Keywords
Palliative Care; Pancreatic Neoplasms; Quality of Life
Abbreviations
MDASI: M.D. Anderson Symptom Inventory; QoL: quality of life
Pancreatic Cancer and Quality of Life
Pancreatic cancer is the fourth leading cause of cancer death in the United States. Its prognosis remains poor despite advances in surgery, radiation therapy, and chemotherapy [1]. As pancreatic cancer often presents insidiously, the majority of patients are not diagnosed until they have advanced or metastatic disease. For the 20% of patients who can undergo curative resection, even with clear margins, the 5-year survival rate is only 10-25%. Therefore, much of pancreatic cancer management is aimed at palliation of symptoms. Common symptoms include pain, fatigue, malabsorption, cachexia, obstruction (both intestinal and biliary), and thromboembolism. Though treatment with surgery, radiation, and chemotherapy may help to improve morbidity, the toxicities from treatments can also add to the symptom profile, which should always be taken into consideration. For example, when gemcitabine was approved in the mid 1990s it showed only a modest survival benefit; however, 23.8% of patients showed improvement in terms of clinical benefit response (which takes into account pain, weight, and performance status) [2]. Supportive management of symptoms must be initiated early and aggressively to ensure patient comfort [3].
In addition to evaluating methods for symptom management, there has been interest as to how identification of symptoms may aid in prognostication. Several studies have shown that baseline quality of life (QoL) measures are associated with survival in pancreatic cancer [4, 5]. Bernard et al. [6] observed that baseline patient-rated pain and tiredness were predictors of survival, though less significant than CA 19-9 tumor marker levels. Though only some of these studies have shown statistical significance, these measures may help to provide additional information to guide patient care. Tumor markers may benefit from supplementation by measures of QoL which can additionally take into consideration the patient’s perception of their situation as a whole (including both pathophysiological and emotional wellbeing).
What Did We Learn at the 2012 ASCO Gastrointestinal Cancers Symposium?
Here, we review a few of the studies presented at the 2012 ASCO Gastrointestinal Cancers Symposium that address symptom identification and how they may help improve pancreatic cancer management.
Identification of Common Symptoms in Patients with Advanced Pancreatic Cancer Undergoing Gemcitabine-Based Chemotherapy (Abstract #370 [7])
Wang et al. evaluated the correlation between patientreported symptoms, disease burden and treatment duration in patients with advanced pancreatic cancer undergoing gemcitabine-based chemotherapy [7]. They evaluated 100 patients undergoing chemotherapy with the MD Anderson Symptom Inventory (MDASI) (Table 1). Common symptoms include pain, fatigue, and loss of appetite. Of particular interest, is that patients who ended treatment earlier (before 9 weeks) suffered more pain at baseline and had persistently worse symptoms. The authors suggest that more severe symptoms reported by patients may be associated with greater disease burden, and a higher likelihood to stop treatment earlier.

Symptoms as Predictors of Disease Control (Abstract #195 [8])
A Japanese study by Kuwahara et al aimed to determine symptom changes that could predict disease control [8]. The study included 87 patients with treatment naïve, unresectable pancreatic tumors. The patients received gemcitabine monotherapy (n=42), gemcitabine-based chemotherapies (n=41), or S-1 monotherapy (n=4). The patient’s symptoms were scored using a Japanese modified version of the MDASI prior to initiation of treatment and one month later. The tumor responses were assessed using the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.0. They found that patients without worsening of pain or sleep symptoms had higher frequency of disease control, though this only reached significance for sleep disturbance (P=0.004). This is consistent with the theory of Wang et al. [7] that diminished pain on presentation may be indicative of small tumor burden. This study is a helpful complement to ongoing research evaluating the utilization of symptoms as prognostic signs for treatment success and mortality. Gemcitabine has appeared in many studies to improve pain control, but there has been considerable debate as to its impact on overall QoL measures. Romanus et al. addressed this discrepancy, and their results suggest that this may, in part, be due to the use of different tools measuring QoL [9]; therefore, addressing specific symptoms like pain may provide more appropriate reproducibility.
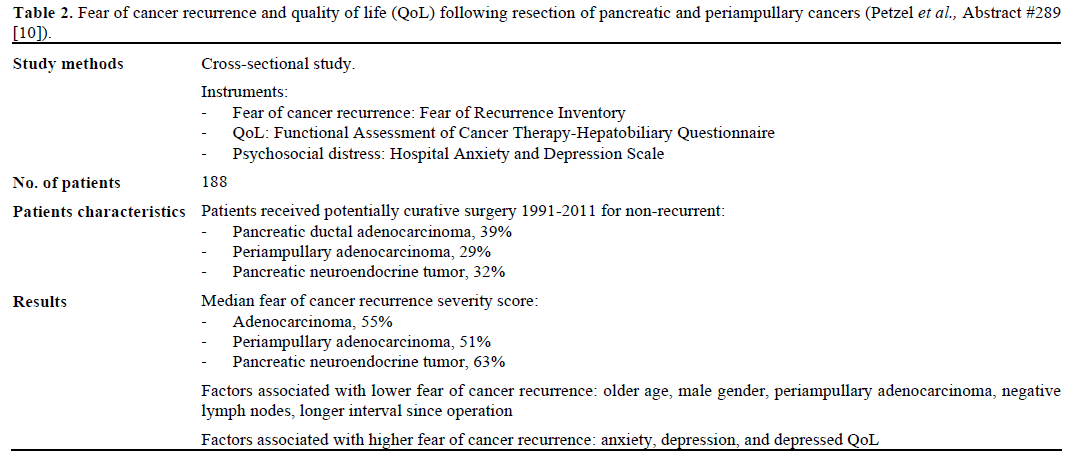
Fear of Cancer Recurrence (Abstract #289 [10])
The symptoms suffered by patients, however, are not only physical in nature, but can also play heavily on their emotional wellbeing. Fear of cancer recurrence has been a stressor studied extensively in cancers with better long-term prognosis, such as breast, prostate, and colon cancer [11]. Petzel et al. [10] evaluated this concern in 188 patients who underwent potentially curative surgery for non-recurrent pancreatic ductal adenocarcinoma, periampullary adenocarcinoma, or pancreatic neuroendocrine tumors (Table 2). All three histologic types had rates of fear of cancer recurrence greater than 50%.
Though these patients are considered successes in a field with such high mortality, this study demonstrates that other symptomatic targets, including those of psychosocial etiology, should be further addressed to provide better support for our patients.
Discussion
Due to pancreatic cancer’s dismal prognosis, much of management is focused upon palliation and symptom management, and the decision to treat a patient with more aggressive maneuvers must always take into account the impact upon a patient’s QoL. However, these three studies present how identification of these symptoms may also change treatment adherence, disease prognosis, or emotional wellbeing. Wang et al. [7] showed a correlation between self-reported pain and early termination of treatment. Though a causal relationship cannot be specifically identified, it is possible that these symptoms either identify a more atrisk population for early drop out, a population that requires better targeting of pain control, or a subgroup with higher disease burden that is less likely to attain disease control. The last theory is particularly consistent with Kuwahara et al. [8] who found that patients with disease control had greater improvement of pain and sleep disturbance scores; suggesting that patient symptoms might be utilized in addition to other markers as indicators of treatment success. The abstract of Petzel et al. [10] also highlighted how other stressors, such as fear of cancer recurrence, anxiety, and depression are also part of QoL measures, and that causes of emotional anxiety must also be taken into consideration when attempting to provide the best care for a patient.
Therefore, when evaluating patients in the clinic setting it will be important to evaluate the patient as a whole and to seek the patients’ self-perception of their symptoms. Patients and their families will be best served by a multidisciplinary team, where oncologist, radiation oncologist, surgeon, nutritionist, psychiatrist and others work together to create a plan which provides comprehensive support for the patient. In the future, this can help improve treatment, adherence, and with future studies, may identify prognostic factors that will better prepare patients and physicians for the natural course of their disease.
Conflict of interest
The authors have no potential conflicts of interest
References
- American Cancer Society. Cancer Facts & Figures 2012. Atlanta: American Cancer Society 2012.
- Burris HA, Moore MJ, Andersen J et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J ClinOncol 1997; 15: 2403-2413. [PMID 9196156]
- Fazal S, Saif MW. Supportive and palliative care of pancreatic cancer. JOP 2007; 8: 240-253. [PMID 17356251]
- Gupta D, Lis CG, Grutsch JF. The European organization for research and treatment of cancer quality of life questionnaire: implications for prognosis in pancreatic cancer. Int J Gastrointest Cancer 2006; 37: 65-73. [PMID 17827524]
- Lis CG, Gupta D, Grutsch JF. Patient satisfaction with quality of life as a predictor of survival in pancreatic cancer. Int J Gastrointest Cancer 2006; 37: 35-44. [PMID 17290079]
- Bernhard J, Dietrich D, Glimelius B et al. Estimating prognosis and palliation based on tumour marker CA 19-9 and quality of life indicators in patients with advanced pancreatic cancer receiving chemotherapy. Br J Cancer 2010; 103: 1318-1324. [PMID 20877359]
- Wang XS, Fogelman DR, Shi Q et al. Patient-reported symptoms from patients with advanced pancreatic cancer undergoing gemcitabine-based chemotherapy. J ClinOncol 2012; 30: Suppl 4; abstr 370.
- Kuwahara A, Mitsunaga S, Ohno I et al. Symptom change that predict disease control by systemic chemotherapy in patients with advanced pancreatic cancer. J ClinOncol 2012; 30: suppl 4; abstr 195.
- Romanus D, Kindler HL, Archer L et al. Does Health-Related Quality of Life Improve for Advanced Pancreatic Cancer Patients Who Respond to Gemcitabine? Analysis of a Randomized Phase III Trial of the Cancer and Leukemia Group B (CALGB 80303). J Pain Symptom Manage 2012; 43: 205-217. [PMID 22104618]
- Petzel MQB, Parker NH, Valentine AD et al. Fear of cancer recurrence and quality of life among survivors of pancreatic and periampullary neoplasms. J ClinOncol 2012; 30: Suppl 4; Abstr 289.
- Koch L, Jansen L, Brenner H, Arndt V. Fear of recurrence and disease progression in long-term (>/=5 years) cancer survivors-a systematic review of quantitative studies. Psychooncology 2012. [PMID 22232030]

