Keywords
Outcome Assessment; Pancreas; Pancreatoduodenectomy
INTRODUCTION
Pancreatoduodenectomy (PD), the only curative surgery for cancer of the periampullary and pancreatic head region, is a technically challenging procedure with the risk of morbidity and mortality. The incidence of pancreatic cancer is rising [1] and it is projected to be the second most-common cause of cancer-related deaths by 2030 [2]. Thus, treatment of this cancer needs attention from global perspective. PD has evolved tremendously over the last few decades [3] initially from a life threatening, two-stage surgery to a singlestage procedure with steadily reducing operating times, the requirement for perioperative blood transfusion [4] as well as post-operative morbidity and mortality [5]. Encouraged by these improvements, there is a drive towards making PD not only more ‘patient-friendly’, but also cost effective [6, 7].
With the looming fear of costs for cancer care escalating over the next decade [8], the general aim of policy makers the world over is directing efforts towards “bending the cost curve” [9-11]. Unfortunately, in this endeavor, instead of focusing on the costs of treating individual patients with specific medical conditions over their full cycle of care, providers aggregate and analyze costs at the specialty or service department level [12]. In this case, efforts aimed at cost containment must ensure that in an attempt at reducing costs, the quality of care and the surgery are, in themselves, not compromised. The situation is compounded in solid organ cancers such as pancreatic cancer, where surgery is the mainstay for cure [13]. On this background, pancreatic surgeons have begun to assess the health economics of PD [6, 14].
Thus, the aim of the current report is to analyze the published literature on data addressing the issue of costs in pancreatic cancer surgery (with a focus on PD) in an effort to determine how disparate are the lines of investigation of health economics and quality indicators of surgery.
Literature Search
A systematic and comprehensive search of major reference databases (MEDLINE, EMBASE, PubMed, and the Cochrane Library) was undertaken using a combination of text words “cost”, “pancreatoduodenectomy”, “pancreaticoduodenectomy”, “health care”, “surgery”. The search was restricted to human studies published in literature but was not language restricted. Articles were compiled into a database and duplicates were removed. The abstracts were then screened for relevance. Subsequently, the reference lists of relevant trials, reviews, and international guidelines were hand-searched. Reference lists of the retrieved literature were cross-searched manually for additional publications. The inclusion criteria were all types of study (randomized, prospective observational, and retrospective observational) describing the analysis of factors influencing costs in PD. The articles that did not report on the factors influencing costs were excluded. Review articles, letters to the editor, comments and editorials were also excluded.
Results
The search yielded 116 studies of which 25 manuscripts [6, 14-37] were retrieved for further evaluation. Of the 25 studies retrieved, 7 manuscripts [31-37] were excluded from the final analysis as the variables analyzed did not significantly influence the costs of PD (Figure 1).
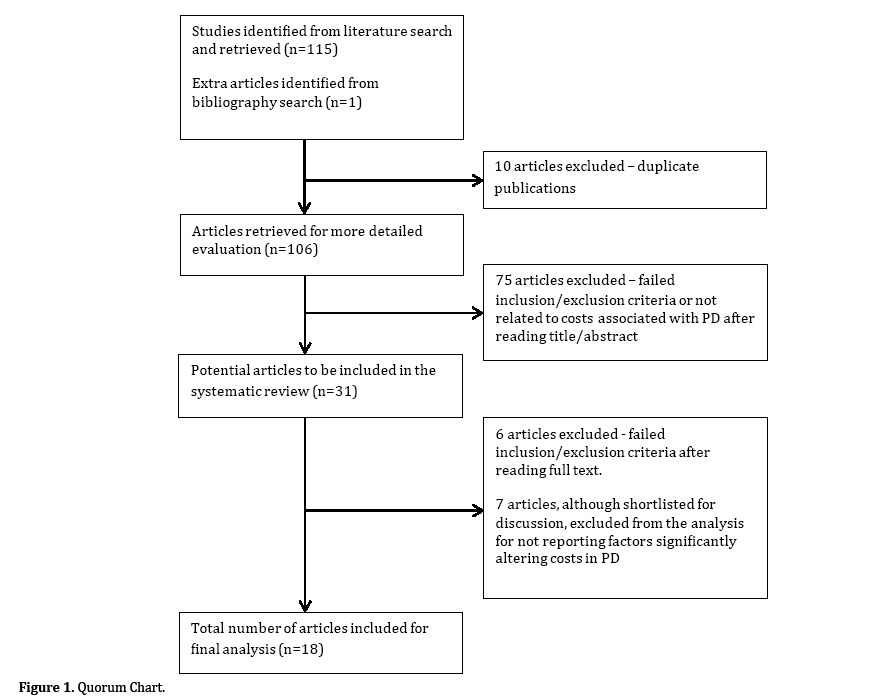
Figure 1. Quorum Chart.
Table 1 summarizes the 18 studies that includes 35,322 patients (patients from multiple publications by the same authors [6, 25] included in the current analysis were excluded if they could be clearly accounted for). The majority of the studies were based on multicentre data analyses from the United States (7 studies) with an additional 5 single centre studies from the same country. Two studies reported data from a single centre in Italy while the only study from Japan was a multicentre analysis. There are also single studies from Belgium, The Netherlands and China.

The factors most frequently noted (≥2 studies) to influence costs of PD were hospital [18, 19, 25, 27, 30] and surgeon volume [18, 20, 24], the occurrence of complications [17, 21, 26] and the implementation of clinical pathways [6, 23]. Low surgeon and hospital volumes were associated with significantly increased hospital costs as was the occurrence of post-operative complications. Costs escalated with the rising severity of the complication [17, 26], the development of post-operative infections [17, 26] or post operative pancreatic fistula (POPF) [14, 16, 17]. The implementation of perioperative clinical pathways was associated with reduced hospital costs.
Other factors noted to significantly increase PDassociated hospital costs included a higher American Society of Anesthesiologists (ASA) grade [22], complications such as medical complications [17], delayed gastric emptying (DGE) [17], post-pancreatectomy hemorrhage (PPH) [26], bile leak [17], and the need for resurgery for the complications [17], length of post-operative hospital stay [14], surgery for malignancies other than pancreatic ductal adenocarcinoma [26], the performance of laparoscopic PD [28] and the delayed removal of peroperatively placed intra-abdominal drains [15].
On the other hand, regionalization of the performance of PD [19] and selective use of the somatostatin analogue, octreotide, in high risk patients [29] significantly reduced total costs o fPD.
The studies not included in the review that addressed factors suspected to alter costs but, on analysis, failed to do so are mentioned below. Elderly patients with their higher propensity for co-morbidities as well as post-operative complications [38] have been thought to incur higher costs should they need PD. However, all 3 studies addressing the aspect of PD in elderly [35-37], found no significant differences in terms of the cost. Studies investigating the use of energy devices for dissection in PD (suggested to reduce operative times and consequently surgical costs) failed to reduce total costs [32, 33]. Similarly, laparoscopic PD costs were not found to be significantly different from open surgery in an analysis of 123 patients (75 of whom underwent laparoscopic PD) [31] which the authors attributed to the shortened hospital stay using the minimally invasive approach. Selective use of diagnostic laparoscopy in pancreatic cancer, too, failed to show a significant impact on total costs [34]. No difference in the impact of the pathology for which PD was performed (neoplasm versus chronic pancreatitis) was noted in the analysis by Holbrook et al. [21].
Reducing Costs and PD – The Way Forward
The manner in which Healthcare costs are borne vary in different parts of the world. The three most common stake holders in bearing cancer-therapy related costs are the patients themselves [39] (self funded - who pay ‘out of pocket’), the Health Insurance companies, and the National health care systems such as the National Institute of Health (NIH) in the United States, the Medicare in Australia and the National Health Service (NHS) in the United Kingdom. The financial burden to the patient even in the case of existing comprehensive health insurance policies [40] or state plans [41], is immense. Reduction in costs would as a rule benefit all the above stake holders and most certainly the patient. However, we must not lose focus of the fact that cost is not the most important aspect of patient care.
In order to understand the factors influencing costs following surgery performed with a curative intent, we reviewed the published data on costs associated with PD – the surgical treatment for periampullary and pancreatic head cancer. This review, the first of its kind, highlights various factors that influence costs following PD, the most prominent being hospital and surgeon volume, the occurrence of complications, and the implementation of clinical pathways.
Interestingly, pancreatic surgeons have long-been challenging themselves in attempting to continuously improve procedural outcomes. From acknowledging the impact of surgeon [42] and hospital volume [43] on perioperative outcomes leading to the drive towards centralization / regionalization of pancreatic surgery [44] to developing quality indicators for not only overall post-operative morbidity (<55%) and mortality (<5%) but even specific complications such as POPF (<16%) [45] there has been a constant thrust towards achieving better results overall. The initial belief that higher hospital or surgeon volumes correlate with better outcomes was critically analyzed [46]. This analysis by Ghaferi et al. [46] determined that that the difference in mortality between high- and low-volume centers was not so much a result of reduced morbidity as it was the ability of these high-volume centers to effectively manage the complications or what was described as low ‘failure to rescue rates’.
Further taking cues from the successful implementation of enhanced recovery protocols following surgery in other subspecialties [47, 48], pancreatic surgeons have attempted to develop and implement clinical pathways following PD [49-51]. This, too, has shown not only to reduce hospital stay, but also costs [6, 23].
Morbidity following PD has remained one of the most stubborn statistics that has dogged pancreatic surgeons. The most common complications following PD include POPF, PPH and DGE. In this regard, surgeons have tried to systematically address these complications. The International Study Group for Pancreatic surgery (ISGPS) has provided evidence-based definitions for each of these entities [52-54] to ensure uniformity of their expression and comparability of data between centers and studies. The underlying risk factors for the development of POPF are the texture of the pancreatic gland and the diameter of the pancreatic duct. A soft, fat infiltrated gland with a small duct diameter (≤3 mm) is associated with a high risk of POPF [55, 56]. Thus, over the last few decades pancreatic surgeons have tried various techniques to tailor the strategy of the pancreaticoenteric anastomosis to the risk factors. Certain factors have been identified to help in reducing the risk such as the use of stents [57] and the use of octreotide. Octreotide has been used by some surgeons in the perioperative period with some evidence to suggest a reduction in the incidence of POPF [58]. This may be the reason for the reduced costs noted in patients who were selectively treated with octreotide [29]. As for the type of anastomosis, despite a fair amount of clinical research into this aspect [59] there remains work to be done to identify the best anastomosis for a particular gland texture. However, standardization of the technique employed by surgeons has been shown to reduce the risk of POPF [60]. The incidence of DGE has been suggested to be influenced by the location of the gastro-/duodenojejunostomy (antecolic versus retrocolic). However, the appropriate technique remains to be determined [61]. The placement of intra-abdominal drains during PD has been the focus of various studies. The rationale [62] behind abdominal drainage has been the value afforded by drains in forewarning the surgeon of potential intraabdominal complications [63] without putting the patient at risk of complications of the drain such as local pain, ascending infection via the drain [64, 65], and interference with patient ambulation. The issue of routine peritoneal drainage following PD suggests reduced risk of morbidity with routine drainage [66]. However, these drains must be removed as soon as possible [67] once sinister complications can be safely ruled out.
Minimally invasive PD was introduced with an aim to reduce the morbidity associated with the large incision utilized in open PD as well owing to its ability to improve vision during dissection. However, an analysis of a large cohort of patients has indicated that minimally invasive PD for cancer has been found to be associated with an increased 30-day mortality [68] and thus comprehensive protocols outlining criteria for implementation are warranted to optimize patient safety.

Thus, from the above analysis two things emerge, viz. factors influencing total hospital costs for PD are in essence markers of surgical quality and secondly, these factors can only be addressed by a true scientific approach and appraisal of the literature. Thus, rather than implementing cost-cutting measures such as across-the-board cuts in expensive services, staff compensation, and head count [12], focusing on improving the quality of surgery and care, itself, are potentially the best strategies to guarantee reduced costs. There are numerous methodologies to critically analyze processes and implement changes for improving outcomes. The author has previously suggested ways in which clinicians can utilize process excellence tools such as the Six Sigma methodology [69] with an aim to improving outcomes of hepatopancreatobiliary surgery and more specifically pancreaticoenteric anastomosis in PD [57]. This is just one of the many tools available. Either way, the bottom line is to reduce costs, we must improve quality!
Conclusion
Using PD, as an example, it is evident that the key to ‘bending the cancer cost curve’ is designing strategies to improve quality of the not only the procedure, but the process. Costs and quality cannot be separated. Reduction in costs can, and must only, be achieved by targeting excellence.
Conflict of Interests
Authors declare no conflict of interests for this article.
References
- Simard EP, Ward EM, Siegel R, Jemal A: Cancers with increasing incidence trends in the united states: 199 through 200. CA Cancer J Clin 201;6:11-12.
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM: Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the united states. Cancer Res 201;:291-2.
- Shukla P, Barreto S, Shrikhande S: The evolution of pancreatoduodenectomy. Hepatogastroenterology 2011
- Ball C, Pitt H, Kilbane M, Dixon E, Sutherland F, Lillemoe K: Peri-operative blood transfusion and operative time are quality indicators for pancreatoduodenectomy. HPB (Oxford) 2010;1:46-4.
- Shrikhande SV, Barreto SG, Somashekar BA, Suradkar K, Shetty GS, Talole S, Sirohi B, Goel M, Shukla PJ: Evolution of pancreatoduodenectomy in a tertiary cancer center in india: Improved results from service reconfiguration. Pancreatology 201;1:6-.
- Vanounou T, Pratt W, Fischer JE, Vollmer CM, Jr., Callery MP: Deviation-based cost modeling: A novel model to evaluate the clinical and economic impact of clinical pathways. J Am Coll Surg 200;20:570-57.
- Kennedy EP, Rosato EL, Sauter PK, Rosenberg LM, Doria C, Marino IR, Chojnacki KA, Berger AC, Yeo CJ: Initiation of a critical pathway for pancreaticoduodenectomy at an academic institution--the first step in multidisciplinary team building. J Am Coll Surg 200;20:91-92; discussion 92-91.
- 8Mariotto AB, Yabroff KR, Shao Y, Feuer EJ, Brown ML: Projections of the cost of cancer care in the united states: 2010-2020. J Natl Cancer Inst 201;10:11-12.
- Good M, Good CB: Bending the cost curve in cancer care. N Engl J Med 201;36:6-6; author reply 6-6.
- Field K, Faragher I, Gibbs P: Bending the cost curve in cancer care. N Engl J Med 201;36:6; author reply 6-6.
- Smith TJ, Hillner BE: Bending the cost curve in cancer care. N Engl J Med 201;36:2060-206.
- Kaplan RS, Porter ME: How to solve the cost crisis in health care. Harv Bus Rev 201;8:-, , -6passim.
- Shrikhande S, Barreto S: Surgery for pancreatic carcinoma: State of the art. Indian J Surg 201;:7-.
- Topal B, Peeters G, Vandeweyer H, Aerts R, Penninckx F: Hospital cost-categories of pancreaticoduodenectomy. Acta Chir Belg 200;10:3-37.
- Bassi C, Molinari E, Malleo G, Crippa S, Butturini G, Salvia R, Talamini G, Pederzoli P: Early versus late drain removal after standard pancreatic resections: Results of a prospective randomized trial. Ann Surg 2010;2:20-21.
- Daskalaki D, Butturini G, Molinari E, Crippa S, Pederzoli P, Bassi C: A grading system can predict clinical and economic outcomes of pancreatic fistula after pancreaticoduodenectomy: Results in 75consecutive patients. Langenbecks Arch Surg 201;3:-.
- Enestvedt CK, Diggs BS, Cassera MA, Hammill C, Hansen PD, Wolf RF: Complications nearly double the cost of care after pancreaticoduodenectomy. Am J Surg 201;20:3-33.
- Enomoto LM, Gusani NJ, Dillon PW, Hollenbeak CS: Impact of surgeon and hospital volume on mortality, length of stay, and cost of pancreaticoduodenectomy. J Gastrointest Surg 201;1:690-700.
- Gordon TA, Burleyson GP, Tielsch JM, Cameron JL: The effects of regionalization on cost and outcome for one general high-risk surgical procedure. Ann Surg 19;2:-4.
- Ho V, Aloia T: Hospital volume, surgeon volume, and patient costs for cancer surgery. Med Care 200;:71-72.
- Holbrook RF, Hargrave K, Traverso LW: A prospective cost analysis of pancreatoduodenectomy. Am J Surg 19;1:50-51.
- Kennedy TJ, Cassera MA, Wolf R, Swanstrom LL, Hansen PD: Surgeon volume versus morbidity and cost in patients undergoing pancreaticoduodenectomy in an academic community medical center. J Gastrointest Surg 2010;1:1990-19.
- Porter GA, Pisters PW, Mansyur C, Bisanz A, Reyna K, Stanford P, Lee JE, Evans DB: Cost and utilization impact of a clinical pathway for patients undergoing pancreaticoduodenectomy. Ann Surg Oncol 2000;:4-48.
- Rosemurgy A, Cowgill S, Coe B, Thomas A, Al-Saadi S, Goldin S, Zervos E: Frequency with which surgeons undertake pancreaticoduodenectomy continues to determine length of stay, hospital charges, and in-hospital mortality. J Gastrointest Surg 200;1:4-44.
- Rosemurgy AS, Bloomston M, Serafini FM, Coon B, Murr MM, Carey LC: Frequency with which surgeons undertake pancreaticoduodenectomy determines length of stay, hospital charges, and in-hospital mortality. J Gastrointest Surg 200;:-.
- Santema T, Visser A, Busch O, Dijkgraaf M, Goslings J, Gouma D, Ubbink D: Hospital costs of complications after a pancreatoduodenectomy. HPB (Oxford) 2015
- Sutton JM, Wilson GC, Paquette IM, Wima K, Hanseman DJ, Quillin RC, 3rd, Sussman JJ, Edwards MJ, Ahmad SA, Shah SA, Abbott DE: Cost effectiveness after a pancreaticoduodenectomy: Bolstering the volume argument. HPB (Oxford) 201;:10-106.
- Tan CL, Zhang H, Peng B, Li KZ: Outcome and costs of laparoscopic pancreaticoduodenectomy during the initial learning curve vs laparotomy. World J Gastroenterol 201;:531-531.
- Vanounou T, Pratt WB, Callery MP, Vollmer CM, Jr.: Selective administration of prophylactic octreotide during pancreaticoduodenectomy: A clinical and cost-benefit analysis in low- and high-risk glands. J Am Coll Surg 200;20:-55.
- Yoshioka R, Yasunaga H, Hasegawa K, Horiguchi H, Fushimi K, Aoki T, Sakamoto Y, Sugawara Y, Kokudo N: Impact of hospital volume on hospital mortality, length of stay and total costs after pancreaticoduodenectomy. Br J Surg 201;10:52-52.
- Mesleh MG, Stauffer JA, Bowers SP, Asbun HJ: Cost analysis of open and laparoscopic pancreaticoduodenectomy: A single institution comparison. Surg Endosc 201;2:451-452.
- Eng OS, Goswami J, Moore D, Chen C, Brumbaugh J, Gannon CJ, August DA, Carpizo DR: Safety and efficacy of ligasure usage in pancreaticoduodenectomy. HPB (Oxford) 201;1:74-.
- Piccinni G, Pasculli A, D'Ambrosio E, Gurrado A, Lissidini G, Testini M: Retrospective comparison of traditional vs. Ligasure impact dissection during pancreatoduodenectomy: How to save money by using an expensive device. Surg Technol Int 201;2:8-.
- Enestvedt CK, Mayo SC, Diggs BS, Mori M, Austin DA, Shipley DK, Sheppard BC, Billingsley KG: Diagnostic laparoscopy for patients with potentially resectable pancreatic adenocarcinoma: Is it cost-effective in the current era? J Gastrointest Surg 200;1:117-11.
- Langan RC, Huang CC, Mao WR, Harris K, Chapman W, Fehring C, Oza K, Jackson PG, Jha R, Haddad N, Carroll J, Hanna J, Parker A, Al-Refaie WB, Johnson LB: Pancreaticoduodenectomy hospital resource utilization in octogenarians. Am J Surg 2015
- Langan RC, Zheng C, Harris K, Verstraete R, Al-Refaie WB, Johnson LB: Hospital-level resource use by the oldest-old for pancreaticoduodenectomy at high-volume hospitals. Surgery 201;15:36-3.
- Vickers SM, Kerby JD, Smoot TM, Shumate CR, Halpern NB, Aldrete JS, Gleysteen JJ: Economics of pancreatoduodenectomy in the elderly. Surgery 19;120:620-62; discussion 62-6.
- Sukharamwala P, Thoens J, Szuchmacher M, Smith J, DeVito P: Advanced age is a risk factor for post-operative complications and mortality after a pancreaticoduodenectomy: A meta-analysis and systematic review. HPB (Oxford) 201;1:64-65.
- Zaidi AA, Ansari TZ, Khan A: The financial burden of cancer: Estimates from patients undergoing cancer care in a tertiary care hospital. Int J Equity Health 201;1:60.
- Arozullah AM, Calhoun EA, Wolf M, Finley DK, Fitzner KA, Heckinger EA, Gorby NS, Schumock GT, Bennett CL: The financial burden of cancer: Estimates from a study of insured women with breast cancer. J Support Oncol 200;:2-27.
- Longo CJ, Fitch M, Deber RB, Williams AP: Financial and family burden associated with cancer treatment in ontario, canada. Support Care Cancer 200;1:107-10.
- Nordback L, Parviainen M, Raty S, Kuivanen H, Sand J: Resection of the head of the pancreas in finland: Effects of hospital and surgeon on short-term and long-term results. Scand J Gastroenterol 200;3:14-1460.
- Birkmeyer JD, Finlayson SR, Tosteson AN, Sharp SM, Warshaw AL, Fisher ES: Effect of hospital volume on in-hospital mortality with pancreaticoduodenectomy. Surgery 199;12:250-2.
- Gordon TA, Bowman HM, Tielsch JM, Bass EB, Burleyson GP, Cameron JL: Statewide regionalization of pancreaticoduodenectomy and its effect on in-hospital mortality. Ann Surg 19;22:-7.
- Sabater L, Garcia-Granero A, Escrig-Sos J, Gomez-Mateo Mdel C, Sastre J, Ferrandez A, Ortega J: Outcome quality standards in pancreatic oncologic surgery. Ann Surg Oncol 201;:113-11.
- Ghaferi AA, Birkmeyer JD, Dimick JB: Hospital volume and failure to rescue with high-risk surgery. Med Care 201;4:10-10.
- Bianchini C, Pelucchi S, Pastore A, Feo CV, Ciorba A: Enhanced recovery after surgery (eras) strategies: Possible advantages also for head and neck surgery patients? Eur Arch Otorhinolaryngol 2013
- Gotlib Conn L, Rotstein OD, Greco E, Tricco AC, Perrier L, Soobiah C, Moloney T: Enhanced recovery after vascular surgery: Protocol for a systematic review. Syst Rev 201;:.
- Chaudhary A, Barreto S, Talole S, Singh A, Perwaiz A, Singh T: Early discharge after pancreatoduodenectomy - what helps and what prevents? Pancreas 201;4:2-27.
- Coolsen MM, van Dam RM, van der Wilt AA, Slim K, Lassen K, Dejong CH: Systematic review and meta-analysis of enhanced recovery after pancreatic surgery with particular emphasis on pancreaticoduodenectomies. World J Surg 2013
- Lassen K, Coolsen MM, Slim K, Carli F, de Aguilar-Nascimento JE, Schafer M, Parks RW, Fearon KC, Lobo DN, Demartines N, Braga M, Ljungqvist O, Dejong CH: Guidelines for perioperative care for pancreaticoduodenectomy: Enhanced recovery after surgery (eras(r)) society recommendations. World J Surg 201;3:240-25.
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, Sarr M, Traverso W, Buchler M: Postoperative pancreatic fistula: An international study group (isgpf) definition. Surgery 200;13:-1.
- Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr MG, Traverso LW, Yeo CJ, Buchler MW: Delayed gastric emptying (dge) after pancreatic surgery: A suggested definition by the international study group of pancreatic surgery (isgps). Surgery 200;1:76-76.
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr MG, Yeo CJ, Buchler MW: Postpancreatectomy hemorrhage (pph): An international study group of pancreatic surgery (isgps) definition. Surgery 200;1:20-2.
- Shukla PJ, Barreto SG, Fingerhut A: Do transanastomotic pancreatic ductal stents after pancreatic resections improve outcomes? Pancreas 2010;3:56-56.
- Mathur A, Pitt HA, Marine M, Saxena R, Schmidt CM, Howard TJ, Nakeeb A, Zyromski NJ, Lillemoe KD: Fatty pancreas: A factor in postoperative pancreatic fistula. Ann Surg 200;2:105-106.
- Shukla PJ, Barreto SG: Can we apply the process improvement tool six sigma to enhance outcomes in hepatopancreatobiliary surgery? HPB (Oxford) 200;1:-.
- Jin K, Zhou H, Zhang J, Wang W, Sun Y, Ruan C, Hu Z, Wang Y: Systematic review and meta-analysis of somatostatin analogues in the prevention of postoperative complication after pancreaticoduodenectomy. Dig Surg 201;:1-20.
- Machado NO: Pancreatic fistula after pancreatectomy: Definitions, risk factors, preventive measures, and management-review. Int J Surg Oncol 201;201:60247.
- Shrikhande SV, Barreto G, Shukla PJ: Pancreatic fistula after pancreaticoduodenectomy: The impact of a standardized technique of pancreaticojejunostomy. Langenbecks Arch Surg 200;3:-.
- Zhou Y, Lin J, Wu L, Li B, Li H: Effect of antecolic or retrocolic reconstruction of the gastro/duodenojejunostomy on delayed gastric emptying after pancreaticoduodenectomy: A meta-analysis. BMC Gastroenterol 201;1:6.
- Shrikhande SV, Barreto SG, Shetty G, Suradkar K, Bodhankar YD, Shah SB, Goel M: Post-operative abdominal drainage following major upper gastrointestinal surgery: Single drain versus two drains. J Cancer Res Ther 201;:26-2.
- Wente MN, Shrikhande SV, Kleeff J, Muller MW, Gutt CN, Buchler MW, Friess H: Management of early hemorrhage from pancreatic anastomoses after pancreaticoduodenectomy. Dig Surg 200;2:20-20.
- Nora PF, Vanecko RM, Bransfield JJ: Prophylactic abdominal drains. Arch Surg 1;10:1-1.
- Raves JJ, Slifkin M, Diamond DL: A bacteriologic study comparing closed suction and simple conduit drainage. Am J Surg 1;14:61-620.
- Wang YC, Szatmary P, Zhu JQ, Xiong JJ, Huang W, Gomatos I, Nunes QM, Sutton R, Liu XB: Prophylactic intra-peritoneal drain placement following pancreaticoduodenectomy: A systematic review and meta-analysis. World J Gastroenterol 201;:2510-2.
- Fong ZV, Correa-Gallego C, Ferrone CR, Veillette GR, Warshaw AL, Lillemoe KD, Fernandez-Del Castillo C: Early drain removal-the middle ground between the drain versus no drain debate in patients undergoing pancreaticoduodenectomy: A prospective validation study. Ann Surg 2015
- Adam MA, Choudhury K, Dinan MA, Reed SD, Scheri RP, Blazer DG, Roman SA, Sosa JA: Minimally invasive versus open pancreaticoduodenectomy for cancer: Practice patterns and short-term outcomes among 706 patients. Ann Surg 2015
- Snee R: Six sigma: The evolution of 100 years of business improvement methodology. Int J Six Sigma Competitive Advantage 200;:-20.

