Yael R1, Stella B2 and Dan G1*
1Tel Aviv Sourasky Medical Center, Division of Gynecologic Oncology, Affiliated to the Sackler Faculty of Medicine, Tel Aviv University, Tel-Aviv, Israel
2Tel Aviv Sourasky Medical Center, Institute of Pathology, Affiliated to the Sackler Faculty of Medicine, Tel Aviv University, Tel-Aviv, Israel
*Corresponding Author:
Dan G, Tel Aviv
Sourasky Medical Center, Division of Gynecologic Oncology, Affiliated to the Sackler Faculty of Medicine, Tel Aviv University, Israel
Tel: 972-3-9625622
Fax: 972-3-9625670
E-mail: grisaro@post.tau.ac.il
Received date: October 11, 2015; Accepted date: November 25, 2015; Published date: November 27, 2015
Copyright: © 2015 Dan G, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Originally described at 1969 [1], Li freumani syndrome (LFS) is an inherited autosomal dominant cancer predisposition syndrome associated with TP53 mutations. Also known as the Sarcoma, Breast, Leukemia and Adrenal Gland (SBLA) cancer syndrome, it is manifested by a range of malignancies occurring at an unusual early age. In addition to the "core malignancies" after which it was named, other tumors have been reported less frequently, including melanoma, gastric cancer, lymphoma, Wilms tumor and colorectal carcinoma [2-4]. The female lifetime risk for tumor development is approximately 100% depending on mutation type [5,6] and for both sexes, once a first tumor is diagnosed, the probability of developing a second malignancy within the following 30 years is very high -57%. Sarcomas account for approximately 25% of tumors in patients with TP53 germline mutations with median age of onset at 15 years [7,8].
Case
Our 15 years old female LFS patient first presented with right temporomandigular rhabdomiosarcoma with lung metastases treated with surgery and chemoradiation when she was only 3 y.o. At the age of 11 she was diagnosed with osteogenic sarcoma involving the left TMJ that has metastasized to the lungs. Notably, using the Chompret criteria, multiple tumors, two of which belong to the LFS tumor spectrum and the first of which occurred before age 46 years are sufficient for the diagnosis [9]. Despite adjuvant chemotherapy, 4 years later a tumor reappeared adjacent to the mandibular stump obligating resection and reconstruction of parts of the left maxilla, zygoma and orbit. At 13, osteogenic sarcoma of the left fibula was surgically removed with neoadjuvant chemotherapy, but a year later, when it reoccurred, a below knee amputation was necessary. She first presented to our Gyneco-oncologic unit with a right labial mass. Biopsy indicated sarcoma. Despite her age, considering the harming affect of radiation, we recommended and performed partial right hemivulvectomy (Figure 1A). Final pathological report confirmed the diagnosis of low grade sarcoma and free surgical margins (Figure 1B).
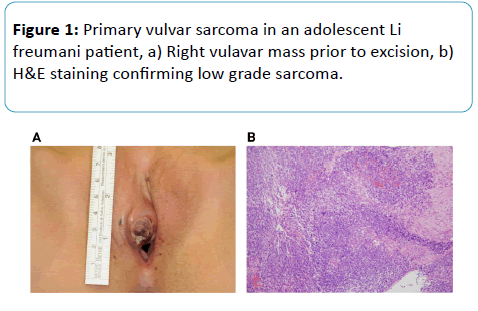
Figure 1: Primary vulvar sarcoma in an adolescent Li freumani patient, a) Right vulavar mass prior to excision, b) H&E staining confirming low grade sarcoma.
Discussion
Vulvar sarcomas are highly uncommon and account for 1.5-5% of all vulvar neoplasia [10,11]. Vulvar sarcomas in adolescent are even more rare, described only as several case reports [12,13]. To our knowledge, this is the first case of primary vulvar sarcoma in a LFS patient. This female is the only LFS patient out of 6 siblings. Being that this syndrome has a 100% penetrance, she probably carries a de novo mutation. As mention above, at 11 years of age, she was diagnosed with osteogenic sarcoma involving the left TMJ. This could be accounted, perhaps, to the radiation treatment she underwent. Accumulating data suggests that radiation induced cancers are more common in LFS [14,15] including one study in which half of the secondary sarcomas occurred in the radiation field [16]. It is now accepted that radiation should be avoided whenever possible.
Conclusion
The natural embarrassment delaying disclosure of genital findings at puberty and the importance of early diagnosis in sparing both mutilating surgery and hazardous radiation therapy obligates special attention by all caregivers.
References
- Li FP, Fraumeni JF (1969) Soft-tissue sarcomas, breast cancer, and other neoplasms. A familial syndrome?. Ann Intern Med 71: 747-52.
- Malkin D (2011) Li-fraumeni syndrome. Genes Cancer 2:475-84.
- Li FP, Fraumeni JF Jr, Mulvihill JJ, Blattner WA, Dreyfus MG, et al. (1988) A cancer family syndrome in twenty-four kindreds. Cancer Res 48: 5358-62.
- Gonzalez KD, Noltner KA, Buzin CH, Gu D, Wen-Fong CY, et al. (2009) Beyond Li Fraumeni Syndrome: clinical characteristics of families with p53 germline mutations. J Clin Oncol 27: 1250-1256.
- Chompret A, Brugières L, Ronsin M, M Gardes, F Dessarps-Freichey, et al. (2000) P53 germline mutations in childhood cancers and cancer risk for carrier individuals. Br J Cancer 82: 1932-1937.
- Lustbader ED, Williams WR, Bondy ML, Strom S, Strong LC (1992) Segregation analysis of cancer in families of childhood soft-tissue-sarcoma patients. Am J Hum Genet 51: 344-56.
- Olivier M, Goldgar DE, Sodha N, Ohgaki H, Kleihues P, et al. (2003) Li-Fraumeni and related syndromes: correlation between tumor type, family structure, and TP53 genotype. Cancer Res 63: 6643-6650.
- Ognjanovic S, Olivier M, Bergemann TL, Hainaut P (2012) Sarcomas in TP53 germline mutation carriers: a review of the IARC TP53 database. Cancer 118: 1387-1396.
- Tinat J, Bougeard G, Baert-Desurmont S, Stéphanie V, Cosette M, et al. (2009) 2009 Version of the Chompret criteria for Li Fraumeni syndrome. J Clin Oncol 27: e108-109.
- Ulutin HC, Zellars RC, Frassica D (2003) Soft tissue sarcoma of the vulva: A clinical study. Int J Gynecol Cancer 13: 528-531.
- Patrizi L, Corrado G, Saltari M, Perracchio L, Scelzo C, et al. (2013) Vulvar "proximal-type" epithelioid sarcoma: report of a case and review of the literature. Diagn Pathol. 8: 122.
- Tunitsky-Bitton E, Uy-Kroh MJ, Michener C, Tarr ME (2015) Primary Ewing Sarcoma Presenting as a Vulvar Mass in an Adolescent: Case Report and Review of Literature. J Pediatr Adolesc Gynecol. 28: e179-183.
- Yang J, Guo Q, Yang Y, Zhang J, Lang J, et al. (2012) Primary vulvar Ewing sarcoma/primitive neuroectodermal tumor: a report of one case and review of the literature. J Pediatr Adolesc Gynecol 25: e93-97.
- Hisada M, Garber JE, Fung CY, Fraumeni JF Jr, Li FP (1998) Multiple primary cancers in families with Li-Fraumeni syndrome. J Natl Cancer Inst 90: 606-611.
- Limacher JM, Frebourg T, Natarajan-Ame S, Bergerat JP (2001) Two metachronous tumors in the radiotherapy fields of a patient with Li-Fraumeni syndrome. Int J Cancer 96: 238-42.
- Heymann S, Delaloge S, Rahal A, Caron O, Frebourg T, et al. (2010) Radio-induced malignancies after breast cancer postoperative radiotherapy in patients with Li-Fraumeni syndrome. Radiat Oncol 5:104.

