C for 5 minutes resulted in ablation of parenchyma with sparing of important peri-pancreatic structures.
Acknowledgement
Rita Medical Systems (Mountain View, CA, USA) provided partial financial support by providing the probes used in this study. We acknowledge the help of our colleague Mr Rory McCloy who provided us with the use of the Wolfson laboratory suite
References
- Venbrux AC, Montague BJ, Murphy KPJ, Bobonis LA, Washington SB, Soltes AP, Frassica FJ. Imageguided percutaneous radiofrequency ablation for osteoid osteomas. J VascIntervRadiol 2003; 14:375- 80. [PMID 12631644]
- Anzai Y, Lufkin R, DeSalles A, Hamilton DR,Farahani K, Black KL. Preliminary experience withMR guided thermal ablation of brain tumours. AJNRAm J Neuroradiol 1995; 16:39-48. [PMID 7900601]
- Rosenthal DI, Hornicek FJ, Torriani M, GebhardtMC, Mankin HJ. Osteoid osteoma: percutaneoustreatment with radiofrequency energy. Radiology 2003;229:171-5. [PMID 12944597]
- Decadt B, Siriwardena AK. Radiofrequencyablation of liver tumours: systematic review. LancetOncol 2004; 5:550-60. [PMID 15337485]
- Lam CM, Ng KKC, Poon RTP, Ai V, Yuen J, FanST. Impact of radiofrequency ablation on themanagement of patients with hepatocellular carcinomain a specialized centre. Br J Surg 2004; 91:334-8.[PMID 14991635]
- Date RS, Biggins J, Paterson I, Denton J,Mcmahon RF, Siriwardena AK. Development andvalidation of an experimental model for the assessmentof radiofrequency ablation of pancreatic parenchyma.Pancreas 2005; 30:266-71. [PMID 15782106]






