Keywords
Neuroendocrine Tumors; Prognosis; World Health
Organization
Abbreviation
NECs neuroendocrine carcinomas; NETs
neuroendocrine tumors
INTRODUCTION
Pancreatic neuroendocrine neoplasms, rare tumors
of the pancreas that constitute 1–2% of all pancreatic
malignancies, are a highly heterogeneous mixture of tumors
that originate from pluripotent stem cells [1, 2]. Their
biological behavior varies widely from nearly benign
tumors to malignant ones that give rise to metastasis and
local invasion. Most are known as slow growing tumors
and demonstrate better prognosis than pancreatic
ductal adenocarcinoma (PDAC) [3, 4]. Despite numerous
reports on newly diagnosed pancreatic neuroendocrine
neoplasms, their biological behavior is still not fully
understood. In particular, identifying the prognostic
factors for pancreatic neuroendocrine neoplasms
has been challenging because of their rarity and
heterogeneous nature [5]. World Health Organization
(WHO) classification 2010 classifies neuroendocrine
neoplasms based on their Ki67 and Mitotic indexes [6],
and it is not only the most widely accepted classification
and grading system, but also valuable in predicting
prognosis [7]. In 2017, the WHO classification will be
updated on the basis of recent evidence.
WHO Classification 2010
The European Neuroendocrine Tumor Society (ENETS)
proposed classifying neuroendocrine neoplasms into
well differentiated neuroendocrine tumors (NETs) and
poorly differentiated neuroendocrine carcinomas (NECs)
based on Ki67 and Mitotic indexes for the first time in
2007; the classification correlates favorably with patient
prognosis [8]. Subsequently, under WHO classification
2010, neuroendocrine neoplasms have been divided into
three grades by adopting the ENETS classification (Table
1): NET G1 (Ki67 index ≤2% and Mitotic index <2/10 high
power field (HPF)), NET G2 (Ki67 index 3-20% or Mitotic
index 2-20/10 HPF) and NEC (Ki67 index >20% or Mitotic
index >20/10 HPF) [6]. The efficacy of the classification
criteria in terms of predicting prognosis has been validated
in numerous studies including a large international cohort
study which included 1072 patients, whereby the 5-year
survival rate of NET G1 is about 95%, of NET G2 about 75%
and of NEC about 25% (Figure 1) [7].
Figure 1. Prognosis in pancreatic neuroendocrine neoplasms under WHO classification 2010.
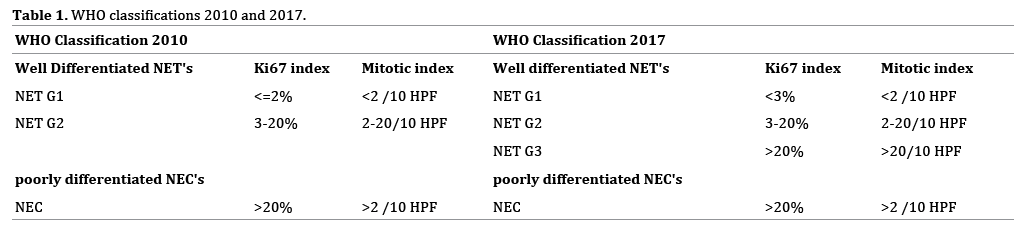
WHO Classification 2017
Recent studies have shown that NECs under WHO
classification 2010 is heterogeneous; it comprises well
differentiated and poorly differentiated groups in terms of
pathological differentiation, and well differentiated groups
demonstrate significantly better prognosis than poorly
differentiated ones [9, 10]. Therefore, neuroendocrine
neoplasms need to be subdivided on the basis of not
only Ki67 and Mitotic indexes, but also pathological
differentiation.
Under WHO classification 2017 (Table 1),
neuroendocrine neoplasms are primary classified into well differentiated NETs and poorly differentiated NECs
based on pathological differentiation. Subsequently, well
differentiated NETs are classified into NET G1 (Ki67
index <3% and Mitotic index <2/10 HPF), NET G2 (Ki67
index 3-20% or Mitotic index 2-20/10 HPF) and NET G3
(Ki67 index >20% or Mitotic index >20/10 HPF). Poorly
differentiated NECs are classified as NEC G3 (Ki67 index
>20% or Mitotic index >20/10 HPF). In consequence, NECs
under WHO classification 2010 came to be subdivided
into two groups under WHO classification 2017; well
differentiated groups are NET G3 and poorly differentiated
groups are NEC G3 [11].
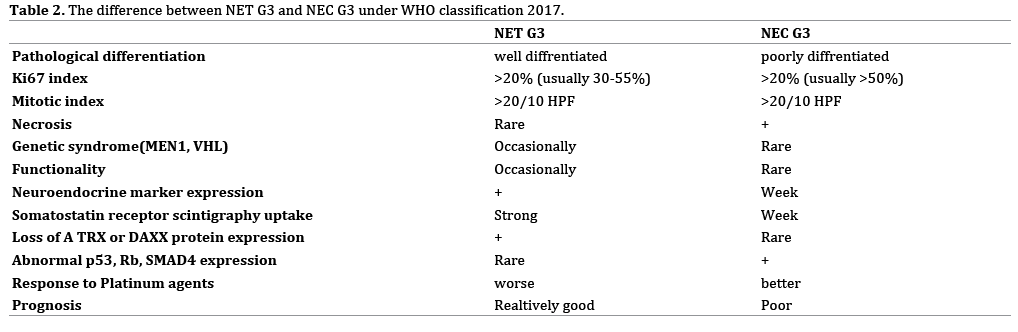
The differences between NET G3 and NEC G3 are
summarized in Table 2. The usual Ki67 index for NET
G3 and NEC G3 is 30-55% and >50%, respectively.
NET G3 has neuroendocrine marker (Chromogranin
A and Synaptophysin) expression, somatostatin
receptor scintigraphy uptake and loss of alpha
thalassemia/mental retardation syndrome X-linked
(ATRX) or death-domain associated protein (DAXX)
protein expression. On the other hand, NEC G3 has
abnormal Rb, p53, SMAD4 expression, and tumor
necrosis is commonly observed [12, 13, 14]. NEC G3
rarely involves genetic syndromes like MEN1 or von
Hippel-Lindau disease, and rarely has any function.
NEC G3 has a poor prognosis, but a better response to
platinum agents than does NET G3 [10, 15].
Since the population of pancreatic NET G3 and NEC
G3 is small, their precise prognosis has not been well
understood. There has been a small retrospective study
which included 50 patients with NET G2, 19 patients
with NET G3, and 42 patients with poor ly differentiated NECs. In this study, the 5-year survival rate of NETG3
has been estimated at about 29% and that of NEC
G3 at about 16% (Figure 2) [9]. The prognosis of
pancreatic neuroendocrine neoplasms under new WHO
classification 2017 has to be further evaluated in largescale
studies.
Figure 2. Prognosis in Pancreatic NET G2, G3 and NEC G3 under WHO classification 2017.
Other alterations in WHO classification 2017 include
the cutoff value of the Ki67 index for NET G1/G2; several
studies have shown that a Ki67 index of 5% or 10% is a
better cutoff value than one of 2% [7, 16, 17]. Nonetheless,
this classification shows a slightly different threshold
Ki67 index of 3%, which might not significantly affect the
prognosis of NET G1 and G2.
TNM Classification
Like other tumors, pancreatic neuroendocrine
neoplasms are also classified by tumor/node/metastasis
(TNM) classification. WHO classification is a malignancy
grading based on the biological behavior of neuroendocrine
neoplasms; on the other hand, TNM classification is a
clinical staging for mortality risk assessment based on
the anatomical extent of neuroendocrine neoplasms. Two
major TNM classifications of pancreatic neuroendocrine
neoplasms have been proposed by ENETS and the
American Joint Cancer Committee/Union for International
Cancer Control (AJCC/UICC). The ENETS TNM is specifically
designed for pancreatic neuroendocrine neoplasms; on
the other hand, the AJCC/UICC TNM classification (7th
edition) is primarily designed for PDAC [18]. Compared
with PDAC, pancreatic NETs are slow growing tumors,
large at diagnosis, limited to the pancreas and metastasize
during the late course of the disease. Thus, several studies
have shown that the ENETS classification of TNM is more accurate than that of AJCC/UICC (7th edition) and
is recommended for use on pancreatic neuroendocrine
neoplasms [7].
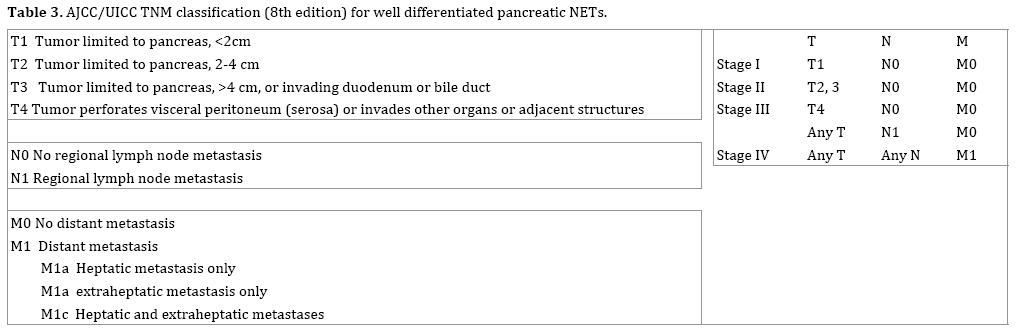
In 2016, the AJCC/UICC TNM classification was revised
and updated to the 8th edition (Table 3) [19]. In the
revision, pancreatic neuroendocrine neoplasms are divided
into two groups based on the Ki67 and Mitotic indexes:
well differentiated pancreatic NETs are defined as those
with a Ki67 index of ≤20% and a Mitotic index of ≤20/10
HPF; high-grade pancreatic NECs are defined as those with
a Ki67 index of >20% or a Mitotic index of >20/10 HPF.
Well differentiated pancreatic NETs are classified similar
to the ENETS TNM classification and high-grade pancreatic
NECs are classified as PDAC. The prognostic value of the
AJCC/UICC TNM classification (8th edition) for pancreatic
neuroendocrine neoplasms needs to be validated through
a large-scale study.
Further Prognostic Factors
Besides WHO classification and TNM classification,
numerous studies have described further prognostic factors
to enhance the stratification of pancreatic neuroendocrine
neoplasms, which include clinicopathological, radiological,
molecular and genetic features.
The presence of liver metastasis has been mentioned as
one of the most valuable prognostic factors in the ENETS
guidelines [20, 21]. The prognosis of patients with stage IV
pancreatic neuroendocrine neoplasms is a heterogeneous
because metastatic sites, number, or metastatic pattern are
not specified in the present TNM classifications. There have
been some studies described the liver metastatic pattern
as prognostic factors [22]. The extent of liver metastasis
either unilobar, bilobar or the presence of the extraabdominal
metastasis is a predictor of overall survival.
Nonetheless, the clinical impact of distant metastasis as
prognostic factors is still controversial and can change
greatly with advances in the treatment [23].
As for the radiological features, the calcification on
computed tomography, the status of 18F-fluorodeoxy
glucose uptake on 18F-fluorodeoxyglucose positron emission
tomography (FDG-PET) and the status of somatostatin
receptor scintigraphy (SRS) uptake have been described as
prognostic factors [24, 25, 26]. Previous study has shown
that calcified pancreatic neuroendocrine neoplasms on
preoperative computed tomography were predictive of NET
G2 as opposed to NET G1 and correlate with lymph node
involvement [24]. Others reported that the patients with
FDG-PET-positive and/or SRS-negative had a worse overall survival than those with FDG-PET- negative and/or SRSpositive
[25, 26]. We have recently published a study that
focused on the tumor invasion; the patients with stenosis
and upstream dilatation of the main pancreatic duct on preoperative
magnetic resonance cholangiopancreatography
had worse recurrence-free-survival than did those without
involvement [27].
As for the molecular biological markers, plasma
chromogranin A, loss of DAXX or ATRX, loss of
heterozygosity (LOH) of the pleckstrin homology like domain
family A member 3 (PHLDA3) gene, have been described as
prognostic factors [28, 29, 30, 31, 32, 33]. Chromogranin A
is a known diagnostic tumor marker for neuroendocrine
neoplasms. Previous studies have shown that the increase of
plasma chromogranin A levels is associated with poor clinical
outcomes for the patients with pancreatic neuroendocrine
neoplasms [28, 29]. Mutations in DAXX or ATRX have been
detected in 40% of pancreatic neuroendocrine neoplasms.
These mutations were associated with better clinical outcome
[30]. Loss of DAXX or ATRX is associated with chromosome
instability in pancreatic neuroendocrine neoplasms and
correlated with tumor stage and metastasis, reduced time of
relapse-free survival, and decreased time of tumor-associated
survival [31]. PHLDA3 have a tumor suppressive function of
pancreatic neuroendocrine neoplasms via repression of Akt
activity and various Akt-regulated biological processes. The
patients exhibiting LOH at the PHLDA3 locus seemed to have
a poorer prognosis compared with the patients without LOH
[32, 33].
Various novel prognostic factors based on
clinicopathological, radiological, and genetic features are
increasingly identified and contributed to more detailed
prognostic stratification in association with the WHO
classification and TNM classification.
CONCLUSION
The WHO classification is useful to predict the prognosis
and select proper therapeutic options of the pancreatic
neuroendocrine neoplasms. Recent studies have shown
that NECs under WHO classification 2010 comprises well
differentiated and poorly differentiated groups in terms
of pathological differentiation, and well differentiated
groups demonstrate significantly better prognosis than poorly differentiated ones. The WHO classification has
been updated in 2017 and NECs under WHO classification
2010 came to be subdivided into well differentiated NET
G3 and poorly differentiated NEC G3. In addition to WHO
classification, TNM classification and further prognostic
factors are also valuable to predict the prognosis. In this
review, we described the alterations in the latest upgrade
of these classifications and introduced further prognostic
factors.
Conflict of Interest
The authors have no financial conflicts of interest
concerning the manuscript to disclose.
References
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, Mares JE, et al. One hundred years after "carcinoid": epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008; 26:3063-72. [PMID: 18565894].
- Modlin IM, Oberg K, Chung DC, Jensen RT, de Herder WW, Thakker RV, et al., Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol 2008; 9:61-72. [PMID: 18177818].
- Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas 2010; 39:707-12. [PMID: 20664470].
- Fischer L Kleeff J, Esposito I, Hinz U, Zimmermann A, Friess H, et al., Clinical outcome and long-term survival in 118 consecutive patients with neuroendocrine tumours of the pancreas. Br J Surg 2008; 95:627-35. [PMID: 18306152].
- Halfdanarson TR, Rabe KG, Rubin J, Petersen GM. Pancreatic neuroendocrine tumors (PNETs): incidence, prognosis and recent trend toward improved survival. Annals of Oncology 2008; 19:1727-33. [PMID: 18515795].
- Bosman FT, Carneiro F, Hruban RH, Theise ND. WHO Classification of Tumours of the Digestive System 4th ed. Lyon: IARC, 2010.
- Rindi G Falconi M, Klersy C, Albarello L, Boninsegna L, Buchler MW, et al., TNM staging of neoplasms of the endocrine pancreas: results from a large international cohort study. J Natl Cancer Inst 2012; 104: 764-77. [PMID: 22525418].
- Pape UF, Jann H, Müller-Nordhorn J, Bockelbrink A, Berndt U, Willich SN, et al., Prognostic relevance of a novel TNM classification system for upper gastroenteropancreatic neuroendocrine tumors. Cancer 2008; 113:256-65. [PMID: 18506737].
- Basturk O Yang Z, Tang LH, Hruban RH, Adsay V, McCall CM, et al. The high-grade (WHO G3) pancreatic neuroendocrine tumor category is morphologically and biologically heterogenous and includes both well differentiated and poorly differentiated neoplasms. Am J Surg Pathol 2015; 39:683-90. [PMID: 25723112].
- Vélayoudom-Céphise FL Duvillard P, Foucan L, Hadoux J, Chougnet CN, Leboulleux S, et al. Are G3 ENETS neuroendocrine neoplasms heterogeneous? Endocr Relat Cancer 2013; 20:649-57. [PMID: 23845449].
- Lloyd RV, Osamura RY, Klöppel G, Rosai J. WHO Classification of Tumours of Endocrine Organs 4th ed. Lyon: IARC, 2017.
- Basturk O, Tang L, Hruban RH, Adsay V, Yang Z, Krasinskas AM, et al., Poorly differentiated neuroendocrine carcinomas of the pancreas: a clinicopathologic analysis of 44 cases. Am J Surg Pathol 2014; 38:437-47. [PMID: 24503751].
- Tang LH, Basturk O, Sue JJ, Klimstra DS. A Practical Approach to the Classification of WHO Grade 3 (G3) Well-differentiated Neuroendocrine Tumor (WD-NET) and Poorly Differentiated Neuroendocrine Carcinoma (PD-NEC) of the Pancreas. Am J Surg Pathol 2016; 40:1192-202. [PMID: 27259015].
- Yachida S, Vakiani E, White CM, Zhong Y, Saunders T, Morgan R, et al., Small cell and large cell neuroendocrine carcinomas of the pancreas are genetically similar and distinct from well-differentiated pancreatic neuroendocrine tumors. Am J Surg Pathol 2012; 36:173-84. [PMID: 22251937].
- Sorbye H, Welin S, Langer SW, Vestermark LW, Holt N, Osterlund P, et al., Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): the NORDIC NEC study. Ann Oncol 2013; 24:152-60. [PMID: 22967994].
- Scarpa A, Mantovani W, Capelli P, Beghelli S, Boninsegna L, Bettini R, et al., Pancreatic endocrine tumors: improved TNM staging and histopathological grading permit a clinically efficient prognostic stratification of patients. Mod Pathol 2010; 23:824-33. [PMID: 20305616].
- Khan MS, Luong TV, Watkins J, Toumpanakis C, Caplin ME, Meyer T.A comparison of Ki-67 and mitotic count as prognostic markers for metastatic pancreatic and midgut neuroendocrine neoplasms. Br J Cancer 2013; 108:1838-45. [PMID: 23579216].
- Rindi G, Klöppel G, Alhman H, Caplin M, Couvelard A, de Herder WW, et al. TNM staging of foregut (neuro)endocrine tumors: a consensus proposal including a grading system. Virchows Arch 2006; 449:395-401. [PMID: 16967267].
- Brierley JD, Gospodarowicz M and Wittekind C, UICC TNM Classification of Malignant Tumours 8th ed. New York: Wiley-Blackwell, 2016.
- Steinmuller T, Kianmanesh R, Falconi M, Scarpa A, Taal B, Kwekkeboom DJ, et al. Consensus guidelines for the management of patients with liver metastases from digestive (neuro) endocrine tumors: foregut, midgut, hindgut, and unknown primary. Neuroendocrinology. 2008; 87:47–62. [PMID: 18097131].
- Falconi M, Eriksson B, Kaltsas G, Bartsch DK, Capdevila J, Caplin M, et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016; 103:153-71. [PMID: 26742109].
- Panzuto F, Merola E, Rinzivillo M, Partelli S, Campana D, Iannicelli E, et al. Advanced digestive neuroendocrine tumors: metastatic pattern is an independent factor affecting clinical outcome. Pancreas 2014; 43:212-8. [PMID: 24518498].
- Lee L, Igarashi H, Fujimori N, Hijioka M, Kawabe K, Oda Y, et al., Long-term outcomes and prognostic factors in 78 Japanese patients with advanced pancreatic neuroendocrine neoplasms: a single-center retrospective study. Jpn J Clin Oncol 2015; 45:1131-8. [PMID: 26378090].
- Poultsides GA Huang LC, Chen Y, Visser BC, Pai RK, Jeffrey RB, et al. Pancreatic neuroendocrine tumors: radiographic calcifications correlate with grade and metastasis. Ann Surg Oncol 2012; 19:2295-303. [PMID: 22396008].
- Binderup T Knigge U, Loft A, Federspiel B, Kjaer A. 18F-fluorodeoxyglucose positron emission tomography predicts survival of patients with neuroendocrine tumors. Clin Cancer Res 2010; 16:978-85. [PMID: 20103666].
- Garin E Le Jeune F, Devillers A, Cuggia M, de Lajarte-Thirouard AS, Bouriel C, et al., Predictive value of 18F-FDG PET and somatostatin receptor scintigraphy in patients with metastatic endocrine tumors. J Nucl Med 2009; 50:858-64. [PMID: 19443590].
- Nanno Y, Matsumoto I, Zen Y, Otani K, Uemura J, Toyama H, et al., Pancreatic Duct Involvement in Well-Differentiated Neuroendocrine Tumors is an Independent Poor Prognostic Factor. Ann Surg Oncol 2017; 24:1127-33. [PMID: 27822631].
- Rossi RE, Garcia-Hernandez J, Meyer T, Thirlwell C, Watkins J, Martin NG, et al. Chromogranin A as a predictor of radiological disease progression in neuroendocrine tumours. Ann Transl Med 2015; 3:118. [PMID: 26207246].
- Nanno Y, Toyama H, Matsumoto I, Otani K, Asari S, Goto T, et al. Baseline plasma chromogranin A levels in patients with well-differentiated neuroendocrine tumors of the pancreas: A potential predictor of postoperative recurrence. Pancreatology 2017; 17:291-294. [PMID: 28043759].
- Jiao Y, Shi C, Edil BH, de Wilde RF, Klimstra DS, Maitra A, et al., DAXX/ATRX, MEN and mTOR pathway genes are frequently altered in pancreatic neuroendocrine tumors. Science 2011; 331:1199-203. [PMID: 21252315].
- Marinoni I Kurrer AS Vassella E Dettmer M Rudolph T Banz V, et al., Loss of DAXX and ATRX are associated with chromosome instability and reduced survival of patients with pancreatic neuroendocrine tumors. Gastroenterology 2014; 146:453-60.e5. [PMID: 24148618].
- Kawase T Ohki R, Shibata T, Tsutsumi S, Kamimura N, Inazawa J, et al., PH Domain-Only Protein PHLDA3 Is a p53-Regulated Repressor of Akt. Cell 2009; 136:535-550. [PMID: 19203586].
- Ohki R, Saito K, Chen Y, Kawase T, Hiraoka N, Saigawa R, et al. PHLDA3 is a novel tumor suppressor of pancreatic neuroendocrine tumors. Proc Natl Acad Sci U S A 2014; 111:E2404-13. [PMID: 24912192].



