Manu K Nayar, Keith L Leiper, Martin G Lombard
Department of Gastroenterology, Royal Liverpool University Hospital. Liverpool, United Kingdom
- *Corresponding Author:
- Manu Nayar
17, Druids cross road
Calderstones
Liverpool L18 3EA
United Kingdom
Phone: +44-7841.575.792
Fax: +44-151.7065.846
E mail: nayarmanu@hotmail.com
Received January 9th, 2005 - Accepted January 25th, 2005
Keywords
Esophageal Stenosis; Esophagitis; Pancreas; Pancreatic Cyst
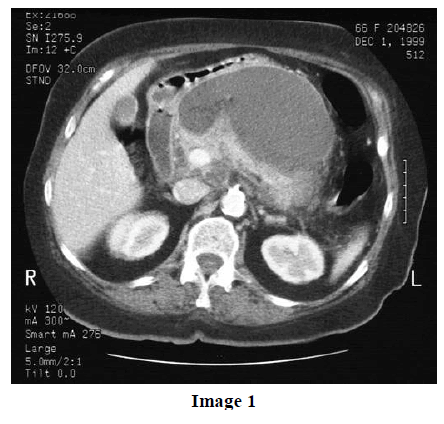
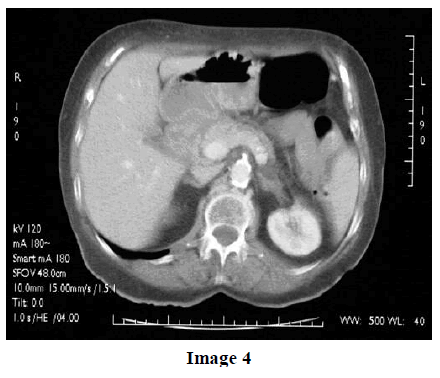
A-68-year old lady was admitted in with a history of feeling generally unwell and tired. Routine investigations were inconclusive. She recovered well in hospital and the conclusion was that she probably had an episode of viral fever. She was readmitted two months later with a history of epigastric pain, heartburn and loss of appetite. Routine blood tests including full blood count, urea and electrolytes, liver function tests and Creactive proteins were normal. Gastroscopy showed mild esophagitis, severe erosive gastritis with a slight bulge in the antrum. She was started on high dose proton pump inhibitors and sucralfate for gastric protection. In view of the bulge in the antrum we performed a computed tomography scan which revealed a 5x5x2 cm pancreatic pseudocyst impinging on the stomach wall, a portal vein and pancreas otherwise looked normal (Images 1 and 2). Subsequently she had an extensive anterior wall myocardial infarction and had a stormy course in hospital with left ventricular failure and chest infections. She recovered very well and was discharged with the plan of draining the pseudocyst at a later date. Unfortunately she was readmitted with symptoms of dysphagia and loss of appetite and gastroscopy this time revealed a tight esophageal stricture probably secondary to prolonged reflux of acid and inflammation. The stricture was dilated with relief of symptoms. Multiple repeat esophageal biopsies over the next three months revealed chronic inflammation and no evidence of neoplasia. Repeat CT scan done after six months demonstrated the pseudocyst but she had by now developed splenic vein thrombosis. It was felt the cause for the stricture was secondary to persistent reflux of acid because of the pseudocyst compressing the gastric lumen. Endoscopic ultrasound and CT scan performed six weeks later demonstrated that the cyst had reduced in size and no intervention was required (Images 3 and 4). She continues to have regular esophageal dilatation, every 3-4 weeks. She is on high dose proton pump inhibitors and continues to be in good health


Idiopathic acute pancreatitis is seen in 30% of patients presenting with symptoms of abdominal pain and nausea [1]. Most patients (36%) subsequently do not have further attacks. Pancreatic pseudocyst may be a consequence of acute pancreatitis, pancreatic trauma or chronic pancreatitis. Symptomatic pseudocysts may require treatment either surgical, radiological or endoscopic drainage. Complications of pseudocysts (i.e., hemorrhage, infection, rupture and malignant transformation) occurs in 5 to 41% and roughly correlates with the size of the cysts [2]. Though pressure effects of the cysts on surrounding structures (i.e., stomach, duodenum, biliary tree) is a recognized entity [3], there is no data in literature suggesting a pseudocyst resulting in persistent gastroesophageal reflux due to pressure effects on the gastric wall. We postulate that constant reflux has resulted in repeated episodes of acute inflammation leading to stricture formation. In this case, prolonged stasis was probably exacerbated by her morbidity following a myocardial infarction. Repeated biopsies are necessary to rule out the possibility of underlying malignancy. Although an uncommon consequence of a pancreatic pseudocyst one should to be alerted to the possibility of this complication occurring especially in a patient complaining of persistent reflux symptoms. The pseudocyst may require drainage (unlike in our case) to prevent stricture formation. Treatment includes acid suppression in high doses. Prokinetic agents may be necessary.
References
- Di Magno EP, Chari S. Acute pancreatitis. In: Sleisinger MH, Fordtran JS, eds. Gastrointestinal Disease. Volume 2. 7th ed. Philadelphia, PA, USA: Saunders, 2002:913-37.
- Yeo CJ, Bastidas JA, Lynch-Nyhan A, Fishman EK, Zinner MJ, Cameron JL. The natural history of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990; 170:411-7. [PMID 2326721]
- O'Malley VP, Cannon JP, Postier RG. Pancreatic pseudocysts: cause, therapy, and results. Am J Surg 1985; 150:680-2. [PMID 3907380]

