Keywords
Dysphonia/Aphonia; Vocalization; GRBAS code; Psychogenic cause; Dissociation
Introduction
This article is a clinical report on 38 patients of psychogenic dysphonia including aphonia from our clinic. Psychogenic dysphonia, particularly aphonia, is difficult to define, therefore the definition of F44.4, Dissociative Motor Disorder, Psychological Aphonia on International Classification of Diseases and Related Health Problems. Tenth revision (ICD-10) [1] is temporarily employed. In this report, dysphonia and/or aphonia are abbreviated as “dysphonia”. To date, there have been many international studies on dysphonia, the report on Minnesota Multiphasic Personality Inventory (MMPI) in 27 patients [2], clinical study in 121 cases [3], the longitudinal study of 30 patients [4], nearly 500 cases [5], the long term outcome of 40 patients [6], and the study on 28 patients [7]. However, few articles from Japan have been reported in English. Now, our study in Japan is presented internationally and the occurrence of the term “dysphonia/aphonia” is discussed.
Subjects and Methods
Thirty-eight outpatients were evaluated between April 2001 to July 2014. Their ages ranged from 21 years old to 74 years old at the time of their first visit to our clinic. Twenty-eight were females and 10 were males. During this period, the number new patients who visited our clinic was 1662. Accordingly, the incident ratio of the dysphonic patients is 2.3%, which is rather high compared with other psychiatric clinics. This may be because the otonasolaryngologist refereed many dysphonic patients to us.
The profiles of all of the patients are described in Table 1. Most of the female patients were in their late twenties to late forties, and most were in their early thirties. By contrast, most males were in their fifties. The distribution by age is shown in Figure 1.
| No |
Sex |
Age at the first visit |
Time lag of the first visit from the onset of a symptom |
Occupation: singer, professional announcer |
Course of onset |
Symptom or complication |
Opportunity or situation |
| 1 |
M |
51 |
1year |
clerk and missionary |
gradual |
hoarse voice , stuttering |
after having cold |
| 2 |
F |
31 |
6 months |
singer |
gradual |
hoarse voice, tic |
conflict in her family |
| 3 |
F |
38 |
4years and 2 months |
singer |
gradual |
hoarse voice |
conflict in her family |
| 4 |
F |
74 |
12 years |
unemployee |
gradual |
hoarse voice |
trouble in her job |
| 5 |
F |
34 |
4 ~ 5 years |
civil servant |
gradual |
aphonia, upper limb paralysis |
trouble in her job |
| 6 |
F |
35 |
15years or longer |
house wife and missionary |
sudden |
hoarse voice |
trouble in her job |
| 7 |
M |
35 |
attending our clinic |
clerk |
sudden |
hoarse voice |
death of a family member |
| 8 |
F |
59 |
attending our clinic |
house wife and ballet dancer |
sudden |
depression and hoarse voice |
conflict in her family and job |
| 9 |
F |
27 |
2 years |
clerk |
sudden |
spina bifida and hoarse voce |
trouble in her job |
| 10 |
F |
31 |
1year |
clerk and care-giver |
sudden |
headache and hoarse voice |
trouble in her job |
| 11 |
F |
62 |
2 years and 4 months |
house wife |
sudden |
hoarse voice |
conflict in her family |
| 12 |
F |
44 |
2 months |
clerk |
sudden |
paralysis of hand fingers, hoarse voice |
trouble in her job |
| 13 |
F |
25 |
3 months |
working as a volunteer |
sudden |
aphonia |
after having cold |
| 14 |
M |
39 |
6 years |
clerk |
sudden |
depression and hoarse voice |
conflict in his family |
| 15 |
F |
28 |
3months |
hostess |
gradual |
multiple personality, hoarse voice |
conflict in her family |
| 16 |
F |
23 |
7 months |
clerk |
sudden |
anxiety disorder, hoarse voice |
asthma |
| 17 |
F |
27 |
soon |
part time worker, singer |
sudden |
anxiety disorder, hoarse voice |
trouble in her job |
| 18 |
F |
46 |
soon |
perfumer |
sudden |
hoarse voice |
trouble in her job |
| 19 |
F |
58 |
1year |
hostess |
sudden |
anxiety disorder, hoarse voice |
conflict in her family |
| 20 |
F |
75 |
1year |
jobless |
gradual |
anxiety disorder, hoarse voice |
conflict in her family |
| 21 |
F |
43 |
1and half year |
clerk |
gradual |
anxiety disorder, hoarse voice |
conflict in her family |
| 22 |
M |
33 |
4 months |
factory worker |
gradual |
aphonia |
financial affairs |
| 23 |
M |
46 |
3 months |
engineer |
sudden |
headache, hoarse voice |
conflict in his job |
| 24 |
F |
26 |
2years |
engineer |
gradual |
depression, hoarse voice |
conflict in her job |
| 25 |
M |
54 |
2 and half years |
singer |
gradual |
hoarse voice |
conflict in his job |
| 26 |
F |
36 |
5 months |
clerk |
sudden |
hoarse voice |
conflict in her job |
| 27 |
M |
46 |
10 years? |
announcer |
gradual |
anxiety disorder, hoarse voice |
conflict in his job |
| 28 |
F |
41 |
2 months |
house wife |
sudden |
hoarse voice |
conflict in her family |
| 29 |
F |
29 |
2 months |
clerk |
sudden |
hoarse voice after vocal cord operation |
conflict in her job |
| 30 |
M |
24 |
2 years |
student |
gradual |
hoarse voice after vocal cord operation |
after vocal cord operation |
| 31 |
F |
24 |
during visiting |
jobless |
gradual |
schizophrenia, hoarse voice |
avolition |
| 32 |
M |
21 |
during visiting |
student |
sudden |
schizophrenia, hoarse voice |
avolition |
| 33 |
F |
36 |
3 months |
consultant |
sudden |
depression, hoarse voice |
avolition |
| 34 |
F |
24 |
1year and 4months |
civil servant |
sudden |
aphonia |
after having cold |
| 35 |
F |
20 |
2 years and 6 months |
shop-girl |
sudden |
hoarse voice |
conflict in her job |
| 36 |
F |
21 |
2months |
student of vocal music |
gradual |
hoarse voice |
conflict in her training job |
| 37 |
F |
42 |
9 years |
clerk |
gradual |
hoarse voice |
conflict in her family |
| 38 |
M |
55 |
16 years |
announcer |
gradual |
hoarse voice |
conflict in his family |
Table 1: Number of subjects; 38 All patients; 1662 incidence rate 38/1662 (2.3%).
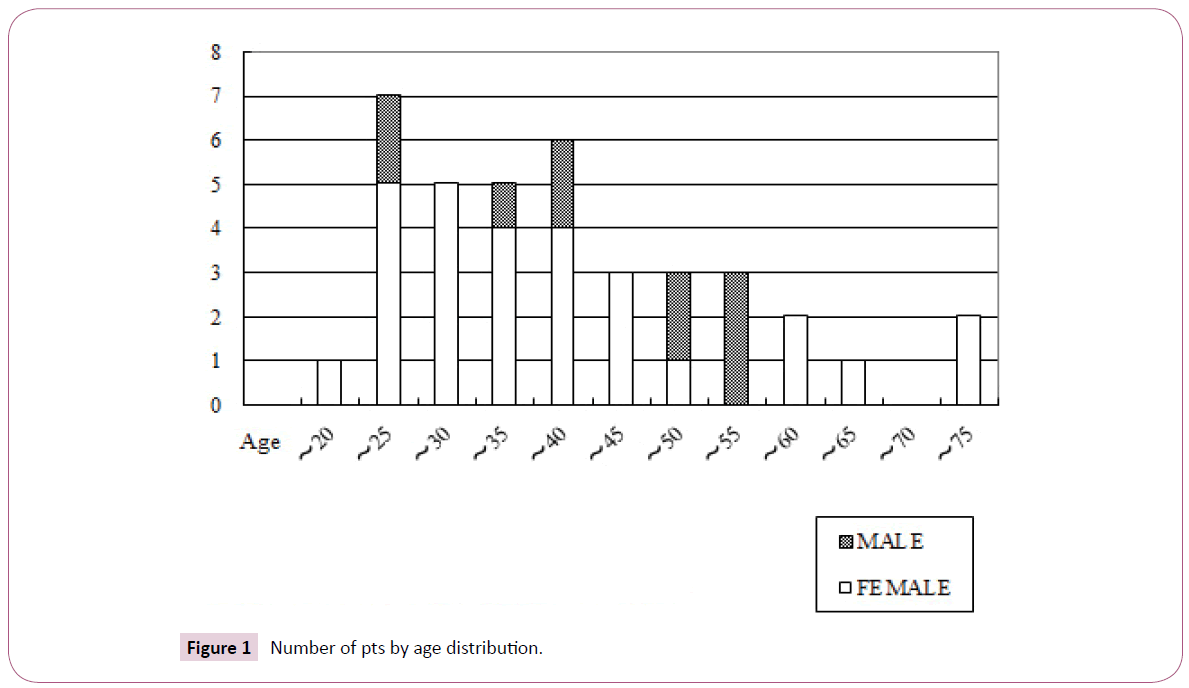
Figure 1: Number of pts by age distribution.
Patients were introduced to our clinic mainly (66% of the patients) by the otonasolaryngologist, psychiatrists, educational counsellors, gynecologists and others referred the rest. In addition, five (14%) patients who were being treated in our clinic with other disorders complained of dysphonia during the treatment (Figure 2).
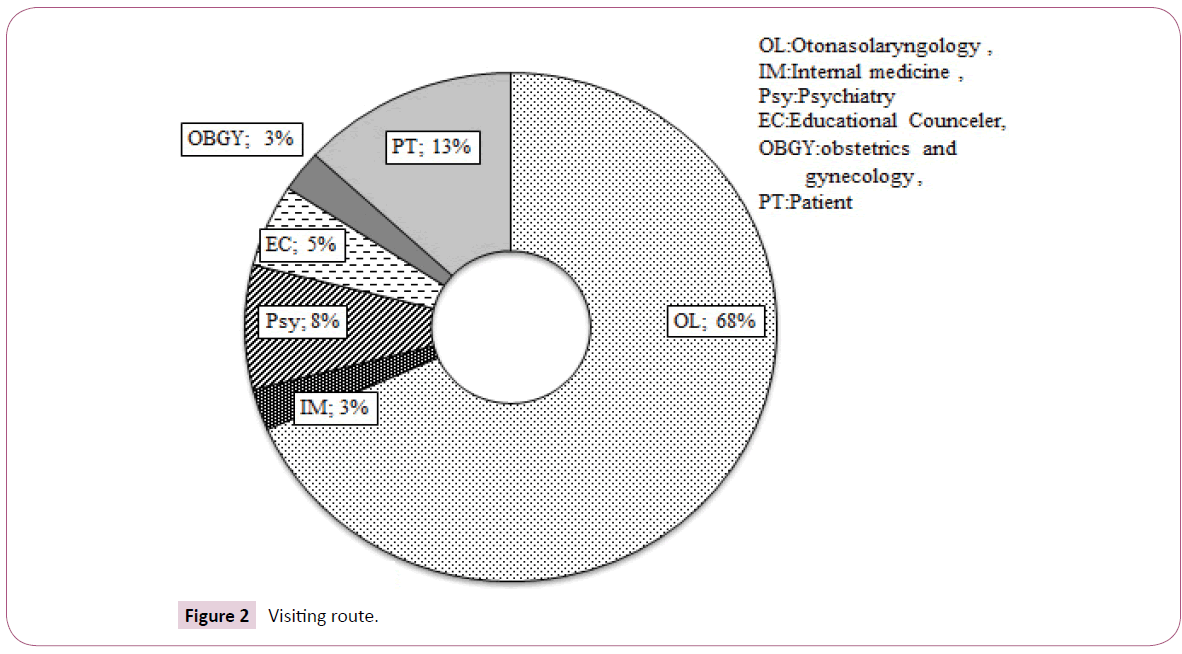
Figure 2: Visiting route.
The patients were interviewed by the author and some of them were treated by his staff. Notes were taken for each patient at all times, but no electric device was used to record her expression and attitude as most of our out-patients with other disorders.
In the clinic, all patients were diagnosed in accordance with ICD- 10. Accordingly, psychogenic dysphonia and aphonia are included in F44.4 dissociative motor disorders.
However, it was rather difficult to describe the complaints and voice sound of the patients. The character of voice sound was described and assessed according to the GRBAS* Scale [8] of the Society of Logopedics and Phoniatrics (Japan) (*unknown naming). The GRBAS scale is as follows: Total score=G;1,2,3, specifically; Rough=R;1,2.3, Breathy=B;1,2,3, Asthenic=A;1,2,3, and Strained=S;1,2,3. In very few patients (three cases) who uttered no voice sound, their appearances, expressions and behavior were described as PLS (pantomime-like silence). They can be called genuinely “aphonic”, which will be precisely described later. These data are shown in the Tables 2 and 3.
| No |
GRBAS |
Duration of treatment or from occurrence |
Times of interview |
Outcome* |
Drugs prescribed |
|
| 1 |
G-1, S-2 |
7ys and 7ms |
over 29 |
I |
BMZ, EZL, CNZ |
|
| 2 |
G-3, A, 3 |
4ys and 4ms |
over 19 |
R |
LRZ, APZ, ESZ, CNZ, ? |
|
| 3 |
G-3, B-2 |
7ys and 8ms |
over 65 |
R |
CNZ, CBZ, FDZ, PSR |
|
| 4 |
G-3, B-2 |
26ys |
over 85 |
R |
LFZ, BMZ, EZL |
|
| 5 |
G-3, S-3 |
3ys and 3ms |
over 33 |
E, R |
CXZ |
|
| 6 |
G-3, A-3 |
- |
1 |
E, R |
- |
Abbreviation |
Drug |
| 7 |
G-3, A-3 |
5ms |
A, 7 |
E, R |
APZ |
? Anti-anxiety drug |
| 8 |
G-3, A-3 |
1 and half ms |
A, 1 |
E, R |
PXT, BTZ, LRZ |
APZ, |
Alprazolam |
| 9 |
G-2, A, 3 |
about 3ys |
82 |
R |
CNZ |
BMZ |
Bromazepam |
| 10 |
G-2, A-3 |
1m |
2 |
R |
- |
CTZ |
Clotiazepam |
| 11 |
G-2, A-3 |
2ms |
over 2 |
R |
OXZ, FVA |
CXZ |
Cloxazolam |
| 12 |
G-1, R-1 |
obscure |
A, 3 |
E, R |
CNZ, BTZ, FVA |
DAP |
Diazepam |
| 13 |
PLS |
1y and 4ms |
26 |
I |
ARP |
EZL |
Etizolam |
| 14 |
G-1, S-1 |
obscure |
A, 4 |
E, R |
FVA |
FDZ |
Fludiazepam |
| 15 |
G-1, A-1 |
obscure |
A, 4 |
E, R |
ARP |
LFZ |
Ethyl lofrazepate |
| 16 |
G-1, B-1 |
1m |
3 |
I |
- |
LRZ |
Lorazepam |
| 17 |
G-1, R-1 |
2 and half ys |
A, 53 |
E, R |
LRZ, BMZ |
OXZ |
Oxazolam |
| 18 |
G-1, R-1 |
1m |
4 |
E, R |
LRZ |
CNZ |
Clonazepam* |
| 19 |
G-1, A-1 |
2 and half ys |
28 |
R |
BMZ, EZL, |
? Anti-depressant |
| 20 |
G-2, B-2 |
3 ys and 1m |
35 |
R |
DAP |
FVA |
Fluvoxamine |
| 21 |
G-2, S-2 |
1y and 11 ms |
10 |
R |
LPZ, FVA, VAP |
PXT |
Paroxetine |
| 22 |
PLS |
8ms |
14 |
I |
BMZ |
SRT |
Sertraline |
| 23 |
G-2, B-2 |
11 ms |
13 |
R |
LRZ, ARP, ZPD, EZL |
ETP |
Escitalopram |
| 24 |
G-2, R-2 |
3 ys and 2 ms |
40 |
R |
LRZ |
? Anti-psychotics |
| 25 |
G-1, S-1 |
4 ms |
8 |
I |
CNZ, EZL, DAP |
ARP |
Aripiprazole |
| 26 |
G-3, B-3 |
10ms |
20 |
E, R |
DAP.CNZ, APZ, |
BNS |
Blonanserin |
| 27 |
G-1, A-1 |
1m |
2 |
I |
DAP |
PSR |
Perospirone |
| 28 |
G-2, A-2 |
4 ms |
8 |
I |
CNZ, BMZ, BNS |
? Antiepileptics |
| 29 |
G-1, R-1 |
9 ms |
12 |
R |
LRZ, CTZ |
CNZ |
Clonazepam* |
| 30 |
G-1, R-1 |
2 ys |
1 |
I |
EZL |
CBZ, |
Clobazam |
| 31 |
G-1, A-1 |
2 s |
A, 7 |
E, R |
ARP |
VAP |
Sodium valproate |
| 32 |
G-1, S-1 |
2 ys and 4 ms |
A, 7 |
E, R |
BNS |
? Hypnotics |
| 33 |
G-0 |
1 m |
2 |
I |
CTZ, ZPD |
BTZ, |
Brotizolam |
| 34 |
PLS |
1 y and 4 ms |
4 |
A |
- |
ESZ, |
Estazolam |
| 35 |
G-1, S-1 |
6 ms |
12 |
R |
ARP |
ZPD |
Zolpidem |
| 36 |
G-2, R-1 |
5 ms |
8 |
R |
CNZ, DAP, ETP |
* Duplicate |
| 37 |
G-2, S-2 |
3 ms |
A, 8 |
A |
CNZ |
|
| 38 |
G-2, S-2 |
16 ys |
A, 3 |
A |
DAP |
|
Note: *A: Attending; E: Episodic; R: Recovered; I: Interrupted.
Table 2: GRBAS grade, duration of treatment, times of interview, outcome, pharmacotherapy.
| |
G-0 |
G-1 |
G-2 |
G-3 |
Sum |
Total |
| R |
-1 |
|
5 |
1 |
0 |
6 |
7 |
| -2 |
|
0 |
1 |
0 |
1 |
| -3 |
|
0 |
0 |
0 |
0 |
| B |
-1 |
|
1 |
0 |
0 |
1 |
7 |
| -2 |
|
0 |
2 |
2 |
4 |
| -3 |
|
0 |
0 |
2 |
2 |
| A |
-1 |
|
4 |
0 |
0 |
4 |
11 |
| -2 |
|
0 |
1 |
0 |
1 |
| -3 |
|
0 |
3 |
3 |
6 |
| S |
-1 |
|
4 |
0 |
0 |
4 |
9 |
| -2 |
|
1 |
3 |
0 |
4 |
| -3 |
|
0 |
0 |
1 |
1 |
| G-Sum |
|
1 |
15 |
11 |
8 |
34 |
35 |
| PLS |
|
|
|
|
3 |
38 |
Table 3: Assessment data by GRBAS scale.
Our psychologist, Ms. Umezu [9] performed Rorschach tests on some patients and reported the results at the International Congress of Rorschach and Projection Test in Tokyo in 2011.
Results
Course of onset of dysphonia or aphonia
Fifteen patients of the 38 patients developed difficulties in speaking (dysphonia) or lost their voices (aphonia) suddenly (sudden course), whereas 23 of them gradually exhibited dysphonia or aphonia (gradual course). Twelve cases exhibited either sudden or gradual onset intermittently or relapsed several times (episodic course). These results are duplicated in Table 4.
| |
Course |
| Sudden |
Gradual |
Episodic(E) |
After an air way disorder |
| Manifestation or symptom |
No |
No |
No |
No |
|
| Aphonia only |
3 |
2 |
1 |
2 |
2 |
| Dysphoni only |
15 |
5 |
10 |
|
4 |
| Complication of neurological symptoms* |
8 |
3 |
5 |
4 |
|
| Anxiety disorder |
6 |
0 |
6 |
2 |
1 |
| Depression |
4 |
3 |
1 |
2 |
|
| Schizophrenia |
2 |
2 |
0 |
2 |
|
| Total |
38 |
15 |
23 |
12 |
7 |
Note: *Paralysis of upper limbs, multiple personality, head ach, spina bifida.
Table 4: Course of occurrence of dysphonic manifestation and complication.
Eighteen cases had exhibited dysphonia or aphonia with no other physical, neurological or mental symptoms according to the introductory letters by other doctors. However, seven cases complained they had caught a cold or suffered a sore throat a couple of month before. On the other hand, eight cases had some neurological symptoms, and 12 cases suffered evident anxiety disorder, depressive state or schizophrenia.
Cases 13, who developed a sudden loss of voice was working as a volunteer activity in a country in South America. The day before one of the managers was supposed to visit her and inspect her work, she lost her voice completely. The symptoms had continued thereafter even after she came back to Japan. Case 10 worked hard every day with no overtime pay. One day at lunch time she lost her voice suddenly when her boss addressed her as usual.
Case 5, who developed a gradual occurrence of dysphonia or aphonia was reshuffled from a skilled office work position to an usherette because of dyskinesia in her hands. It was not until two months after that she gradually found difficulty in speaking, which eventually became serious.
Case 18, who developed an episodic course, had been very busy engaging in her office job and managing the business of her residential apartment. One morning she could not speak right when she was about to fly abroad as she does regularly for business. During her stay in Europe she developed difficulties with speaking. She had shown similar symptoms as this three years earlier.
The period between the onset of symptoms and visiting our clinic
As mentioned above, the patients were referred to us via various routes. Thus, it was rather difficult to understand the period between the onset of symptoms and the first visit to the clinic. Some patients visited the clinic within one month after the onset of a symptom, but some took longer, for a period of up to 12 years (Table 1).
The trigger or for the onset of the symptoms
The situations for all cases are as follows and are presented in Table 1. They are roughly classified into six or seven categories shown in the Figure 3.
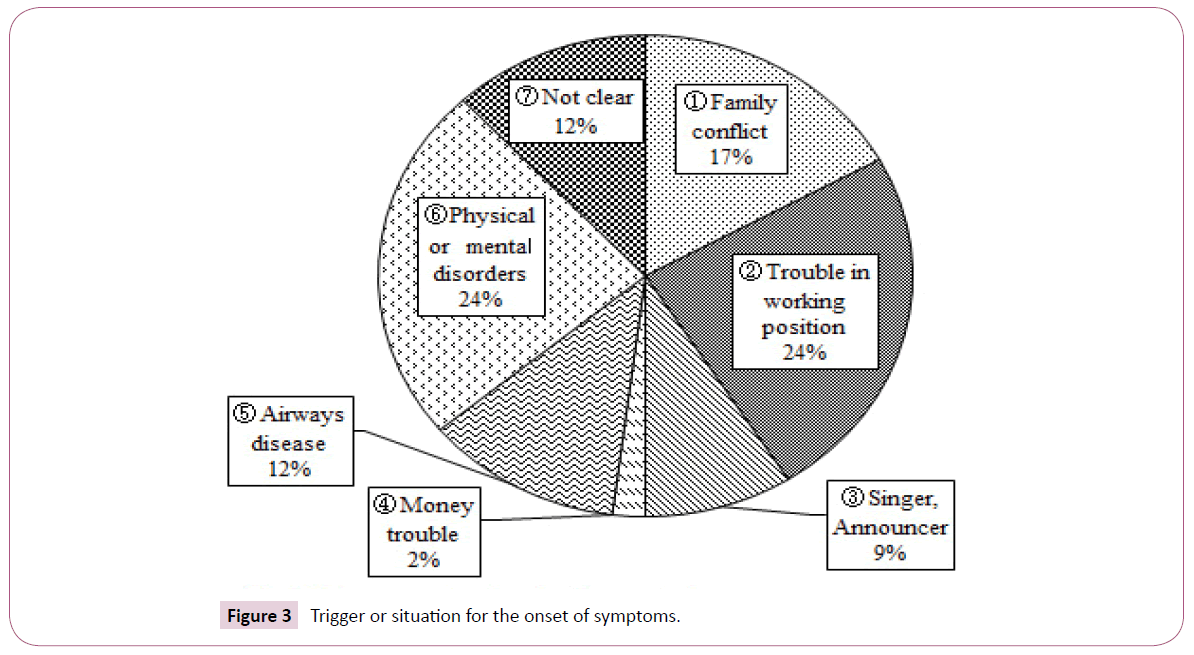
Figure 3: Trigger or situation for the onset of symptoms.
(1) [Conflicts in a family: Cases 2, 4, 11, 19, 20, 21, 28 and 37] When a patient is involved with a conflict in the family, either insidiously or directly, she has dysphonia (in this category, all cases are female). In this category, an emotional conflict occurs between a patient and her mother or mother-in-law or vice versa. Case 4 shared the same residence with her son’s family, but they lived in separate households. She developed dysphonia after a grand-daughter was born. In addition, her son was transferred to a distant office at the same time. Then the daughter- in-law started to express hatred towards her.
(2) [Trouble in the working place: Cases 5, 9, 10 and 18] Patients developed dysphonia when they performed a role or had a relationship with their boss or colleagues in the work place. Case 9 was abused by her colleagues because of her physical handicap (spina bifida). She was excellent in performing design drawing. She bore the abuse, and finally she could not speak smoothly.
(3) [Professional singer or announcer: Cases 2, 3, 17, 25, 27, 36 and 38] Patients started to have difficulties speaking smoothly or singing beautifully or announcing clearly. When Case 2 started to become successful, her husband began to complain about their household. In addition. In addition, her vocal instructor sexually harassed her. Gradually she lost her beautiful voice. Case 27 was getting a mid-level position as an announcer at a broad- casting station. Gradually the leader and senior announcer gave a harder task in announcing. Then the patient developed difficulties in vocalization.
(4) [Financial affairs] Case 22 started to be unable to speak after he owed a large debt. He lost his voice completely after it was found out that he had to pay a large debt from losing a bet.
(5) [After patients caught a cold or infection in the air-ways, no organic sign in the vocal cords, and no any other distinct abnormalities were found]
(6) [Some patients had some physical or mental disorders but neither organic abnormal signs in the vocal cords nor any other distinct abnormalities were found.] Fourteen cases belong to categories (5) and (6)
(7) [Unknown trigger or situation] There were five cases.
Telephone communication
Making telephone calls often made a patient dysphonic or accelerated their symptoms. After that most patients would not answer a phone or talk to any person.
Even after recovering from abrupt onset dysphonia of four months duration, the dysphonic symptoms of Case 26 worsened when she had to talk on the phone. Finally, she stopped answering calls completely.
The patients’ whole manifestation, complication, dysphonia/aphonia
All patients complained of difficulty with speaking. However, they strained to whisper and utter harsh or rough sounds. Sometimes they showed a very asthenic countenance and were very weak of voice. Of the 38 patients, 15 cases complained of only dysphonia. However, they also showed slightly depressed feeling. By contrast three other cases, mentioned above, showed complete silence. They looked bright and active and had energy. These three cases communicated by writing very fast and skillfully. Their syndrome should be called true aphonia (Tables 2-4).
20 cases of the 38 patients had various neuro-psychiatric complications, such motor paralysis (2 cases), multiple personality (1 case), congenital spina bifida with excellent intelligence (1 case), persistent headache (four cases), moderate depression (four cases), anxiety disorders (six cases) or schizophrenia (two cases). Details of these 20 cases with some complications will be described later.
At the first interview most patients used a pen to express their feelings and explain their situations. The therapist asked them to stop using a pen, and most patients except three cases complied.
Assessment data described by GRBAS Scale and PLS
All data from each patient are shown in Table 2, where the outcomes of the cases and the drugs prescribed are also described. The summarized results and relation to outcomes are shown in Tables 3, 5 and Figure 4. Inspecting the results assessed by the GRBAS scale, the number of G-1 grade cases are the most, at 15. G-2 grade cases are 11 and G-3 grade cases are 8. The cases judged as PLS are 3 as mentioned above. The relationship of the outcome and the grade of the GRBAS scale is not statistically significant and will be described later (Figure 4).
| GRVAS Scale |
G-0 |
G-1 |
G-2 |
G-3 |
PLS |
Number |
| Outcome |
|
|
|
|
|
|
| Recovered |
0 |
10 |
8 |
7 |
0 |
25 |
| Attending |
0 |
1 |
1 |
0 |
1 |
3 |
| Intercepted |
1 |
5 |
1 |
1 |
2 |
10 |
| Total |
1 |
16 |
10 |
8 |
3 |
38 |
Table 5: Outcome and GRBAS scale.
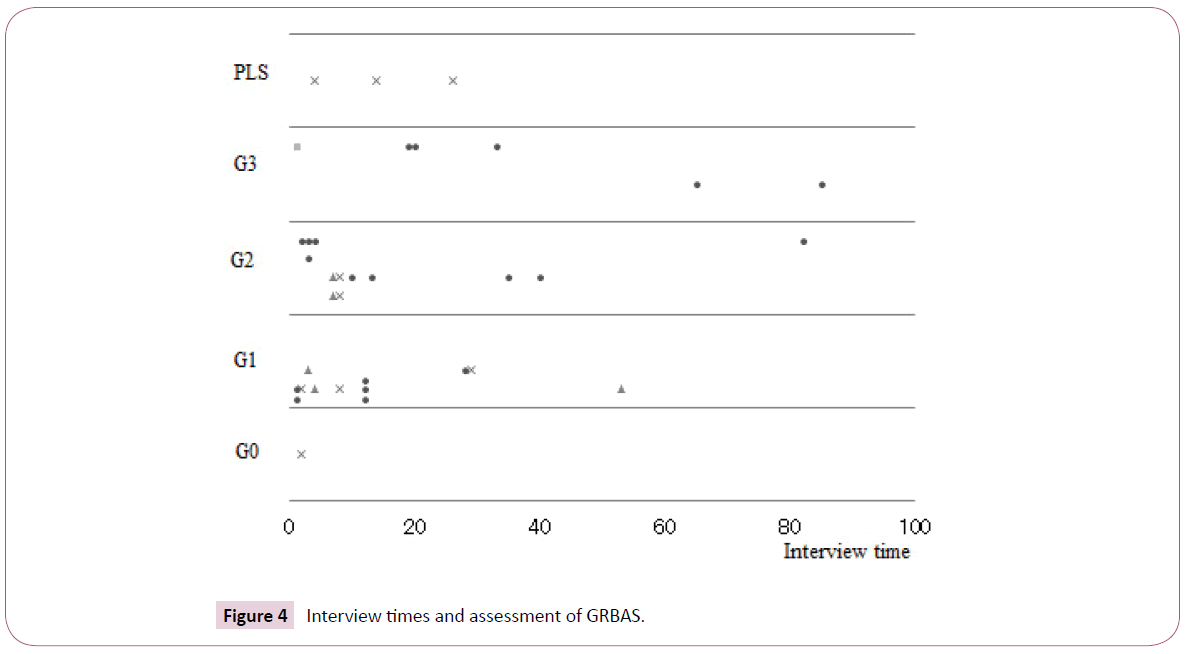
Figure 4: Interview times and assessment of GRBAS.
Character and daily life of the patients
It is rather difficult to describe the character generally. Most patients are honest, modest, hard-working but slightly awkward.
The report on six female patients’ characters investigated using Rorschach and Sentence Completion Test was presented by Umezu [9]. It says in the summary that “W-responses, to take the blot as it is, sometimes means to behave according to a superior’s expectation. To behave under rigid policies is the virtue in Japanese culture, especially for women. They knew the situation that pressured their lives, but they did not know how to interpret the abusive environment they were in, nor how to respond emotionally without getting into trouble. They felt anxiety, loneliness, aggression, and deep exhaustion. In the recovery process, some patients could use D-responses freely.
Emotional control still wasn’t enough but handling the situation within their own ability may be the key point for their recovery.”
Neuro-psychiatric complications with dysphonia
As described above, there were various complications which are explained here.
(1) Seemingly motor paralysis, two cases. Case 5 is described above, and Case 12.
(2) Case 15 with multiple personalities wanted to change her personality when she entered a college. She introduced herself under two names. Gradually she could not realize herself and sometimes lost consciousness. She was attacked by some bizarre symptoms and finally spoke with a hoarse voice.
(3) A case of congenital spina bifida, Case 9 is described above.
(4) Persistent headache, four cases. In all cases no organic sign was found.
(5) Anxiety disorders, six cases. Case 21 had suffered social phobia from 14 to 21 years-old. When she became 40 years old, she had a panic attack because of her family trouble. After she recovered, she started a job as a telephone appointer. Soon after that she had bitten her tongue. Since then she started to have difficulties in speaking.
(6) Moderate depression, four cases. Case 8 had been treated for almost 10 years because of depressive episodes at intervals. When she was 63 years-old, her mother died. The mother’s heritage was inherited to her brothers and sister, but nothing was given to her. After the funeral, she gradually developed aphonia.
(7) Schizophrenia, two cases. When Case 31 was 16 yearsold, she developed schizophrenia with abulia and auditory hallucinations. Since then she has been treated by our clinic. At the onset, dysphonia not mutism of several weeks-duration appeared but it disappeared completely after the remission.
Treatment
The psychotherapeutic treatment
At the first interview, most patients except few cases with bright countenance expressed slight anxiety and depression. At first the therapist himself did not use a pen and advised patients to try to speak as much as possible (Tables 2 and 5).
The therapist explained to them that the therapeutic plans consisted of a psycho-therapeutic approach, pharmacological means and some vocal training by a speech therapist. The first one included listening to them about their situation, accepting all of their distress, cognitive training to find the way to recovery and how to behave or vocalize. Each session was almost 30 min to 1 h.
Through the whole course of therapy, the therapist generally followed the instructions by H.S.
Sullivan [10], Peter Lomas [11] or other therapists. The basic principle of the author’s psychotherapy is written in his own book [12].
Case 6 and 16 recovered soon after two sessions during a month with no pharmacological treatment. Both of them started to utter voice smoothly when the treatment began and after they regained their fair voice, they agreed termination of therapy.
The psychopharmacological therapy
At first most patients expressed doubts as to whether they could regain their voices with pharmacological agents. The therapist explained to them precisely the efficacy of individual agents and obtained the informed consent from all patients except one. Case 34 rejected taking any agents, as she did with another doctor.
Considerably more agents were prescribed than what was expected when the treatment started (Tables 2 and 6). Most patients were given antianxiety agents, which had slight antidepressive efficacy as well.
| Outcome |
Anti-anxiety drug |
Anti-depressant |
Anti-psychotics |
Anti-epileptics |
| R |
32 |
6 |
5 |
10 |
| A |
1 |
0 |
1 |
0 |
| I |
12 |
0 |
2 |
0 |
| Sum |
45 |
6 |
8 |
10 |
Table 6: Prescribed agent and outcome (duplicated).
When the patients who were told they had a convulsive nature to their voice by a previous doctor and actually showed a strained voice, they were mainly given clonazepam which has both anti-anxiety and anti-convulsive efficacies. Particularly for Case 3 who is a popular singer, this agent had been very effective for a long time and finally could be discontinued.
Both patients who were originally diagnosed with depressive psychosis (Cases 8 and 14) and showed depressive states because of dysphonia (Cases 11, 12, 23 and 36) were administered anti-depressives, SSRIs of rather small doses.
Anti-psychotics had been originally administered to two patients (Cases 31 and 32).
Another six patients (Cases 3, 13, 15, 23, 28 and 35) who exhibited perplexed feelings or behaviour were also given very small doses of atypical anti-psychotics.
A few patients who complained of insomnia were prescribed hypnotics, such as benzodiazepines or other drugs.
The course of treatment and outcome
All patients including three complete aphonic patients returned with a relaxed mood to our clinic at least twice. The duration of visiting our clinic and number of sessions are shown on the Table 2 and Figure 4. The relation of the course or outcome of the treatment to the degree of GRBAS scale and PLS are also displayed in the Table 5 and Figure 4.
The patients who underwent remission did not necessarily show light degrees as G-1. However, the patients who were judged at first as G-2 or G-3 showed the tendency to need many sessions but eventually recovered. Thus, as observed above, the relation of the course or outcome of the treatment to the degree of GRBAS scale and PLS cannot be considered significant.
Twenty five patients recovered and are remission and three are still returning to the clinic at present. Final outcomes of 10 discontinued patients are unknown.
The relation of the efficacies of the pharmacological agents administered to the outcome, regretfully, could not be considered significantly different.
Two peculiar cases
Case 22 showed up in a complete aphonia and wrote neatly with a pen. At the second session, his mobile phone suddenly rang and he talked fluently to the other person, who was his mother. After the conversation terminated, he became mute again. Of course, the therapist advised him to solve his distress. However, he immediately he left and never returned to us.
Case 36 was an excellent student in a post graduate vocal music course. However, when she began to be instructed by her teacher, she started developing dysphonia. After eight sessions of psychotherapy and pharmacotherapy using anti-anxiety agents over a five-month period, she went to an amusement park with her younger sister. They rode a roller coaster. When the roller coaster plunged steeply, they shouted in a loud voice together. After the event she recovered her voice completely. After two years, she succeeded in singing at the memorial concert.
Discussion
Definition and significance of dysphonia and aphonia
As described above, dysphonia or aphonia are observed in various pathological states.
In the ICD 10 [1] aphonia is classified in the item dissociative motor disorder, F44.4. In DSM-4-TR [13], the mechanism of aphonia is described as “ for example, after an argument, inner conflict about the expression of rage may be expressed as “aphonia” or as a paralysis of the arm”, in the item 300.11:motor disorders of conversion disorder. However, no precise definition of aphonia exists. Surprisingly, there is, no definition of dysphonia or aphonia in the DSM-5 [14]. According to a Japanese otolaryngologist, H Hirose [15], aphonia means a state in which a patient speaks solely by whispering, but with no sound, because the glottis does not completely shut, even in the absence of any organic-pathological damage due to a psychogenic cause.
Some philological consideration on aphonia or dysphonia
In the description by Schuster et al. [16], the term “hysterical mutism” was introduced into the medical field under the direction of J.M. Charcot [17] in the late 19th century. The term aphonia was described in the 8th edition of a textbook by E. Kraepelin [18] but not in the 7th edition, where the term astasia and abasia were described. In Japan the first description on aphonia appeared in the textbook by S. Kure [19]. However, the term aphonia cannot be found in the literatures on hysteria by P. Janet [20], E. Kretschmer [21] and S. Freud [22]. When they observed the symptoms of hysteria, they noticed and described astasia or abasia but not aphonia as motor disturbances. The author wonders whether there were no aphasia or if they did not notice or think the phenomenon of aphonia was significant. Regardless the term “aphonia” or “dysphonia” appeared at the end of 19th century, and this fact is an important implicating regarding at the sociological change of human relation in this age, which will be discussed later.
When T. Yamazaki [23] reported 57 cases in Japanese in 1959, only a few but brief clinical reports on aphonia had been published in Japan. However, in his studies Yamazaki described 41 cases with muscular paralysis of the vocal cord inspected by himself. In Yamasita’s report [24], the EMG activities from the inner anterior and lateral vocal muscles increased but after-discharges decreased in dysphonia patients.
Causes or reasons of occurrence of dysphonia or aphonia suggested by the triggering events or situations
The events or situations that may trigger or cause the occurrence of dysphonia /aphonia are summarized from all cases and illustrated in six or seven items in Figure 3.
Among them it is characteristic that in the item of family conflicts the patients concerned were all females who were weaker in position and were forced either insidiously or directly to be involved in a conflict that may jeopardized her being in a family.
The item of troubles in the work place including professional singing or announcing, the patients suffered dysphonia when they were performing their work or having a difficult relationship with their bosses or colleagues. Each patient was necessarily weak in her position or physical condition and abused by her colleague or boss. Particularly when a singer or announcer started to become successful, a person around her spoke to her critically, or sexually harassed her. Patients began to feel difficulties in speaking smoothly, singing beautifully or announcing clearly.
Family conflict, work place trouble and professional singing or announcing hazard, are stressors threatening a patient’s well-being-in her social life. Aronson et al. [2] concluded acute situational conflicts were causative factors in the majority of 27 cases by MMPI assessment.
In our report, there was only one case of financial trouble. A patient started to be entirely unable to speak after he found out he owed a large debt. Generally, it is well known that several cases of conversion disorders are caused by economic trouble.
Some patients had some physical ailment, including a cold or infection of the air-ways or mental disorders but organic abnormal signs were found in neither the vocal cords nor in any other organ. Rather many cases belong to categories (5) and (6).
In the unknown triggers category, 12% of cases are included. More cases with sexual and economical trouble might be included, which are frequently observed in dissociation disorders.
Selection and propriety of treatments
As mentioned above, the author treated most patients with both psychotherapy and various pharmaceutical methods. At the same time some patients received vocal exercises independently. Generally speaking, a combination of these treatments and if possible, close communication between a medical doctor, psychotherapist and vocal trainer is recommended.
Additionally, after a careful assessment of antianxiety agents, which have slight anti-anxiety and depressive efficacy, treatment with these agents is recommended. If a patient shows a convulsive nature in the throat or strained voice, it is better to administer clonazepam which has both anti-anxiety and anti-convulsive efficacies.
First or secondary depressive patients should be administered anti-depressives, SSRIs of rather low doses. A psychotic patient should be given original anti-psychotics of the atypical generation, and if necessary, a small amount of clonazepam.
What aphonia and/or dysphonia means
Speaking is an indispensable means of expressing one-self in daily social life. Compared with astasia or abasia, dysphonia implies a greater loss of an important means in social life.
In most cases, family conflicts or troubles in the work place, including professional singing or announcing threaten one’s being in such a position. Under such threatening situation she cannot express herself, which means a disadvantage or peril in her social life. From this point of view, it is easier to understand that the number of female patients is greater than the number of male patients. One can say females in their late twenties to thirties and males in forties to fifties are at a risky age in their social lives.
As mentioned above the symptoms or terms “aphonia” or “dysphonia” were not be noticed or described until the last decade of the 19th century, although many symptoms of hysteria or conversion disorder had been observed and reported by Charcot [16,17]. According to Baggioni [25], from the end of the 19th century to the first two decades of the 20th century before World War 1, a new acquisition of freedom in human language occurred from mutual recognition of the traditional society in European society. Around the time, Saussure [26], the so-called founder of linguistics was giving his lecture on new linguistics and Freud introduced psychoanalysis in psychiatry. In parallel with the change of the current in human language, patients with hysteria or conversion disorder had been noticed to show dysphonia. The author defines “aphonia/dysphonia” as a state in which vocalization is only with a hoarse voice or incapable of speaking and expressing oneself by only gesture with no organic abnormalities of the vocal cords.
Funding
The source of funding was supported only by the Sannou Institute of Psychiatry and Psychology.
Acknowledgement
The author expresses profound gratitude to Professor Dr. Hiroyuki Fukuda who had led him to the extensive clinical work on dysphonia and introduced most patients to his clinic. Additionally, he extends sincere thanks to Atsuko Umezu, clinical psychologist, Yuko Nakahara, speech therapist and Chieko Furuya-Mine, psychiatric social worker, as well as Ms. Yukiko Niikawa, for her graphic design and all other staff for their eager collaboration.
References
- WHO (1994) ICD-10 F44.4, Dissociative motor disorder. Psychological Aphonia.
- Aaronson AE, Peterson HW Jr, Litin EM (1966) Psychiatric symptomatology in functional dysphonia and aphonia. J Speech Hear Disord 31: 115-127.
- House A, Andrews HB (1987) The psychiatric and social characteristics of patients with functional dysphonia. J Psychosom Res 31: 483-490.
- Andersson K, Schalen L (1997) Etiology and treatment of psychogenic voice disorder: results of a follow-up study of thirty patients. J Voice 98: 80081-80087.
- Maniecka-Aleksandrowwicz B, Domeracka-Kolodziei A, Rozak-Komorowska A, Szeptvcka-Adamus A (2006) Management and therapy in functional aphonia: analysis 500 cases. Otolaryngol Pol 60: 191-197.
- Reiter R, Pommel D, Brosch S (2013) Long term outcome of psychogenic voice disorders. Auris Nasus Larynx 40: 470-475.
- Martins RH, Tavares EL, Ranalli PF, Branco A, Pessin AB (2014) Psychogenic dysphonia: diversity of clinical and vocal manifestations in a case series. Braz J Otorhinolaryngol 80: 497-502.
- https://www.interm.co.jp
- Umezu A (2011) Rohrschach and sentence completion test. International Congress of Rohrschach and Projective Methods, Tokyo.
- Sullivan HS (1954) The Psychiatric Interview. The William Alanson White Foundation, WW Norton & Company Inc., New York.
- Lomas P (1973) True and false experience. London: Allan Lane, p: 160.
- Suzuki J (2001) Interview as a Therapy (Jap). Kongou Publishing C., Tokyo.
- American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders (4th Edn).
- American Psychiatric Association (2012) Diagnostic and statistical manual of mental disorders (5th Edn).
- Hirose H (1998) Clinic on vocal disorders (Jap). Interuna Shuppann, Tokyo.
- Schuster JP, Mouchabac S, Le Strat Y, Limosin F (2011) Hysterical Mutism. Encephale 37: 339-344.
- L’Iconographie photographique de la Salpetriere, service de J-M. Charcot, par Bourneville et P. Regnard. Paris, Progres Medical, V. Adrien Delahaye & Cie, 1877.
- Kraepelin E (1915) die hysterische Aphonie. Psychiatrie (8th Edn). Verlag von Johann Ambrosius Barth, p: 1592.
- Kure S (1917) Aphonie. Textbook of mental disease (1st Part). Tohoudou Shoten, Tokyo, p: 253.
- Janet P (1911) L’etat mental Hysteriques (2nd Edn). Felix Algan, Editeur, Paris.
- Kretschmer E (1948) Medizinische Psychologie. Georg Thieme Verlag, Stuttgart.
- Freud S (1952) Studien ueber Hysterie. Gesammelte Werke Bd.1, Imago Publishing Co. Ltd, London.
- Yamazaki T, Ishikawa M, Kamimura T (1959) Nature of hysteric aphonia. JIBI to Rinshou 6: 52-57.
- Yamasita T, Ueda N, Kawamoto N, Ueda S (2009) Hysteric dysphonia and EMG of inner laryngeal muscle. JIBI to Rinshou 6: 370-375.
- Baggioni D (1997) Langues et nations en Europe. Editions Payot & Rivages.
- Constantin M (1910) 3 eme Cours de Linguistique Generale by Ferdinand de Saussure, the Bibliotheque Publique et Universitaire, Geneva.

