Keywords
Pancreatitis; Pulmonary Embolism
Abbrevations
PTE pulmonary thromboembolism
INTRODUCTION
Vascular complications of pancreatitis are among the causes of morbidity and mortality, common being haemorrhage into a psuedocyst, erosion of the arteries, rupture of psuedoanuerysm, venous thrombosis and formation of varices [1]. Acute pancreatitis can result into systemic inflammatory response which may lead to a number of vascular and pulmonary complications. Portosplenic and splanchnic venous thrombosis are very well described in acute pancreatitis. However extrasplanchnic involvement is less common [2], particularly pulmonary thromboembolism, being a very rarely reported complication of acute pancreatitis [3-6].
Here we report four cases of pulmonary thromboembolism in acute pancreatitis on the top of chronic pancreatitis. We found that all the patients had pancreatic ascites, its association with pulmonary embolism has been reported only in two patients in the literature up to our knowledge [3].
CASE SERIES
Case #1
A forty-six-year-old male presented with a history of moderate epigastric pain since 1 month, increased in severity since last 10 days. He developed distention of abdomen after 1 week but without jaundice and pedal edema. He started developing dyspnea on exertion and coughing in last 15 days without any chest pain. Patient was alcoholic, consumed country alcohol around 120 grams per day since 20 years and chronic tobacco chewer. Heart rate was 88/min, Blood pressure was 130/80 mmHg and no hypoxia on arterial blood gas analysis. Abdominal examination showed epigastric tenderness with presence of ascites. Liver function tests were normal with amylase of 356 IU/L (15-100 IU/L) and lipase of 560 IU/L (0-60 IU/L). On diagnostic paracentesis, there were 1100 white cells/ mm3 (80% lymphocytes), 4.3 g/dL proteins and serum albumin ascites gradient (SAAG) of 0.6. Ascitic fluid amylase was 5401 IU/L. Contrast Enhanced Computed Tomography (CECT) scan of abdomen was showing atrophic pancreas with parenchymal calcification, peripancreatic fat stranding, 3 mm pancreatic duct and multiple intraductal calculi along with ascites (Figure 1). Two Dimensional Echocardiogram (2D Echo) and Electrocardiogram (ECG) were normal. Acute thrombosis of lobar and segmental branches of bilateral pulmonary arteries was noted in CT angiography with wedge shaped bands in both lung bases consistent with lung infarcts (Figure 2). His lower limb and abdominal vessel doppler were not suggestive of any thrombus.
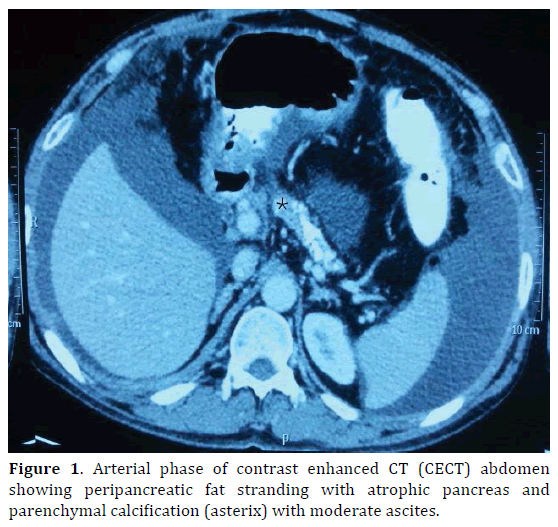
Figure 1. Arterial phase of contrast enhanced CT (CECT) abdomen showing peripancreatic fat stranding with atrophic pancreas and parenchymal calcification (asterix) with moderate ascites.
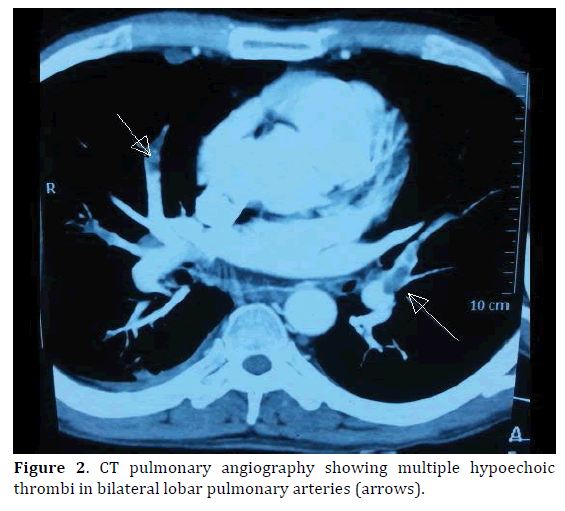
Figure 2. CT pulmonary angiography showing multiple hypoechoic thrombi in bilateral lobar pulmonary arteries (arrows).
Subcutaneous heparin was started along with analgesics and fluids. Pancreaticogram demonstrated a leak in the neck of pancreas and pancreatic duct stenting was done for the same. Ascites improved after few days. Patient shifted on oral anticoagulation and discharged at day 15.
Case #2
A thirty-year-old male, chronic alcoholic admitted to emergency department with complains of severe epigastric pain since 1 month, which was continuous, boring, radiating to back. He developed generalised abdominal distention after 5 days. He developed dyspnea on exertion before 1 week. He had similar type of severe abdominal pain before 1 year and 3 months, each time requiring hospital admission. He had multiple episodes of mild to moderate intermittent epigastric pain in 1 year, for which he used to take oral analgesics. He was alcoholic taking around 100 grams of country liquor daily since 8 years. Heart rate was 100/ minute and blood pressure was 120/70 mmHg at admission. Tachypnea was present with a rate of 25/minute but without hypoxia. Per abdomen was tender with severe ascites. Decreased air entry in both lower zones was noted on respiratory examination. Hemogram, liver enzymes and renal function tests were normal. Amylase was elevated (718 IU/L), so as lipase (400 IU/L). Diagnostic paracentesis was done, showing 135 cells, 85% neutrophils. Fluid proteins were 4.1 g/dL and amylase was 9290 IU/L. Atrophic pancreas with a leak in pancreatic duct in the body, peripancreatic edema and fat stranding were found on CECT abdomen along with ascitis. ECG had sinus tachycardia. Moderate pulmonary arterial hypertension (PAH) with dilated right atrium and ventricle were noted on 2D echo. CT pulmonary angiography (CTPA) suggested bilateral distal pulmonary artery thrombosis, extending into ascending, descending and segmental arteries (Figure 3). However, lower limb doppler was normal.
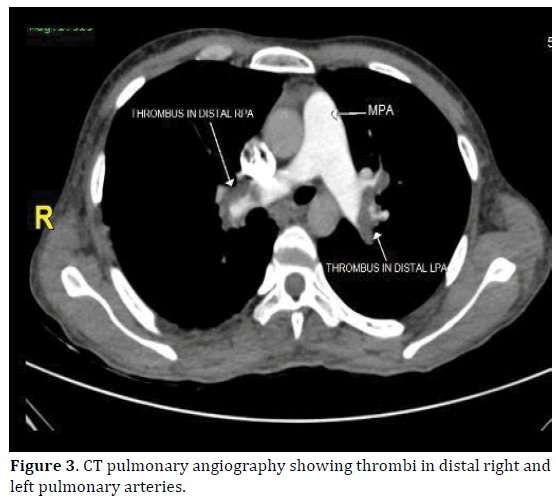
Figure 3. CT pulmonary angiography showing thrombi in distal right and left pulmonary arteries.
He was started on subcutaneous heparin and warfarin along with fluids and analgesics support. Patient improved after 15 days with conservative management.
Case #3
Thirty-eight-year-old male was hospitalised with 3 months history of severe epigastric pain, radiating to back and generalised abdominal distention and 15 days history of bilateral pedal edema. He also had dyspnea since 15 days, associated with left sided pleuritic chest pain. Patient consumed 80 grams of beer daily since last 5 years. Heart rate was 112/minute and blood pressure was 110/70 mmHg on admission. Abdomen was tender and distended with positive signs of free fluid and 5cm x 5cm bulge was palpated in epigastrium. Other systems were unremarkable. Serum amylase (1438 IU/L) and lipase (485 IU/L) were found elevated. Liver enzymes and hemogram were normal. Diagnostic ascitic tapping was done showing 3200 leucocytes / mm3 (70% polymorphs), 3.6 g/dL of proteins and SAAG of 0.7. Fluid amylase was > 10,000 IU/L. CECT abdomen was suggestive of acute necrotising pancreatitis with a large psuedocyst with portal vein and superior mesenteric vein thrombosis. Echocardiogram revealed moderate pulmonary arterial hypertension. Lower limb venous doppler suggested distal left saphenofemoral vein and popliteal vein thrombosis. To evaluate the cause for dyspnea with pleuritic chest pain, we ordered CT pulmonary angiography which showed left pulmonary artery thromboembolism with adjacent lung infarcts.
Patient was put on intravenous fluids, antibiotics and subcutaneous heparin. Symptoms decreased within a few days and patient was discharged on oral anticoagulation after 22 days.
Case #4
Thirty-five-year-old male presented with complain of severe epigastric pain since 15 days, radiating to back, followed after 3 days by abdominal distention and bilateral pedal edema, but more on left side. He had mild dyspnea since 4 days. He had an episode of acute pancreatitis with pleural effusion 3 months back. He used to drink 150 grams of country liquor since last 15 years. At admission, abdominal examination showed severe tenderness with ascites. Serum amylase was elevated (645 IU/L) with normal renal and liver function tests. Ascitic fluid examination revealed cells 250 cells/mm3 (65% lymphocytes), 1.94 g/dL protein, SAAG of 0.6, amylase of 5286 IU/L and lipase >10,000 IU/L. CECT abdomen suggested acute on chronic pancreatitis with around 4 cm psuedocyst in body communicating with pancreatic duct with ascites (Figure 4). Left sided greater saphenous vein and left anterior tibial vein were found thrombosed on doppler. Despite of normal 2D echo and electrocardiography, CT pulmonary angiography showed bilateral segmental pulmonary artery thrombosis with right sided lung infarct (Figure 5).
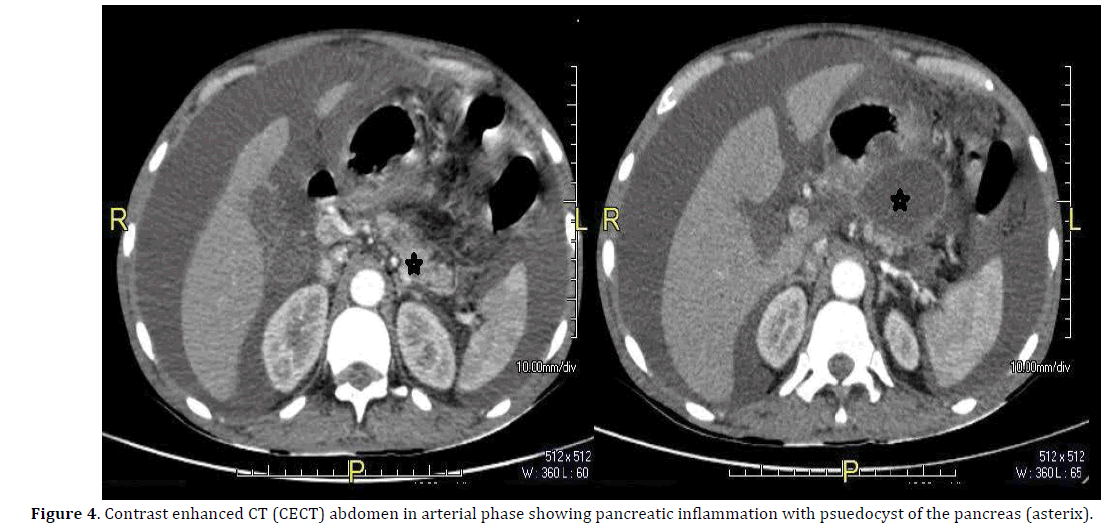
Figure 4. Contrast enhanced CT (CECT) abdomen in arterial phase showing pancreatic inflammation with psuedocyst of the pancreas (asterix).
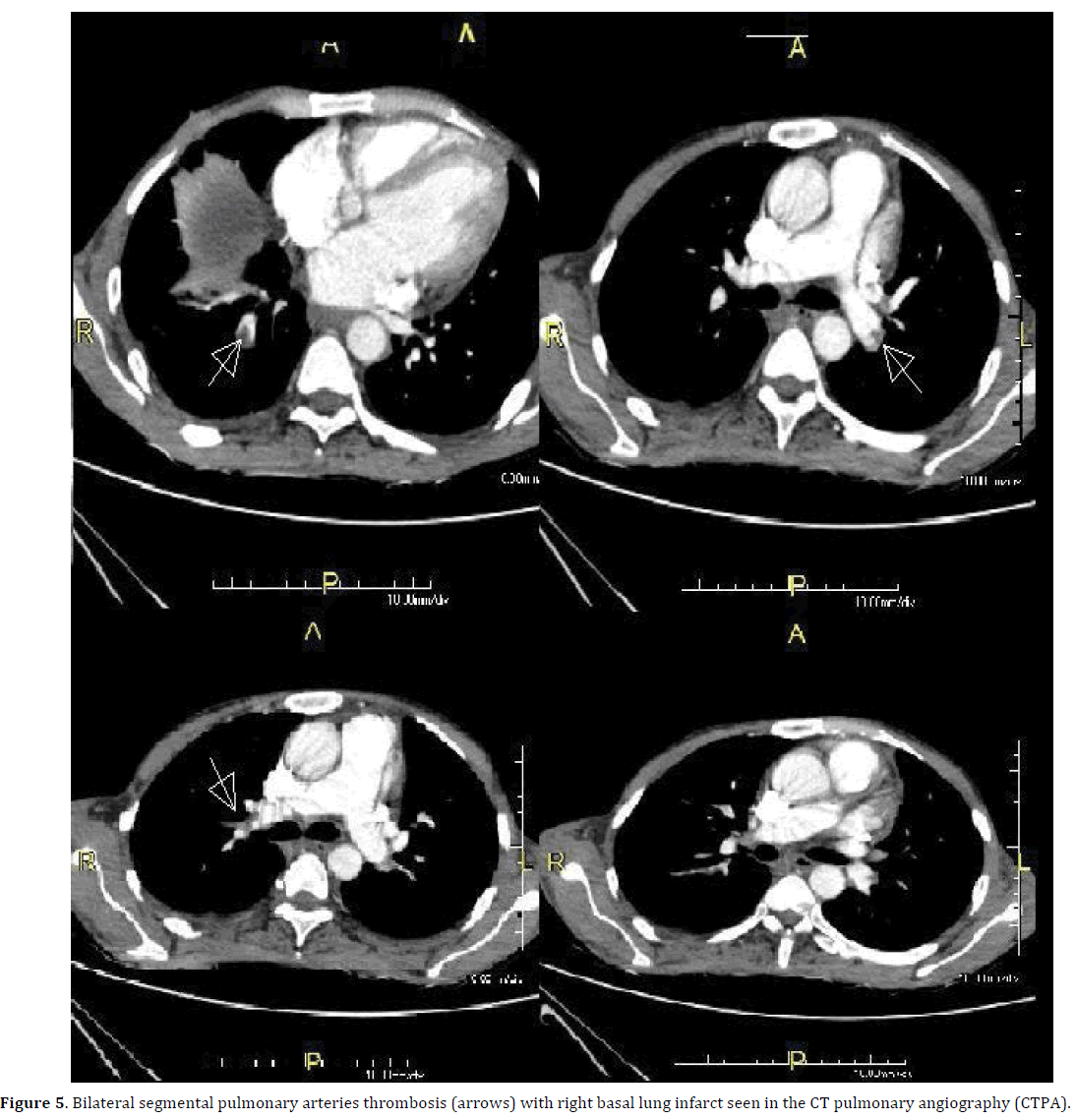
Figure 5. Bilateral segmental pulmonary arteries thrombosis (arrows) with right basal lung infarct seen in the CT pulmonary angiography (CTPA).
Patient started on heparin, intravenous octreotide and fluids. Clinical improvement seen after 10 days and discharged at day 25.
DISCUSSION
Approximately one quarter of the patients with acute and chronic pancreatitis develop vascular complications [1]. Most common are haemorrhage into a psuedocyst, erosion of the arteries, rupture of psuedoanuerysm, venous thrombosis and formation of varices. Among them, venous thrombosis is a described complication in pancreatitis, particularly in acute pancreatitis [1].
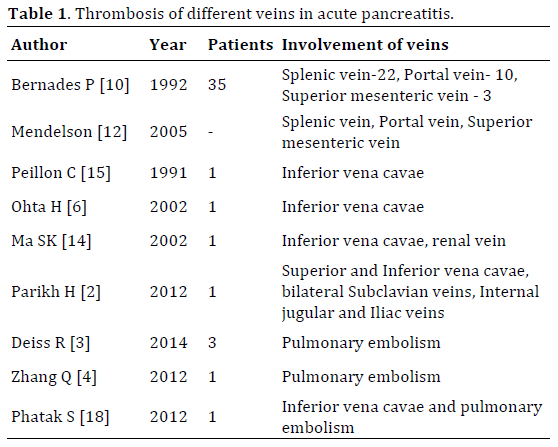
The mechanism of venous thrombosis in acute pancreatitis is often multifactorial. First and the most frequently described mechanism is the inflammatory response associated with acute pancreatitis leading to a prothrombotic state, which makes vascular events more likely. Second, involvement of the vein by surrounding edema and cellular infiltration may cause venous thrombosis [7-9]. Third, compression of the vein by a psuedocyst or enlarged pancreatic parenchyma in turn precipitates vascular event [10]. Fourth, even a rupture of cyst into a vein also precipitates thrombosis [6]. At microvascular level, the mechanism of vascular injury may be due to intrinsic endothelial damage due to inflammatory mediators [11]. Involvement of veins in vascular thrombosis is variable. Portal vein, splenic vein and superior mesenteric vein are the most commonly involved vessels [12, 13]. Other vessels involvement have also been reported (Table 1) [15].
The pathogenesis of pulmonary embolism is also multimodal. It could be either due to thrombus detached from deep leg veins or sometimes inferior vena cavae [2]. Ohta et al. and Goenka et al. have reported an association of simultaneous inferior vena cavae thrombosis and pulmonary embolism with acute pancreatitis [6, 16]. Another case of acute pancreatitis with involvement of inferior vena cavae and pulmonary arteries in antiphospholipid antibody syndrome has been published [17]. Renal vein thrombus can also eventually cause pulmonary embolism. Only 2 cases have been reported so far [6, 14]. Inferior vena cavae and renal vein thrombosis results from either compression by psuedocyst or rupture of psuedocyst [6]. In recently published case series, pulmonary thromboembolism was proposed to be related to prothrombotic effect of inflammatory cytokines in acute pancreatitis [3]. Despite of vigorous efforts, no causative mechanisms have been elucidated in some cases [4]. In an experimental study on pulmonary microvasculature in acute pancreatitis, mild pancreatitis showed abruptly terminating vessels. In more severe pancreatitis, there was substantial loss of vascular density, tortuosity, and abrupt terminations of those vessels present. This suggests that microvascular abnormalities are responsible for pulmonary infarction seen in acute pancreatitis [11].
Among four cases reported in present series, all the patients were having acute pancreatitis superimposed on chronic pancreatitis. Etiology of chronic pancreatitis was alcohol in all of them. Predominant symptoms were abdominal pain (100%) and distention of abdomen (100%). All patients were symptomatic for pulmonary embolism, while in the series reported by Deiss et al. 2 out of 3 patients were found to have embolism incidentally [3]. Two patients (50%) had deep vein thrombosis, the presumed source for pulmonary embolism. One had left anterior tibial vein thrombosis while the other had left popliteal vein thrombosis. Rest of the patients did not have any deep vein or splanchnic vein thrombosis. However, causative vein thrombus is found only in nearly 50% cases of PTE. This is similar to our observation in the present series. Intrinsic endothelial damage may have played a role for vascular event in these cases.
Surprisingly, pancreatic ascites was a common association in all four cases while 2 out of 3 patients in the series reported by Deiss et al. also had pancreatic ascites [3]. Pancreatic ascites is one of the grave complications of pancreatitis, often along with pleural effusion, responsible for 20-30% mortality rates in some studies [18]. We hypothesize that pancreatic enzymes released in the ascitic fluid could have caused severe inflammation in the systemic veins. This may trigger cytokines to cause endothelial damage and venous thrombosis and thus, pulmonary embolism. This could be one of the possible explanation for association of pancreatic ascites with PTE. However, a direct causal relationship of pancreatic ascites with pulmonary embolism is a question of ongoing research.
In conclusion, pulmonary embolism is a rare association of acute and chronic pancreatitis. We should keep a high index of suspicion for pulmonary thromboembolism in cases of acute on chronic pancreatitis with dyspnea, especially in the presence of pancreatic ascites which may confer a possible added risk for developing PTE.
Conflict of Interest
The authors declare that they have no competing interests.
References
- Mallick IH, Winslet MC. Vascular complications of pancreatitis. JOP 2004; 5:328-337. [PMID: 15365199]
- Parikh H, Shukla A, Aswani Y, Bhatia S. Multiple Extrasplanchnic Venous Thromboses: A Rare Complication of Pancreatitis. A Case Report. JOP 2012; 13: 317-9. [PMID: 22572142]
- Deiss R, Young P. Pulmonary embolism and acute pancreatitis: Case series and review.Turk J Gastroenterol2014; 25:575-7. [PMID: 25417623]
- Zhang Q, Zhang QX, Tan XP, Wang WZ, He CH, Xu L, Huang XX. Pulmonary embolism with acute pancreatitis: A case report and literature review. World J Gastroenterol 2012; 18:583-6. [PMID: 22363127]
- Asanuma Y, Furuya T, Shibata S, Shioya T, Miura M, Koyama K. Postoperative acute pulmonary thromboembolism in patients with acute necrotizing pancreatitis with special reference to apheresis therapy. TherApher 1998; 2:199-204. [PMID: 10227770]
- Ohta H, Hachiya T. A case of inferior vena cava thrombosis and pulmonary embolism secondary to acute exacerbation of chronic pancreatitis: A rare finding in radionuclide venography. Ann Nucl Med 2002; 16:147-9. [PMID: 12043910]
- Ammann RW, Akovbiantz A, Largiader F,Schueler G. Course and outcome of chronic pancreatitis. Longitudinal study of a mixed medical-surgical series of 245 patients. Gastroenterology 1984; 86:820-8. [PMID: 6706066]
- Bradley EL III. The natural history of splenic vein thrombosis due to chronic pancreatitis: indications for surgery. Int J Pancreatol 1987; 2:87-92. [PMID: 3500243]
- Lankisch PG. The spleen in inflammatory pancreatic disease. Gastroenterology 1990; 98:509-16. [PMID: 2403954]
- Bernades P, Baetz A, Levy P, Belghiti J, Menu Y, Fékété F. Splenic and portal venous obstruction in chronic pancreatitis. A prospective longitudinal study of a medical-surgical series of 266 patients. Dig Dis Sci 1992; 37:340-6. [PMID: 1735356]
- Kelly DM, McEntee GP, McGeeney KF, Fitzpatrick JM. Pulmonary microvasculature in experimental acute haemorrhagic and oedematous pancreatitis. Br J Surg 1991. [PMID: 1933186]
- Mendelson RM, Anderson J, Marshall M, Ramsay D. Vascular complications of pancreatitis. ANZ J Surg 2005; 75:1073-9. [PMID: 16398814]
- Bernades P, Baetz A, Levy P, Belghiti J, Menu Y, Fékété F. Splenic and portal venous obstruction in chronic pancreatitis. A prospective longitudinal study of a medical-surgical series of 266 patients. Dig Dis Sci 1992; 37:340-6. [PMID: 1735356]
- Ma SK, Kim SW, Kim NH, Choi KC. Renal vein and inferior vena cava thrombosis associated with acute pancreatitis. Nephron 2002; 92: 475-7. [PMID: 12218335]
- Peillon C, Manouvrier J, Testart J. Inferior vena cava thrombosis secondary to chronic pancreatitis with pseudocyst. Am J Gastroenter 1991; 86:1854-6. [PMID: 1962640]
- Goenka MK, Kochhar R, Gulati M, Singh G, Khanna SK, Mehta SK. Acute pancreatitis complicated by pulmonary thromboembolism secondary to inferior vena caval thrombosis. J ClinGastroenterol 1994; 19:85-6. [PMID: 7930445]
- Phatak S, Redkar N, Patil MA, Karnik ND. Antiphospholipid syndrome presenting as pulmonary thrombosis and pancreatitis in a young man. BMJ Case Rep 2012;2012. [PMID: 23235100]
- Fielding GA, McLatchie GR, Wilson C, Imrie CW, Carter DC. Acute pancreatitis and pancreatic fistula formation. Br J Surg 1989; 76: 1126-8. [PMID: 2597965]

