Keywords
Pancreatic Neoplasms; Prophylactic Surgical Procedures
Abbreviations
BO biliary obstruction; GOO gastric outlet obstruction;
PBGB prophylactic biliary and gastrointestinal bypass; PHC pancreatic
head cancer, QOL quality of life
INTRODUCTION
Pancreatic cancer is the most aggressive malignancy
of the abdominal organs, and approximately 80% of
pancreatic cancers are found in unresectable state [1].
The pancreas head is the most common site at which
pancreatic cancer develops [2]. Pancreatic head cancer
(PHC) is often associated with biliary obstruction (BO),
which causes jaundice, liver dysfunction, and cholangitis,
and gastric outlet obstruction (GOO), which develops in a
relatively later period and leads to anorexia and vomiting.
These complications deteriorate the quality of life (QOL)
of patients with PHC. Although the best way to prevent or
palliate BO and GOO is curative resection, most patients
with PHC do not benefit from resection. The National
Comprehensive Cancer Network guidelines propose
endoscopic biliary stenting, percutaneous biliary drainage
with subsequent internalization, and open biliary bypass
to palliate BO and gastrojejunostomy, enteral stenting, and
percutaneous endoscopic gastrostomy to palliate GOO in
patients with unresectable PHC [3].
However, some patients with unresectable PHC have
no symptoms of BO or GOO at the time of diagnosis. These
patients are usually treated by chemotherapy without
palliation. However, most patients are expected to develop
BO or GOO as the lesions progress. These complications
often interrupt continuation of chemotherapy. Cholangitis
due to BO can be life-threatening, especially when
patients have leukocytopenia secondary to chemotherapy.
Therefore, it is reasonable to prevent the development
of BO prior to chemotherapy. In addition, the usefulness
of prophylactic gastrointestinal bypass for unresectable
periampullary cancer has been shown in randomized
controlled trials [4, 5].
We have performed biliary and gastrointestinal bypass
in unresectable PHC patients without either BO or GOO
who were fit for surgery and provided informed consent
to prevent the development of BO and GOO and thus
ensure planned chemotherapy as well as maintain the patients’ QOL. The purpose of this study was to evaluate
the safety and preventive effect of prophylactic biliary and
gastrointestinal bypass (PBGB) for patients without either
BO or GOO. For this purpose, we analyzed perioperative
outcomes of PBGB and compared long-term outcomes
including the incidence of BO and GOO between patients
with and without PBGB.
METHODS
Study Population
This study was approved by the Ethics Committee of
Kyushu University and conducted according to the Helsinki
Declaration. We retrospectively reviewed the medical
records of patients who had PHC that was considered
unresectable owing to locally advanced or metastatic
disease and who were treated at the Department of
Surgery and Oncology, Kyushu University Hospital
between January 2001 and December 2013. Patients
without either BO or GOO at the time of their first visit
were selected for the study. They were divided into a
PBGB group and a control group according to whether
they underwent PBGB. The perioperative outcomes
of PBGB were analyzed. If patients had undergone
palliative treatment for BO or GOO, the outcomes were
also reviewed. The patients’ clinical backgrounds and
long-term outcomes, including the incidence of BO and
GOO and the survival rate, were compared between the
two groups. Survival time was defined as the period
between the first visit to our institute and death. For
patients diagnosed with unresectable PHC by imaging
findings, the treatment was selected at the discretion
of the attending surgeons or physicians and the
patients’ intentions. We generally recommended PBGB
if patients were fit for surgery. However, chemotherapy
or chemoradiotherapy was selected for patients
who were considered to need early administration
of chemotherapy, such as those with multiple liver
metastases; patients with locally advanced disease who
had possibility of conversion to resection; and patients
whose life expectancy was considered short. If the
PHC in patients who were planned to undergo curative
resection was found to be unresectable at laparotomy,
biliary and gastrointestinal bypasses were performed.
Biliary and Gastrointestinal Bypass
We mainly performed hepaticocholecystojejunostomy
for biliary bypass and gastrojejunostomy for gastrointestinal
bypass. These procedures have been previously described
[6]. Briefly, approximately 1-cm incisions were created at
the common hepatic duct and neck of the gallbladder, and
a single-layer side-to-side anastomosis of the common bile
duct and gallbladder was performed with an interrupted
or running suture. Side-to-side cholecystojejunostomy and
side-to-side gastrojejunostomy were carried out in a Rouxen-
Y fashion. Side-to-side jejunojejunostomy between the
afferent and efferent loops was then performed (Braun
anastomosis). Both stapling devices and hand suturing
were used for these anastomoses.
Statistical Analysis
Continuous variables were compared by Student’s
t-test or the Mann–Whitney U-test. Categorical variables
were compared by the chi-square test or Fischer’s exact
test. The Kaplan–Meier method was used to estimate
survival, and the log-rank test was used for comparison.
A two-sided p value of <0.05 was considered statistically
significant. All statistical analyses were performed using
JMP software (version 9.0.2; SAS Institute, Cary, NC, USA).
RESULTS
In total, 151 patients with unresectable PHC were
treated in our institution between January 2001 and
December 2013. The reasons for unresectability were
locally advanced disease in 77 patients (51%), metastatic
disease in 33 (22%), and both locally advanced and
metastatic disease in 41 (27%). The associations of BO or
GOO with the patients’ palliative treatments are shown in Figure 1.
Figure 1. Association of biliary obstruction (BO) or gastric outlet obstruction (GOO) and palliative treatments in 151 patients with unresectable pancreatic head cancer (PHC). †Two patients underwent endoscopic biliary stenting and other 2 patients had percutaneous biliary drainage prior to bypass.
Ninety-three patients had either BO or GOO, and 60
of them initially underwent biliary and gastrointestinal
bypass. Although 33 of the 93 patients were initially
treated by biliary stenting, six of them required biliary and
gastrointestinal bypass later.
Fifty-eight patients had neither BO nor GOO at
the time of diagnosis. Thirty-two of these 58 patients
underwent PBGB (PBGB group). The PHC of three
patients in the PBGB group was found to be unresectable
at laparotomy, and the PHC of the remaining patients
was considered unresectable based on imaging findings.
Hepaticocholecystojejunostomy, hepaticojejunostomy,
and cholecystojejunostomy were performed for biliary
bypass in 29, 2, and 1 patient, respectively. All patients
underwent gastrojejunostomy. The median operation time,
median blood loss, and median postoperative hospital stay
were 272 minutes (range, 129–495 min), 173 ml (range,
30–610 ml), and 18 days (range, 4–59 days), respectively.
Only one patient (3%) had postoperative morbidity (bile
leakage); no perioperative mortality occurred. The patient
with bile leakage was treated conservatively. During
the postoperative follow-up, neither BO nor GOO was
recognized in the PBGB group.
The remaining 26 patients were designated as the
control group. All patients in the control group developed
BO or GOO and required intervention during the follow-up:
14 patients were treated by endoscopic biliary stenting,
and the other 12 underwent biliary and gastrointestinal
bypass. Among the 12 patients who underwent bypass, 1
developed BO, 5 developed GOO, and 6 developed both BO
and GOO before bypass. Of the six patients who developed
BO and GOO before bypass, two underwent endoscopic
biliary stenting and two underwent percutaneous biliary
drainage prior to bypass. In the control group, 81%
(21/26) of the patients developed BO and 42% (11/26)
developed GOO. The incidences of BO and GOO in the
control group were significantly higher than those in the PBGB group (p<0.0001 and p<0.0001, respectively). Two
patients (8%) developed morbidities after intervention.
One patient developed a liver abscess after stent insertion,
and another patient developed a brain infarction after
bypass. Twelve of the 14 patients (86%) treated by biliary
stenting required stent replacement at a median frequency
of 2 (range, 1–10).
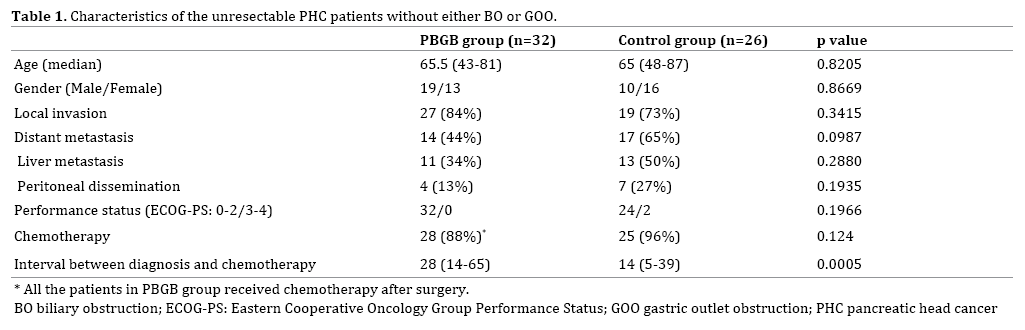
The patients’ characteristics including age, sex, local
invasion, distant metastasis (including liver metastasis
and peritoneal dissemination), performance status, and
introduction of chemotherapy were comparable between
the PBGB and control group (Table 1). Although interval
between initial diagnosis and first chemotherapy was
significantly longer in the PBGB group, the survival
time from the patients’ first visit at our institution was
comparable between 2 groups (356 days in the PBGB
group and 358 days in the control group; p=0.6368) (Figure 2).
Figure 2. Overall survival from the day of the first visit. Overall survival was not significantly different between the PBGB and the control group
(p = 0.6368).
DISCUSSION
In the present study, the following findings were
revealed: 1) PBGB effectively prevented development of
both BO and GOO in patients with unresectable PHC, while
all patients in the control group required subsequent
palliative procedure; 2) The postoperative morbidity and
perioperative mortality rates associated with PBGB were
quite low; and 3) There was no difference in survival
between the PBGB and control group.
Several studies, including randomized controlled trials
and meta-analyses, reported a lower recurrence rate of BO
in patients who underwent surgical biliary bypass than in
those who underwent biliary stenting [7, 8, 9, 10, 11, 12, 13]. In our study, none of the patients who underwent PBGB developed BO, while 81% (21/26) of the patients in
the control group developed BO. In addition, 86% (12/14)
of the patients who were treated by biliary stenting in the
control group had recurrence of BO and required stent
replacement. Although some authors asserted that the
main advantage of biliary stenting is a shorter hospital
stay [8, 11], a literature review by Glazer et al. [9] showed
that the total hospital stay from the procedure until
death was longer in patients with biliary stenting than in
patients with bypass because of repeated hospitalization
for stent replacement. Most of the biliary stents used for
the patients in this study were plastic stents because of the
policy of our institute. The patency period of a plastic stent
is shorter than that of a metal stent. A review by Moss et
al. [10] showed that the median patency of a metal stent
ranged from 108 to 273 days while that of a plastic stent
ranged from 54 to 165 days. However, this result suggests
that even metal stents require replacement if they are used
for patients whose life expectancy is nearly 1 year, as in
our series.
Two randomized controlled trials showed that
prophylactic gastrojejunostomy significantly reduced
the incidence of GOO in patients who were found to have
unresectable cancer after laparotomy [4, 5]. In the trial
in Netherland, 44% (12/29) of the patients with biliary
bypass alone developed GOO, while only 6% (2/36) of
the patients with biliary and gastrointestinal bypass
did [5]. In a study performed at Johns Hopkins [4], 19%
(8/43) of the patients with biliary bypass alone developed
GOO, although surgeons had judged that they were not
at a significant risk for duodenal obstruction at the time
of surgery. In the latter study, none of the patients with
biliary and gastrointestinal bypass developed GOO. In both trials, additional gastrointestinal bypass did not increase
morbidity or mortality.
In previous studies, the morbidity and mortality rates
associated with palliative biliary and gastrointestinal
bypass reportedly ranged from 17% to 50% and from
0% to 5.9%, respectively [4, 5, 14, 15, 16, 17]. Compared
with these results, the postoperative outcomes of our
study (morbidity: 3%, mortality: 0%) were quite
favorable. One possible reason for the low incidence
of postoperative morbidity and mortality was that
patients in the PBGB group did not have BO and GOO at
the time of the operation. Singh et al. [18] reported that
preoperative biliary stenting significantly increased
morbidity and mortality after surgical bypass. Räty et al. [19] described that gastric emptying problems owing to
GOO were a risk factor of postoperative morbidity after
hepaticojejunostomy and gastrojejunostomy. Patients
with GOO often have concurrent nutritional disorders.
Malnutrition increases postoperative morbidity and
mortality [20]. Additionally, PBGB can avoid the
emergency setting. Bartlett et al. [15] showed that
an emergent operation is a significant risk factor for
postoperative morbidity and mortality.
Our results did not show a significant difference in
the prognosis between the PBGB and the control groups.
Suspension of chemotherapy due to BO or GOO in the control group might have few effects on survival in our series.
Recently, combinations of chemotherapy regimens, such
as FOLFIRINOX or nab-paclitaxel plus gemcitabine, have
been shown to prolong survival of patients with pancreatic
cancer metastasis [21, 22]. No patient in our study
received these regimens because they were authorized in
Japan quite recently (FOLFIRINOX, December 2013; nabpaclitaxel
plus gemcitabine, December 2014). These new
regimens are more frequently associated with neutropenia
than the conventional regimen [21, 22]. Development or
recurrence of BO might have resulted in severe cholangitis
and prolonged suspension of chemotherapy in the control
group if patients had been treated by new regimens. In
addition, Conroy et al. [21] called for attention to BO in
FOLFIRINOX because high bilirubin levels increase the
risk of irinotecan-induced toxicity. Our results showed
that PBGB had a reliable and preventive effect on BO. The
PBGB group might have shown more favorable prognostic
outcomes than the control group if they had been treated
by these new regimens.
Recently laparoscopic approaches have been applied to
BO and GOO [23, 24, 25]. They might reduce postoperative
pain, enhance recovery of the patients and be options of
palliative treatment for unresectable pancreatic cancer
patients.
A limitation of our study was the retrospective,
nonrandomized design; thus, there might be selection bias
between the PBGB and the control group. The treatments
that patients received were diverse because our policy for
treating unresectable pancreatic cancer changed during
the study period. To establish solid evidence of PBGB,
prospective randomized control trials are needed.
CONCLUSION
PBGB showed excellent preventive effects on BO and
GOO with low morbidity. At the present time, nonsurgical,
palliative procedures are preferred for the treatment
of BO and GOO associated with unresectable PHC rather
than surgical prophylactic procedures. PBGB may have the
potential to improve the QOL and prognosis of patients
with unresectable PHC in the progress of chemotherapy. It
is time to reappraise prophylactic surgical procedures for
unresectable pancreatic cancer.
Acknowledgment
The protocol of this research has been approved by a
suitably constituted Ethics Committee of the institution and it
conforms to the provisions of the Helsinki Declaration. Ethics
Committee of Kyushu University, Approved No. 28-112.
This study was supported by Grants-in-Aid for Scientific
Research (KAKENHI; #16K10601).
Conflict of Interest
Authors declare no conflict of interests for this article.
References
- Li D, Xie K, Wolff R, Abbruzzese JL. Pancreatic cancer. Lancet 2004; 363:1049–57. [PMID: 15051286].
- Hruban RH, Boffetta P, Hirooka N, Iacobuzio-Donahue C, Kato Y, Kern SE, et al. Ductal adenocarcinoma of the pancreas. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. WHO classification of tumours of the digestive system. 4th ed. Lyon: IARC; 2010. p. 281–91.
- National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology: pancreatic adenocarcinoma. Version 2. 2015.
- Lillemoe KD, Cameron JL, Hardacre JM, Sohn TA, Sauter PK, Coleman J, et al. Is prophylactic gastrojejunostomy indicated for unresectableperiampullary cancer? A prospective randomized trial. Ann Surg 1999; 230:322–8; discussion 8–30. [PMID: 10493479].
- Van Heek NT, De Castro SM, van Eijck CH, van Geenen RC, Hesselink EJ, Breslau PJ, et al. The need for a prophylactic gastrojejunostomy for unresectableperiampullary cancer: a prospective randomized multicenter trial with special focus on assessment of quality of life. Ann Surg 2003; 238:894–902; discussion 902–5. [PMID: 14631226].
- Ueda J, Kayashima T, Mori Y, Ohtsuka T, Takahata S, Nakamura M, et al. Hepaticocholecystojejunostomy as effective palliative biliary bypass for unresectable pancreatic cancer. Hepatogastroenterology 2014; 61:197–202. [PMID: 24895820].
- Andersen JR, Sorensen SM, Kruse A, Rokkjaer M, Matzen P. Randomised trial of endoscopic endoprosthesis versus operative bypass in malignant obstructive jaundice. Gut 1989; 30:1132–5. [PMID: 2475392].
- Artifon EL, Sakai P, Cunha JE, Dupont A, Filho FM, Hondo FY, et al. Surgery or endoscopy for palliation of biliary obstruction due to metastatic pancreatic cancer. Am J Gastroenterol 2006; 101:2031–7. [PMID: 16968509].
- Glazer ES, Hornbrook MC, Krouse RS. A meta-analysis of randomized trials: immediate stent placement vs. surgical bypass in the palliative management of malignant biliary obstruction. J Pain Symptom Manage 2014; 47:307–14. [PMID: 23830531].
- Moss AC, Morris E, Mac Mathuna P. Palliative biliary stents for obstructing pancreatic carcinoma. Cochrane Database Syst Rev 2006:CD004200. [PMID: 16625598].
- Shepherd HA, Royle G, Ross AP, Diba A, Arthur M, Colin-Jones D. Endoscopic biliary endoprosthesis in the palliation of malignant obstruction of the distal common bile duct: a randomized trial. Br J Surg 1988; 75:1166–8. [PMID: 2466520].
- Smith AC, Dowsett JF, Russell RC, Hatfield AR, Cotton PB. Randomised trial of endoscopic stenting versus surgical bypass in malignant low bile duct obstruction. Lancet 1994; 344:1655–60. [PMID: 7996958].
- Taylor MC, McLeod RS, Langer B. Biliary stenting versus bypass surgery for the palliation of malignant distal bile duct obstruction: a meta-analysis. Liver Transpl 2000; 6:302–8. [PMID: 10827230].
- Ausania F, Vallance AE, Manas DM, Prentis JM, Snowden CP, White SA, et al. Double bypass for inoperable pancreatic malignancy at laparotomy: postoperative complications and long-term outcome. Ann R Coll Surg Engl 2012; 94:563–8. [PMID: 23131226].
- Bartlett EK, Wachtel H, Fraker DL, Vollmer CM, Drebin JA, Kelz RR, et al. Surgical palliation for pancreatic malignancy: practice patterns and predictors of morbidity and mortality. J Gastrointest Surg 2014; 18:1292–8. [PMID: 24671470].
- Lesurtel M, Dehni N, Tiret E, Parc R, Paye F. Palliative surgery for unresectable pancreatic and periampullary cancer: a reappraisal. J Gastrointest Surg 2006; 10:286–91. [PMID: 16455463].
- Mann CD, Thomasset SC, Johnson NA, Garcea G, Neal CP, Dennison AR, et al. Combined biliary and gastric bypass procedures as effective palliation for unresectable malignant disease. ANZ J Surg 2009; 79:471–5. [PMID: 19566872].
- Singh S, Sachdev AK, Chaudhary A, Agarwal AK. Palliative surgical bypass for unresectableperiampullary carcinoma. Hepatobiliary Pancreat Dis Int 2008; 7:308–12. [PMID: 18522888].
- Räty S, Sand J, Piironen A, Nordback I. Complications of palliative hepaticojejunostomy and gastrojejunostomy in unresectableperiampullary cancer: patient- and disease-related risk factors. Hepatogastroenterology 2006; 53:133–7. [PMID: 16506392].
- Evans DC, Martindale RG, Kiraly LN, Jones CM. Nutrition optimization prior to surgery. Nutr Clin Pract 2014; 29:10–21. [PMID: 24347529].
- Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364:1817–25. [PMID: 21561347].
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013; 369:1691–703. [PMID: 24131140].
- Eguchi H, Yada K, Shibata K, Matsumoto T, Etoh T, Yasuda K, et al. Laparoscopic stomach-partitioning gastrojejunostomy is an effective palliative procedure to improve quality of life in patients with malignant gastroduodenal outlet obstruction. Asian J Endosc Surg 2012; 5: 153-6. [PMID: 22994415].
- Berti S, Ferrarese A, Feleppa C, Francone E, Martino V, Bianchi C, et al. Laparoscopic perspective for distal biliary obstruction. Int J Surg 2015; 21: 564-7. [PMID: 26118614].
- Mizuguchi Y, Nakamura Y, Uchida E. Modified laparoscopic biliary enteric anastomosis procedure using handmade double-armed needles. Asian J Endosc Surg 2016; 9: 93-6. [PMID: 26781538].



