Amir Houshang Mohammad Alizadeh
Research Center for Gastroenterology and Liver Diseases, Shahid Beheshti University of Medical Sciences, Taleghani Hospital, Tehran, Iran
*Corresponding Author:
Mohammad Alizadeh AH
Shahid Beheshti University of Medical Sciences, Talegani
Hospital, Parvaneh Ave, Tabnak St, Evin, Tehran, Iran. 19857
Phone +0098-21-22432521
Fax 0098-21-22432517
E-mail ahmaliver@yahoo.com
Received April 02nd, 2014-Accepted May 7th, 2015
Keywords
Echinococcus granulosus; Endosonography; Pancreas
Introduction
Cystic Echinococcosis is a near-cosmopolitan zoonosis caused by adult or larval stages of tiny cestode parasites belonging to the genus Echinococcus and the family Taeniidae [1, 2]. The genus Echinococcus consists of six species but four are of public health concern: Echinococcus granulosus (which gives rise to cystic hydatid disease), Echinococcus multilocularis (which causes alveolar echinococcosis), Echinococcus oligarthus (which cause polycystic echinococcosis). Recently two new species have been identified: Echinococcus shiquicus on the Tibetan plateau and Echinococcus felidis in African lions but to date no human infection have been described [2-4]. On a global basis, Echinococcus granulosus is the most common species and is responsible for 95% of the human cystic echinococcosis cases reported [5].
Infected Organs
The annual incidence of hydatid disease has been reported to be 18 to 20 cases per 100.000 inhabitants [6]. The liver and lungs act as the primary filtering beds with their vast capillary network and hence are the organs most frequently (90% of cases) involved in human echinococcosis. Primary pancreatic involvement (without liver or lung disease) is found in less than 1% of the various sites of hydatid disease, about 0.2 % of abdominal locations and less than 1% in those countries where the disease is endemic [7-12]. Pancreatic infestation is mainly by hematogenous dissemination, local spread via pancreatobiliary ducts, and peripancreatic lymphatic invasion [12-15]. Clinical presentation varies with size of the cyst and anatomic location. The hydatid cyst of the pancreas is mainly located in the head (57%), followed by the body (24-34%) and the tail (16-19%) [14]. The relatively higher frequency in the pancreatic head can be explained by the fact that the head region is the most vascularized [16].
Clinical Symptoms and Complications
The clinical presentation of hydatid disease of the pancreas is variable depending on the size and anatomical location of the cyst [17]. An abdominal mass, epigastric pain, weight loss, discomfort and vomiting are the main clinical symptoms [18-20]. Cyst in head of pancreas can cause obstructive jaundice [14, 19-23]. Accordingly, two hypotheses are posited: main pancreatic duct compression caused by the cyst itself [24] and main pancreatic duct obstruction by hydatid scolices’ migration from the hydatid cyst [25-28]. Also, cholangitis, duodenal stenosis or fistula, acute and chronic pancreatitis, pancreatic abscess and pancreatic fistula are unusual complications of hydatid cysts involving the head of the pancreas [29-33]. Cysts located in the body or tail of the pancreas can be symptomless and may be detected by the presence as an abdominal mass [34, 35]. Mesenteric vein thrombosis, the compression of splenic vein causing portal hypertension, rupture into the biliary three or into the peritoneal cavity, gastrointestinal tract and abcess formation are uncommon presentations of cysts in the body and tail [21, 23, 36]. Increased bilirubin, ALP, ALT, AST, amylase and lipase have been reported in these patients [37-49].
Diagnosis- Imaging techniques
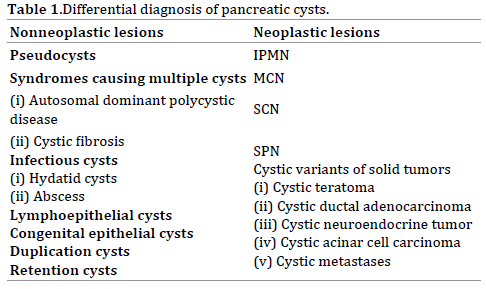
The preoperative diagnosis of hydatid cysts is very difficult. Establishing a precise diagnosis may be difficult because the presenting symptoms and the findings of clinical investigations may be similar to some other more commonly encountered cystic lesions of the pancreas [50]. Cystic lesions of the pancreas (CLP) are relatively common and differentiating among these cysts is challenging. CLPs include pseudocysts, retention cysts, duplication cysts, lymphoepithelial cysts, congenital epithelial cysts, cysts which occur in association with polycystic disease or von Hippel-Lindau disease, serous cystic adenomas (SCA), mucinous cystic neoplasms (MCN), intraductal papillary mucinous tumors (IPMN), solid pseudopapillary tumors (SPN), cystic metastases from cancer of the lung, ovary, or melanoma, vascular tumours (haemangioma or lymphangioma) and primary hydatid disease of the pancreas (Table 1) [51-57].
Imaging modalities range from simple to complex and invasive. Ultrasound is readily available and cost effective. The diagnostic sensitivity of abdominal ultrasound in abdominal echinoccosis in general ranges from 93-98% [3, 58, 59], but it may be less accurate with pancreatic lesions, due to the difficulty in visualisation of the pancreas. Abdominal CT scan shows the presence of a cyst in the pancreas with no enhancement on contrast. The classical imaging features of hydatid cysts include a multivesicular cyst containing daughter cysts, ‘hydatid sand’ (layering of scolices in the cyst), ‘water lily sign’ (floating membrane within the cyst), Cyst wall calcification and hyper-intense cyst wall on plain CT [60]. Magnetic resonance imaging shows the characteristic low-signal intensity rim of hydatid cyst on T2-weighted images and is superior in demonstrating irregularities of the rim. These irregularities represent incipient detachment of the membranes [61]. Although the presence of cystic lesions of the pancreas are easily identified by ultrasound, CT scan and magnetic resonance imaging (MRI), these methods have limited sensitivity in making a specific diagnosis because of the considerable overlap of imaging features [62]. A specific diagnosis is seldom made preoperatively unless hydatid disease is suspected. Since its early introduction in the early 1990’s, EUS has emerged as a safe and accurate technique for the diagnosis, stage, and treat a variety of lesions. A particularly useful aspect of EUS is the enhanced imaging of the pancreas [63].
Endoscopic ultrasound involves placing small, highfrequency ultrasound transducers on the tips of fiberoptic or video-endoscopes [64]. With several technological improvements, such as the introduction of electronic transducers and color-doppler capability, EUS is able to gain accurate images, with high negative predictive value, ranging from 87 to 100% [65, 66]. By placing the transducer within the gut lumen, EUS overcomes the two major technologic problems for pancreatic imaging by transcutaneous ultrasound; obscuring overlying gas filled bowel and the necessity to use low frequency and therefore low resolution ultrasound to penetrate to the depth of the pancreas [64].The strict proximity between the transducer and the lesions allows for a very precise definition of the structural component of the cysts and some components of pancreatic cysts, are better visualized with EUS than with other modalities [67]. Sensitivity of EUS in pancreatic mass detection can reach 97%, with a better yield than transabdominal US and conventional CT scan, mainly with small size lesions (<3 cm) [68]. EUS can accurately show the relationship between the cyst and pancreatic duct [69]. Endoscopic ultrasound provides more detailed morphological information as well as the opportunity for biochemical and cytological sampling which helps in differentiating hydatid cysts from other cystic pancreatic lesions. Aspiration of cyst fluid for (cytologic and/or chemical) analysis or biopsy of the cyst wall has been recommended as methods of distinguishing hydatid cysts of the pancreas from more commonly occurring pseudocysts or cystic tumours [70]. EUS now allows combining the biopsy (EUS-guided fine needle aspiration) and therapeutic capabilities of EUS (eg. tumor injection therapy or celiac neurolysis) with the initial diagnostic procedure [67]. The first EUS-FNA of a pancreatic lesion was reported in 1994 and there have been numerous series since then [71-77]. EUS-FNA techniques has been described extensively elsewhere [78- 82] and involve passing an 18 to 25 (usually 22) gauge stainless steel, echogenic aspiration needle through the biopsy port of an echoendoscope under real-time guidance into an endosonographically visualized pancreatic lesion or fluid collection. The needle is moved back and forth through the lesion with varying degrees of suction applied to it and the sample is deposited on a cytology slide(s) for immediate staining and cytopathologic examination [64]. EUS-FNA is the most cost-effective modality as primary approach and it is able to change patient management as previously reported [83, 84]. Moreover, EUS-FNA has a lower risk of needle tract seeding when compared with a percutaneous approach due to a short needle track, which does not pass through peritoneal or pleural surfaces [85]. EUS-FNA can provide material for a cytologic diagnosis in up to 80% of cases of pancreatic cystic lesions [86-90]. Major complications related to EUS-FNA of pancreatic cystic lesions include acute pancreatitis (0.85%) [91, 92], abdominal pain (0.56%) [91], hemorrhage within the cyst (<1%) [87, 88, 89], infection and fever (0.85%) [88- 92]. The history of acute or chronic pancreatitis was not associated with higher risk [91]. Overall, the accuracy for diagnosing various cystic lesions by EUS-FNA is 54% to 97% [86-90, 93]. Finally, when EUS is combined with its sister endoscopic procedure, therapeutic ERCP, it results in a powerfully efficient combination of diagnostic, staging and therapeutic techniques that are very difficult to match with any other set of procedures [94]. However, EUS, although operator dependent, can be very useful, particularly when CT or RMN are equivocal [67] and due to these advantages, EUS has evolved into an important technique to assess cystic lesions of the pancreas [95].
Conclusion
Pancreatic hydatid cyst is a parasitic infestation that is rare with a reported frequency of 0.1-2% of all cases of hydatid disease. Anatomy of the pancreas may cause difficulties in making the diagnosis. Preoperative diagnosis of pancreatic hydatid cysts is challenging, as its radiologic findings are often mistaken for other cystic lesions of the pancreas. Endoscopic ultrasound is useful in the diagnosis of pancreatic hydatid disease. EUS with its capabilities for fluid sampling for biochemistry and cytology is a very useful discriminates.
Conflicting Interest
The authors had no conflicts of interest
References
- Kul O, Yildiz K. Multivesicular cysts in cattle: characterisation of unusual hydatid cyst morphology caused by Echinococcusgranulosus. Vet. Parasitol. 2010; 170(1-2):162-6. [PMID: 20207486]
- Prathiush PR, D’Souza PE, Gowda AKJ. Diagnosis of Echinococcus granulosus infection in dogs by a coproantigen sandwich ELISA. Vet. Arhiv. 2008; 78:297-305.
- Shaw JM, Bornman PC, Krige JEJ. Hydatid disease of the liver. SAJS 2006; 44(2): 70-77.
- Moro P, Schantz PM. Echinococcosis: a review. Int. J. Infect. Dis. 2009; 13:125-133. [PMID: 18938096]
- Akbulut S, Yavuz R, Sogutcu N, Kaya B, Hatipoglu S, Senol A, et al. Hydatid cyst of the pancreas: Report of an undiagnosed case of pancreatic hydatid cyst and brief literature review.World J. Gastrointest. Surg. 2014; 27:6(10):190-200. [PMID: 25346801]
- Sirwar SB, Indupalli AS, Subhanulla P. Retroperitoneal hydatd cyst: a pare presentation. J. Med. Dent. Sci. 2012; 1(3):176.
- Khiari A, Mzali R, Ouali M, Kharrat M, Kechaou MS, Beyrouti MI: Hydatid cyst of the pancreas. Apropos of 7 cases. Ann. Gastroenterol. Hepatol. 1994; 30:87-91. [PMID: 8067682]
- Derbel F, Zidi MK, Mtimet A, Hamida MBH, Mazhoud J, Youssef S, et al. Hydatid cyst of the pancreas: A report on seven cases. Arab. J. Gastroenterol. 2010; 11:219-22.
- Nisar A. Bhat, Kumar Abdul Rashid, ImtiazWani, ShadabWani, AbeerSyeed: Hydatid cyst of the pancreas mimicking choledochal cyst. Ann. Saudi. Med. 2011; 31(5). [PMID: 21911995]
- Abi F. Unusual localisation of hydatid cyst. Apropos of 40 Cases. J. Chir. 1989;126:307-12. [PMID: 2663895]
- Serhal S, Sebai F, Mestiri S. Hydatid cyst of the pancreas. Apropos of 3 cases. J. Chir. 1987;124:542-4.
- Kayabali I, Gokcora IH, Ormeci N. Surgical treatment of hydatid cysts of the pancreas. Int. Surg. 1991;76:185-8.
- Brown RA, Millar AJ, Steiner Z, Krige JE, Burkimsher D, Cywes S. Hydatid cyst of the pancreasa case report in child. Eur. J. Pediatr. Surg. 1995; 5:121-4. [PMID: 7612583]
- Ozmen MM, Moran M, Karakahya M, Coskun F. Recurrent acute pancreatitis due to a hydatid cyst of the pancreatic head: a case report and review of the literature. JOP. J. Pancreas. 2005; 6:354-8.
- Gonzalez EP, Gil-Grande L, del Arbol LR, del Pozo D, Miquel J, Vazquez M, et al. Presinusoidal portal hypertension secondary to portal invasive echinococcosis. J. Clin. Gastroenterol. 2002; 34:103-4. [PMID: 11743260]
- Jai SR, El Hattabi K, Bensardi F, Chehab F, Khaiz D, Bouzidi A. Primary hydatid cyst of the pancreas causing obstructive jaundice. Saudi. J. Gastroenterol. 2007; 13:191-193. [PMID: 19858645]
- Trigui A, Rejab H, Guirat A, Mizouni A, Ben Amar M, Mzali R, et al. Hydatid cyst of the pancreas about 12 cases. Ann. Ital. Chir. 2013; 84:165-170. [PMID: 23697975]
- Erdener A, Sahin AH, Özcan C. Primary pancreatic hydatid disease in a child: case report and review of the literature. J. Pediatric. Surgery. 1999; 34:491-492. [PMID: 10211664]
- Makni A, Jouini M, Kacem M, Ben Safta Z. Acute pancreatitis due to pancreatic hydatid cyst: a case report and review of the literature. WJES 2012; 7:7. [PMCID: 3325852]
- Moosavi SR, KhajoueiKermany H. Epigastric mass due to a hydatid cyst of the pancreas. A case report and review of the literature. JOP. J Pancreas 2007; 8(2):232-234. [PMID: 17356249]
- Safioleas MC, Moulakakis KG, Manti C, Kostakis A. Clinical considerations of primary hydatid disease of the pancreas. Pancreatology 2005; 5:457-461.
- Krige JEJ, Mirza K, Bornman PC, Beningfield SJ. Primary hydatid cysts of the pancreas. SAJS 2005; 43(2):37-40.
- Jai SR, El Hattabi K, Bensardi F. Primary hydatid cyst of the pancreas causing obstructive jaundice. Saudi J Gastroenterol 2007; 13(4):191-193. [PMID: 19858645]
- Sinha AN, Rao AS, Vyas HG. Hydatid cyst in head of pancreas presenting with obstructive jaundice.Inadia. J. Gastroenterol. 1997; 16:32. [PMID: 9167380]
- Sebbag H, Partensky C, Roche J, Ponchon T, Martins A. Recurrent acute pancreatitis from the rupture of a solitary pancreatic hydatid cyst into Wirsung’s canal. Gastroenterol. Clin. Biol. 1999; 23:793-794.
- Pouget Y, Mucci S, O’Toole D, Lermite E, Aubé C, Hamy A. Recurrent acute pancreatitis revealing a hydatid cyst of the pancreas. Rev. Med. Interne. 2009; 30:358-360. [PMID: 18818003]
- Diop SP, Costi R, Le Bian A, Carloni A, Meduri B, Smadja C. Acute pancreatitis associated with a pancreatic hydatid cyst: understanding the mechanism by EUS. Gastrointest. Endosc. 2010; 72:1312-1314.
- Coskun T, Kama NA, Dener C, Gözalan U. Primary hydatid disease of the pancreas. Am. J. Gastroenterol. 1997; 92: 899-900.
- Cosme A, Orive V, Ojeda E, Aramburu V, Irazusta M, Arenas JI. Hydatid cyst of the head of the pancreas with spontaneous fistula to the duodenum. Am. J. Gastroenterol. 1987; 82: 1311-1313. [PMID: 3687907]
- Wong LS, Braghirolli-Neto O, Min Zu, Buckels JAC, Mirza DF. Hydatid liver disease as a cause of recurrent pancreatitis. J. R. Coll. Surg. Edin. 1999; 44:407-409. [PMID: 10612965]
- Mathai V, Banerjee Jesudason SR, Muthusami JC, Kuruvilla R, Idikula J, Sada P. Chronic pancreatitis caused by intraductalhydatid cysts of the pancreas. Br. J. Surg. 1994; 81:1029. [PMID: 7922055]
- Papadimitriou J. Pancreatic abscess due to infected hydatid disease. Surgery. 1987; 102:880-882. [PMID: 3672327]
- Ismail K, Haluk GI, Necati Ö. Surgical treatment of hydatid cysts of the pancreas. Int. Surg. 1991; 76:185-188. [PMID: 1938210]
- Andrew WK, Glynn TR. Hydatid cyst of the pancreas tail. S. Afr. Med. J. 1981; 59:235-236.
- Du Toit DF, Loxton AJ, Laker L, Dreyer JF. Hydatid cyst of the pancreatic tail. S. Afr. Med. J. 1984; 66: 781-782.
- Placer C, Martin R, Sanchez E, Soleto E. Rupture of abdominal hydatid cysts. Br. J. Surg. 1988; 75: 157.
- Yarlagadda P, Yenigalla BM, Penmethsa U, Myneni RB. Primary pancreatic echinococcosis. Trop. Parasitol. 2013; 3:151-154. [PMID: 24471002]
- Baghbanian M, Salmanroghani H, Karegar S, Binesh F, Baghbanian A. Pancreatic Tail Hydatid Cyst as a Rare Cause for Severe Acute Pancreatitis: A Case Report. Govaresh. 2013; 18:57-61.
- Mandelia A, Wahal A, Solanki S, Srinivas M, Bhatnagar V. Pancreatic hydatid cyst masquerading as a choledochal cyst. J. Pediatr. Surg. 2012; 47:e41-e44. [PMID: 23164030]
- Suryawanshi P, Khan AQ, Jatal S. Primary hydatid cyst of pancreas with acute pancreatitis. Int. J. Surg. Case Rep. 2011; 2:122-124. [PMID: 3199727]
- Somani K, Desai AA. An unusual case of pancreatic hydatid cyst mimicking choledochal cyst. BHJ 2011: 53: 103-105.
- Bhat NA, Rashid KA, Wani I, Wani S, Syeed A. Hydatid cyst of the pancreas mimicking choledochal cyst. Ann. Saudi. Med. 2012; 31:536-538. [PMIC: 3183692]
- Cankorkmaz L, Gümüs C, Celiksöz A, Köylüoglu G. Primary hydatid disease of the pancreas mimicking pancreatic pseudo-cyst in a child: case report and review of the literature. Turkiye. Parazitol. Derg. 2011; 35:50-52. [PMID: 21618194]
- Agrawal S, Parag P. Hydatid cyst of head of pancreas mimicking choledochal cyst. BMJ Case Rep. 2011. [PMIC: 3128356]
- Derbel F, Zidi MK, Mtimet A. Hydatid cyst of the pancreas: A report on seven cases. AJG 2010; 11:219-222.
- Bansal VK, Misra MC, Krishna A, Kumar S, Garg P, Khan RN, et al. Pancreatic hydatid cyst masquerading as cystic neoplasm of pancreas. Trop. Gastroenterol. 2010; 31:335-337. [PMID: 21568157]
- Shah OJ, Robbani I, Zargar SA, Yattoo GN, Shah P, Ali S, et al. Hydatid cyst of the pancreas. An experience with six cases. JOP 2010; 11:575-581. [PMID: 21068489]
- Karakas E, Tuna Y, Basar O, Koklu S. Primary pancreatic hydatid disease associated with acute pancreatitis. HepatobiliaryPancreat. Dis. Int. 2010; 9:441-442. [PMID: 20688612]
- Elmadi A, Khattala K, Elbouazzaoui A, Rami M. Acute cholangitis revealing a primary pancreatic hydatid cyst in a child]. J. de. Pediatrie. Et. De. Puericulture. 2010; 23:201-203. [PMID: 17483783]
- Cankorkmaz L, Gumus C, Celiksoz A, Koyluoglu1 G. primary hydatid disease of the pancrease of the pancreas mimicking pancreatic pseudo cyst in a child: case report and review of the literature. TurkiyeParazitol. Derg. 2011; 35:50-2.
- Le Borgne J. Cystic tumours of the pancreas. Br. J. Surg. 1998; 85:577-579.
- Astiz JM, Astiz L, Buzzi A. Primary hydatid cyst mistaken for carcinoma of the pancreas. J. R. Soc. Med. 1997; 90:334. [PMC ID: 1296312]
- Box JC, Douglas HO. Management of cystic neoplasms of the pancreas. Am. Surg. 2000; 66:495-501.
- Panieri E, Krige JE, Bornman PC, Graham SM, Terblanche J, Cruse JP. Operative management of papillary cystic neoplasms of the pancreas. J. Am. Coll. Surg. 1998; 186:319-324. [PMID: 9510263]
- Brugge WR, Lauwers GY, Sahani D, Fernandez-del Castillo C, Warshaw AL. Cystic neoplasms of the pancreas. N. Engl. J. Med. 2004; 351:1218-1226.
- Azzopardi N. Cystic lesions of the pancreas. Malta Med. J. 2014; 26(02): 58-62.
- Jani N, Hani MB, Schulick RD, Hruban RH, Cunningham SC. Diagnosis and management of cystic lesions of the pancreas. Diagn. Ther. Endosc. 2011.
- Balik AA, Celebi F, Basglu M, Oren D, Yildirgan I, Atamanalp SS. Intraabdominalextrahepaticechinococcosis. Surg. Today 2001; 31:881-884.
- Chammakhi-Jemli C, Mekaouer S, Miaoui A, Daghfous A, Mzabi H, Cherif A, et al. Hydatid cyst of the pancreas presenting with acute pancreatitis. J. Radiol. 2010; 91:797-799. [PMIC ID: 20814363] [64]
- Pedrosa I, Saíz A, Arrazola J, Ferreirós J, Pedrosa CS. Hydatid disease: radiologic and pathologic features and complications. Radiographics 2000; 20:795-817. [PMID: 10835129]
- Ilica AT, Kocaoglu M, Zeybek N, GuvenS, AdaletliI, BasgulA. Exrahepatic abdominal hydatid disease caused by Echinococcusgranulosus: imaging findings. AJR Am. J. Roentgenol. 2007; 189:337-343.
- Missas S, Gouliamos A, Kourias E, Kalovidouris A. Primary hydatid disease of the pancreas. Gastrointest. Radiol. 1987; 12:37-38.
- Puli SR, Kalva N, Bechtold ML, Pamulaparthy SR, Cashman MD, Estes NC, et al. Diagnostic accuracy of endoscopic ultrasound in pancreatic neuroendocrine tumors: A systematic review and meta analysis. World. J. Gastroenterol.2013; 19(23): 3678-3684. PMID: 23801872]
- Dancygier H, Lightdale CJ, Stevens PD. Endoscopic ultrasonography of the upper gastrointestinal tract and colon. In: Dancygier H, Lightdale CJ, editors. Endosonography in gastroenterology. Principles, techniques, findings. Stuttgart: Thieme, 1999:13-22.
- Klapman JB, Chang KJ, Lee JG, Nguyen P. Negative predictive value of endoscopic ultrasound in a large series of patients with a clinical suspicion of pancreatic cancer. Am. J. Gastroenterol. 2005; 100:2658-2661. [PMID: 16393216]
- Owens DJ, Savides TJ. Endoscopic ultrasound staging and novel therapeutics for pancreatic cancer. Surg. Oncol. Clin. N. Am. 2010; 19: 255-266. [PMID: 20159514]
- Barresi L, Tarantino I, Granata A, Curcio G, Traina M. Pancreatic cystic lesions: How endoscopic ultrasound morphology and endoscopic ultrasound fine needle aspiration help unlock the diagnostic puzzle. World J. Gastrointest. Endosc. 2012; 4(6): 247-259. [PMC ID: 3377868]
- Michl P, Pauls S, Gress TM. Evidence-based diagnosis and staging of pancreatic cancer. Best. Pract. Res. Clin. Gastroenterol. 2006; 20:227-251. [PMID: 16549326]
- Diop SP, Costi R, Le Bian A, Carloni A, Meduri B, Smadja C. Acute pancreatitis associated with a pancreatic hydatid cyst: understanding the mechanism by EUS. Gastrointest. Endosc. 2010; 72: 1312-1314.
- ASGE guideline: the role of endoscopy in the diagnosis and the management of cystic lesions and inflammatory fluid collections of the pancreas. Gastrointest. Endosc. 2005; 61(3):363-370. [PMID: 15758904]
- Chang KJ. Endoscopic ultrasound-guided fine needle aspiration in the diagnosis and staging of pancreatic tumors. Gastrointest. Endosc. Clinics North Amer. 1995;5:723-34. [PMID: 19803666]
- Bhutani MS. Endoscopic ultrasonography in pancreatic disease. Seminars in Gastrointestinal Disease 1998;9:51-60.
- Bhutani MS, Hawes RH, Baron PL, Sanders-Cliette A, van Velse A, Osborne JF, et al. Endoscopic ultrasound guided fine needle aspiration of malignant pancreatic lesions. Endoscopy 1997;29:854-58. [PMID: 9476770]
- Erickson RA, Sayage-Rabie L, Beisner RS. Factors impacting endoscopic ultrasound-guided fine needle aspiration passes for pancreatic malignancies. Gastrointest. Endosc. 2000;51:184-90.
- Chang KJ, Katz KD, Durbin TE, Erickson RA, Butler JA, Lin F, et al. Endoscopic ultrasound guided fine needle aspiration. Gastrointest. Endosc. 1994;40:694-9.
- Ylagan LR, Edmundowicz S, Kasal K, Walsh D, Lu DW. Endoscopic ultrasound guided fine-needle aspiration cytology of pancreatic carcinoma: a 3-year experience and review of the literature. Cancer 2002;96:362-9. [PMID: 12478684]
- Chang KJ, Albers CG, Erickson RA, Butler JA, Wuerker RB, Lin F. Endoscopic ultrasound guided fine needle aspiration of pancreatic carcinoma. Am. J. Gastroenterol. 1994;89:263-6. [PMID: 22632941]
- Erickson RA, Sayage-Rabie L, Beisner RS. Factors impacting endoscopic ultrasound-guided fine needle aspiration passes for pancreatic malignancies. Gastrointest. Endosc. 2000;51:184-90. [PMC4063260]
- Erickson RA, Sayage-Rabie L, Avots-Avotins A. Clinical utility of endoscopic ultrasound-guided fine needle aspiration. Acta. Cytol. 1997;41:1647-53. [PMID: 0009165320]
- David O, Green L, Reddy V, KluskensL, Bitterman P, Attal H, et al. Pancreatic masses: a multi-institutional study of 364 fine-needle aspiration biopsies with histopathologic correlation. Diagn. Cytopathol. 1998;19:423-7.
- Erickson RA. Endoscopic ultrasound guided fine needle aspiration of the pancreas. VHJOE 2002;1(3).
- Erickson RA. Technical review: EUS-guided fine needle aspiration. Gastrointest. Endosc. 2004:50:267-79.
- Kliment M, Urban O, Cegan M, Fojtik P, Falt P, Dvorackova J, et al. Endoscopic ultrasound-guided fine needle aspiration of pancreatic masses: The utility and impact on management of patients. Scand. J. Gastroenterol. 2010; 45;1372-1379. [PMID: 20626304]
- Fritscher-Ravens A, Brand L, Knofel WT, Bobrowski C, Topalidis T, Thonke F, et al. Comparison of endoscopic ultrasound-guided fine needle aspiration for focal pancreatic lesions in patients with normal parenchyma and chronic pancreatitis. Am. J. Gastroenterol. 2002; 97; 2768-2775. [PMID: 12425546]
- Boujaoude, J. Role of endoscopic ultrasound in diagnosis and therapy of pancreatic adenocarcinoma. World J. Gastroenterol. 2007; 13:3662-3666. [PMC4250635]
- Aithal GP, Chen RYM, Cunningham JT, Durkalski V, Kim EY, Patel RS, et al. Accuracy of EUS for detection of intraductal papillary mucinous tumor of the pancreas. Gastrointest. Endosc. 2002; 56:701-7. [PMID: 12397279]
- Brandwein S, Farrell JJ, Centeno BA, Brugge WR. Detection and tumor staging of malignancy in cystic, intraductal, and solid tumor of the pancreas by EUS. Gastrointest. Endosc. 2001; 53:722-7. [PMID: 11375578]
- Frossard JL, Amouyal P, Amouyal G, Palazzo L, Amaris J, Soldan M, et al. Performance of endosonography-guided fine needle aspiration and biopsy in the diagnosis of pancreatic cystic lesions. Am. J. Gastroenterol. 2003; 98:1516-24. [PMID: 12873573]
- Lai R, Stanley MW, Bardales R, Linzie B, Mallery S. Endoscopic ultrasound-guided pancreatic duct aspiration: diagnostic yield and safety. Endoscopy 2002; 34:715-20. [PMID: 12195329]
- Williams DB, Sahai AV, Aabakken L, Penman ID, van Velse A, Webb J, et al. Endoscopic ultrasound guided fine needle aspiration biopsy: a large single centre experience. Gut. 1999;44:720-6. [PMID: 10205212]
- Eloubeidi MA, Tamhane A, Varadarajulu S, Wilcox C.M. Frequency of major complications after EUS-guided FNA of solid pancreatic masses: A prospective evaluation. Gastrointest. Endosc. 2006; 63:622-629. [PMID: 16564863]
- O’Toole D, Palazzo L, Arotcarena R, Dancour A, Aubert A, Hammel P, et al. Assessment of complications of EUS-guided fine-needle aspiration. Gastrointest. Endosc. 2001; 53:470-4. [PMID: 11275888]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno BA, Szydlo T, Regan S, et al. The diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst (CPC) study. Gastroenterology 2004; 126:1330-6. [PMID: 15131794]
- Anderson MA, Fisher L, Jain R, Evans JA, Appalaneni V, Ben-Menachem T, et al. Complications of ERCP. Gastrointest. Endosc. 2012; 75(3):467-473.
- Rizk MK, Gerke H. Utility of endoscopic ultrasound in pancreatitis: A review. World J. Gastroenterol. 2007; 13(47): 6321-6326. [PMC4205449]
- Kattan YB. Hydatid cysts in pancreas. BMJ 1975; 729-730. [PMC1675546]
- Sinha AN, Rao ASN, Vyas HG. Hydatid cyst in head of pancreas presenting with obstructive jaundice. Idian J Gastroenterol 1997; 16:33. [PMID: 9167380]
- Astiz JM, Astiz FL, Buzzi AB. Primary hydatid cyst mistaken for carcinoma of the pancreas. J. R. Soc. Med. 1997; 90:334. [PMID: 9227383]
- Bolognese A, Barbarosos A, Muttillo IA, Valabrega S, Bocchetti T. Echinococcus cyst of the pancreas: description of a case and review of the literature. G. Chir. 2000;21(10):389-93. [PMID: 11126737]
- Hewes JC, Milsom A, Purkiss SF. Hydatid Disease Presenting as Pancreatitis. 2000; 1:7-10.
- Colovic R, Grubov N, Radak V, Colovic N, Stojkovic M. Hydatid cyst of the pancreas. Srp. Arh. Celok. Lek. 2004; 132(11-12):435-437.
- Echenique-Elizondo M, Arratíbel JAA. Hydatid Disease of the Pancreas. J. Pancreas 2004; 5(1):51-52. [PMID: 14730124]
- Erkan N, Haciyanli M, Yildirim M, Yilmaz C. A Case report of the unusual presence of hydatid disease in the pancreas and breast. J Pancreas 2004; 5(5):368-372. [PMID: 15365205]
- Ozmen MM, Moran M, Karakahya M, Coskun F. Recurrent Acute Pancreatitis Due to a Hydatid Cyst of the Pancreatic Head: A Case Report and Review of the Literature. J Pancreas 2005; 6(4):354-358. [PMID:16006687]
- Wani RA, Malik AA, Chowdri NA, Wani KA, Naqash SH. Primary extrahepatic abdominal hydatidosis. Int. J. Surg. 2005; 3:125-127. [PMID: 17462273]
- Bayat MRH, Mahomedy S, Misser SK, Corr P. Pancreatic hydatid cyst mimicking a choledochal cyst. SA. J. Radiology 2005; 34-35.
- Zeybek N, TAS H, KA Ymakcioglu N, Ozcan A, Cetiner S, Tufan T. Hydatid cyst in the head of the pancreas in an adult: case report. Kocatepe Med J 2006; 7: 9-121.
- Jai SR, El Hattabi K, Bensardi F, Chehab F, Khaiz D, Bouzidi A. Primary hydatid cyst of the pancreas causing obstructive jaundice. Saudi. J. Gastroenterol. 2007; 13(4): 191-193. [PMID: 19858645]
- Abu-AlHail MC. Pancereatichydatid as a cause of epigastric mass, a case report. Bas. J. Surg. 2008; 14.
- Borisa AD, Bakhshi GD, Tayade MB, Pawar NH, Nikam NN, Pathrikar S. Hydatid cyst of pancreas. Bombay Hosp. J. 2009; 51(1):88-90.
- Heis HA, Bani-Hani KE, Elheis MA. Primary hydatid cyst of the pancreas. Acta. Chir. Belg. 2009;109(5):626-8. [PMID: 19994808]
- Zaidi SH. Some rare presentations of hydatid cysts: two case reports. Cases J. 2009; 2:62. [PMID: 19149905]
- Masoodi I, Nabi G, Kumar R, Lone MA, Khan BA, Al Sayari KN. Hydatid cyst of the pancreas: A case report and brief review. Turk. J. Gastroenterol. 2011; 22 (4):430-432. [PMID: 21948577]
- Kumar Bansal V, Misra M, Karishna A, Kumar S, Garg P, khan R, et al. Pancreatic hydatid cyst masquerading as cystic neoplasm of pancreas. Trop. Gastroenterol. 2010; 31(4):335–337. [PMID: 21568157]
- Shah OJ, Robbani I, Zargar SA, Yattoo GN, Shah P, Ali S. Hydatid cyst of the pancreas. an experience with six cases. J Pancreas 2010; 11(6):575-581. [PMID: 21068489]Suryawanshi P, Khan AQ, Jatal S. Primary hydatid cyst of pancreas with acute pancreatitis. Int J Surg Case Rep 2011; 2:122-124. [PMID: 22096702]
- Cankorkmaz L, Gumus C, Celiksoz A, Koyluoglu G. Primary hydatid disease of the pancreas mimicking pseudo-cyst in a child: case report and review of the literature. TurkiyeParazitolDerg 2011; 35:50-2. [PMID: 21618194]
- Bhat NA, Rashid KA, Wani I, Wani S, Syeed A.Hydatid cyst of the pancreas mimicking choledochal cyst. Ann Saudi Med 2011; 31: 536–538. [PMID: 21911995]
- Dalal U, Dalal AK, Singal R, Naredi B, Gupta S. Primary hydatid cyst masquerading as pseudocyst of the pancreas with concomitant small gut obstructiondan unusual presentation. Kaohsiung J MedSci 2011; 27:32-35. [PMID: 21329890]
- Agrawal S, Parag P. Hydatid cyst of head of pancreas mimicking choledochal cyst. BMJ Case Reports 2011. [PMID: 22693192]
- Rayate A, Prabhu R, Kantharia C, Supe A. Isolated pancreatic hydatid cyst: Preoperative prediction on contrast-enhanced computed tomography case report and review of literature. Med J 2012; 5:66-68.
- Karaman B, Battal B, Ustunsoz B, SahinUgurel M. Percutaneous Treatment of a Primary Pancreatic Hydatid Cyst Using a Catheterization Technique. Korean J Radiol 2012; 13:232-236. [PMID: 22438691]
- Mandelia A, Wahal A, Solanki S, Srinivas M, Bhatnagar V. Pancreatic hydatid cyst masquerading as a choledochal cyst.JPediatrSurg 2012; 47:e41-4. [PMID: 23164030]
- Baghbanian M, Salmanroghani H, Karegar S, Binesh F, Baghbanian A. Pancreatic tail hydatid cyst as a rare cause for severe acute pancreatitis: a case report. Govaresh 2013;18:194-198.
- Turkyilmaz Z, Kapisiz A, Sonmez K, Karabulut R, Basaklar AC. Obstructive jaundice resulted from hydatid cyst of pancreatic head. Hippokratia 2013; 17:378-379. [PMID: 25031523]
- Patil DS, Jadhav KV, Ahire PP, Patil SR, Shaikh TA, Bakhshi GD. Pancreatic hydatid presenting as an intercostal hernia. Int J Med Sci 2013; 2:255-258.
- Gedam BS, Wilkinson TRV, Akulwar VV. Pancreatic hydatid cyst managed successfully by internal drainage. J case Rep 2013; 3:358-361.
- Kaushik K, Garg P, Aggarwal S, Narang A, Verma S, Singh J, et al. Isolated pancreatic tail hydatid cyst - is distal pancretectomy always required?Int JGastroenterol 2013;13.
- Yarlagadda P, Yenigalla BM, Penmethsa U, Myneni RB. Primary pancreatic echinococcosis. Trop Parasitol 2013; 3:151–154. [PMID: 24471002]
- Chatterjee S, Roy MK, Banerjee S, Mukhopadhaya S, Sen S, Mallath M. Hydatid cyst imicking cystic neoplasm of the pancreatic tail: an endoscopic ultrasound diagnosis. Endoscopy 2014; 46: E318–E319. [PMID: 25058831]
- Parashari U, Khanduri S, Agrawal D, Bhadury S, Singh N. An unusual case of primary pancreatic hydatidosis with review of literature. Trop J Med Res 2014; 17:127-129.
- Khoshmohabat H, AkhavanMoqadam J, Sohrabi SZ, KalantarMotamedi MH, Azizi T. Hydatid cyst of the pancreas mimicking neoplasm. JColl PhysiciansSurg Pak 2014; 24:S84-S85. [PMID: 24906281]
- Unal B, Elpek GO, Yildirim S, Gelen T, Erdogan O, Ozkaynak C. Echinococcusmultilocularis infestation in the head of the pancreas. J ClinExpPathol 2014; 4:3.

