Keywords
Cholangiopancreatography, Endoscopic Retrograde; Choledochal Cyst; Congenital Abnormalities; Pancreatitis
Abbreviations
APBJ: anomalous pancreaticobiliary junction; ERCP: endoscopic retrograde cholangiopancreatography
INTRODUCTION
Anomalous pancreaticobiliary junction (APBJ) is a rare malformation in which the pancreatic duct and bile duct join outside the duodenal wall with a common channel which is longer than 15 mm [1, 2]. Komi [3] has proposed a new classification of APBJ, dividing it into three major types, and presently, this is the most accepted classification. In type I, the common bile duct joins the pancreatic duct at a right angle; in type II, the pancreatic duct joins the common bile duct at an acute angle. Both of these types are subdivided into subtypes “a” or “b”, according to whether the common channel is dilated or not. The normal caliber of the common channel is 3-5 mm. In type III, APBJ union is complicated with a patent accessory pancreatic duct with or without an intricate network of ducts, and is sub classified into types IIIa, IIIb, and IIIc (which is equivalent to Warshaw’s type pancreas divisum with biliary dilatation) [3]. Most cases of APBJ are reported from Asian countries, predominantly from Japan [4, 5, 6]. There are only a few studies on APBJ from India [2, 7, 8] but none of them specifically highlight the prevalence of APBJ, in particular the new Komi type III APBJ. We are among the largest gastroenterology referral centres of the country and have retrospectively analyzed our ERCP data obtained between 1985 and 2005, encountering only two cases of type III APBJ. We report these cases with their ERCP findings. This paper also highlights the rarity of type III APBJ in Indian patients with pancreatico-biliary disorders.
MATERIAL AND METHODS
Patients
Retrospective analysis of all ERCP examinations carried out between 1985 and 2005 in our department for various pancreaticobiliary disorders was performed and cases of APBJ were identified and analyzed.
Techniques
All the ERCP examinations were carried out using Olympus sideviewing endoscopes (Olympus Corporation, Tokyo, Japan). Water soluble iodinated contrast was used for opacification of the pancreatic and bile ducts. Three to six spot films were taken for each patient.
Image Analysis
The inclusion criteria were adequate filling of the common bile duct and main pancreatic duct on ERCP, and distinct visualization of the opening of the two ducts separately or by a common channel into the duodenum. All ERCP films were reviewed by a gastrointestinal radiologist. The diagnosis of APBJ was made if the length of the common channel exceeded 15 mm with or without dilation (>5 mm). APBJ was classified according to the new Komi classification [3] and the prevalence of various types was calculated.
ETHICS
Written consent was obtained from each patient who underwent ERCP. The patients were treated according to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004
STATISTICS
All cases of ERCP fulfilling the inclusion criteria, and where the APBJ was clearly discernable were included for analysis. The percentage of patients demonstrating APBJ was calculated and classified according to the new Komi classification [3]. The percentage of the various types of APBJ was calculated for the purpose of estimating the prevalence of type III APBJ.
RESULTS
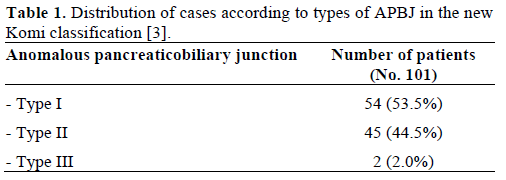
A review of the ERCP records of 3,827 patients yielded a total of 101 patients (2.63%) having APBJ. Of the 101 patients with APBJ, there were 48 males and 53 females, ranging from 3 to 85 years of age. The distribution of the types of APBJ is shown in Table 1.Only 2 patients (2.0% of all APBJ cases and 0.05% of all ERCP examinations) had type III APBJ. The relevant clinical details with detailed ERCP findings of the patients having type III APBJ are herein described.
Case 1
A 31-year-old man presented having experienced recurrent pain restricted to the upper right quadrant for the past 10 years. He had had six episodes, one every 6-12 months, each lasting 7 to 10 days. He denied having fever or jaundice during the episodes of pain, He had never been examined before presenting at our centre. He had had a similar episode of pain for a week before presenting to our centre. On examination, there was no pallor, icterus or lymphadenopathy. There was no hepatosplenomegaly or lumps in the abdomen. Investigations showed hemoglobin of 11.5 g/dL (reference range: 11-14 g/dL), bilirubin of 0.4 g/dL (reference range: 0-1 g/dL), SGOT of 15 IU/L (reference range: 2-40 IU/L), SGPT of 20 IU/L (reference range: 2-41 IU/L) and alkaline phosphatase of 8 IU/L (reference range: 40-129 IU/L). An ultrasound was carried out which revealed a dilated common bile duct. ERCP through the major papilla with contrast injection demonstrated a ventral duct small in caliber with a long common channel (19 mm in length and 2 mm in diameter). The common bile duct and its intrahepatic right and left branches were also dilated which was diagnostic for a type IVb choledochal cyst (Figure 1). There was no communication with the dorsal duct consistent with complete pancreas divisum. The dorsal duct was the dominant duct with a calculus and prominent side branches consistent with the Cambridge type III changes for chronic pancreatitis. The overall features were consistent with APBJ type IIIa and a cyst excision with hepatico-jejunostomy was carried out. The patient has been regularly followed up for the last 18 years without any new complaints.
Figure 1. ERCP image into the major papilla using a contrast
injection shows a long common channel (thin arrows), ventral duct
(arrow heads) and a type IVb choledochal cyst (*). Note the calculi
in the dorsal duct (thick arrows).
Case 2
A 22-year-old female presented having experienced recurrent episodes of pain in the upper abdomen, radiating to the back, for the past 2 months. She had had multiple episodes of similar pain for the past 3 years. Serum amylase was at borderline levels (96 U/L; reference range: 20-100 U/L), SGOT was 30 IU/L, SGPT was 36 IU/L and alkaline phosphatase was elevated (183 IU/L). MRCP revealed dilated main pancreatic and common bile ducts without any dilation of the intrahepatic biliary channels. ERCP demonstrated complete pancreas divisum with the dorsal duct as the dominant duct. There was a long common channel (24 mm in length and 4 mm in diameter) with the ventral duct. The common bile duct was fusiformly dilated without dilation of the intrahepatic biliary ducts consistent with a type Ic choledochal cyst (Figure 2a). The dorsal duct and its side branches were dilated, consistent with Cambridge type III changes for chronic pancreatitis (Figure 2b). The overall morphology was consistent with APBJ type IIIa. A 5-F plastic pancreatic stent was placed in the dominant duct. The patient is being followed up and surgery is planned.
Figure 2. a. ERCP image shows a long common channel (thin
arrows) with the ventral duct (thick arrow) and a type Ic choledochal
cyst. b. ERCP image shows a dominant dorsal duct with changes of
chronic pancreatitis (arrows). Note a choledochal cyst in the
background (*).
DISCUSSION
APBJ is a congenital anomaly in which the main pancreatic and common bile ducts join outside the duodenal wall with a long common channel of more than 15 mm [1, 2]. Choledochal cysts are congenital cystic dilatations of the extrahepatic or intrahepatic bile ducts or both, and have been classified into five types by Todani et al. [9]. According to this classification, type I is a solitary fusiform extrahepatic cyst (further subclassified according to the shape of the affected segment into three types. Type Ia involves cystic dilatation of the common bile duct, type Ib involves focal, segmental dilatation of the common bile duct, and type Ic involves fusiform dilatation of the common bile duct, along with diffuse, cylindric dilatation of the common hepatic duct and common bile duct); type II is an extrahepatic supraduodenal diverticulum; type III is a choledochocele; type IVa are fusiform extra- and intrahepatic cysts; type IVb are multiple extrahepatic cysts, and type V are multiple intrahepatic cysts or Caroli's disease [9].
The association of APBJ with a choledochal cyst may be present in up to 90% of cases [8, 10, 11]. Various causative factors have been postulated for the association of choledochal cysts with APBJ, such as a congenital weakness of the common bile duct and reflux of the pancreatic juices into the bile duct because of high pressure in the pancreatic duct [12, 13]. Hence, this association is more than a chance finding and, once diagnosed, such patients should undergo a definitive surgical procedure to prevent potential complications, such as biliary strictures, cholangitis, and carcinoma of biliary tract, gall bladder and pancreas [1, 2, 7, 8, 14, 15].
Most of the cases of APBJ have been reported from Asian countries, predominantly from Japan [4, 5, 6]. Misra et al. and Nagi et al. from India have described APBJ and related disorders [2, 7, 8], but the prevalence of the various types of APBJ has never been reported from anywhere outside Japan. In their series, Komi et al. from Japan reported type I APBJ in 35.3%, type II in 21.6% and type III in 43.1% of cases [4]. Similar results were reported by Li et al. from Japan where the prevalence of type III APBJ was 41.5% [6].
The present study revealed only 2 cases of type III APBJ; i.e., 2.0% of all APBJ cases and 0.05% of all the ERCP examinations performed over two decades in our institution, a referral centre of North India. This analysis highlights the low prevalence of type III APBJ in symptomatic Indian patients with pancreaticobiliary disorders
Both of our cases showed the clinical and radiological features of chronic pancreatitis, choledochal cysts, long common channel and complete pancreas divisum consistent with the new Komi type IIIa APBJ. The chronic pancreatitis seen in our patients can be attributed to pancreas divisum and APBJ as both of these conditions are known to be associated with an obstructed flow of pancreatic secretions [4, 7, 16, 17]. Pancreatic duct calculi are only rarely encountered in APBJ and choledochal cysts [18, 19], and these are seen predominantly in adults [12]. However, subtype IIIc3 APBJ has been reported to be associated with ductal calculi in up to 43.8% of cases [4]. The proposed pathogenesis of pancreatic ductal calculi is protein plug formation and mucin overproduction [4, 20]. Whether the presence of pancreatic calculi makes a patient with APBJ symptomatic or not is controversial as only a few reports suggest that their presence results in symptoms [13, 20].
The classification of APBJ is important for management as types Ib, IIb, IIIc3 are associated with a dilated common channel (greater than 5 mm) and are frequently complicated by chronic relapsing pancreatitis due to the formation of a protein plug or pancreatic calculi [4]. For type IIIc3, a pyloruspreserving pancreatoduodenectomy is the surgical procedure of choice while, for type Ib and type IIb, a papilloplasty can be carried out if stenosis of the papilla is present [4]. For choledochal cysts, cyst excision with bilioenteric anastomosis should be carried out [9, 13, 21].
In conclusion, in this first report outside Japan, the prevalence of type III APBJ was only 2.0%. We encountered two such cases over two decades in a referral hospital of Northern India. A multicentric study to explore the incidence of APBJ in the general population using non-invasive radiological investigations, such as ultrasound, multidetector computed tomography or magnetic resonance cholangiopancreatography should be carried out to get a better perspective of APBJ and related disorders
Conflict of interest
The authors have no potential conflict of interest
References
- Kimura K, Ohto M, Saisho H, Unozawa T, Tsuchiya Y, Morita M, et al. Association of gall bladder carcinoma and anomalous pancreaticobiliary duct union. Gastroenterology 1985; 89:1258-65. [PMID 4054518]
- Misra SP, Gulati P, Thorat VK, Vij JC, Anand BS. Pancreaticobiliary ductal union in biliary diseases. An endoscopic retrograde cholangiopancreatographic study. Gastroenterology 1989; 96:907-12. [PMID 2914651]
- Komi N. New classification of anomalous arrangement of the pancreaticobiliary duct (APBD) in the choledochal cyst; a proposal of new Komi's classification of APBD. J Jpn Pancr Soc 1991; 6: 234- 43.
- Komi N, Takehara H, Kunitomo K, Miyoshi Y, Yagi T. Does the type of anomalous arrangement of pancreaticobiliary ducts influence the surgery and prognosis of choledochal cyst? J Pediatr Surg 1992; 27:728-31. [PMID 1306647]
- Yokohata K, Kimura H, Naritomi G, Konomi H, Takeda T, Ogawa Y, Tanaka M. Type classification of anomalous pancreaticobiliary junction by ERCP J Hepatobiliary Pancreat Surg 1994; 1:236-9.
- Li L, Yamataka A, Wang YX, Wang DY, Wang K, Li ZX, et al. Anomalous pancreatic duct anatomy, ectopic distal location of the papilla of Vater and congenital biliary dilatation: a new developmental triad? Pediatr Surg Int 2003; 19:180-5. [PMID 12698266]
- Misra SP, Dwivedi M. Pancreaticobiliary ductal union. Gut 1990; 31:1144-9. [PMID 2083859]
- Nagi B, Kochhar R, Bhasin D, Singh K. Endoscopic retrograde cholangiopancreatography in the evaluation of anomalous junction of the pancreaticobiliary duct and related disorders. Abdom Imaging 2003; 28:847-52. [PMID 14753604]
- Todani T, Watanabe Y, Narusue M, Tabuchi K, Okajima K. Congenital bile duct cysts: Classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst. Am J Surg 1977; 134:263-9. [PMID 889044]
- Komi N, Kashiwagi Y, Ikeda N. The etiology of congenital dilatation of the biliary duct. Jpn J Pediatr Surg 1977; 1101-9.
- Kimura K. Studies in 28 cases of congenital cystic dilatation of the common bile duct in the adults. Roentgenological features and a union between the choledochus and the main pancreatic duct. Jpn J Gastroenterol 1976; 73: 61-74.
- Babbitt DP, Starshak RJ, Clemett AR. Choledochal cyst: a concept of etiology. Am J Roentgenol Radium Ther Nucl Med 1973; 119:57-62. [PMID 4744730]
- Chaudhary A, Dhar P, Sachdev A, Kumar N, Vij JC, Sarin SK, et al. Choledochal cysts--differences in children and adults. Br J Surg 1996; 83:186-8. [PMID 8689160]
- Roukounakis NE, Kuhn JA, McCarty TM. Association of an abnormal pancreaticobiliary junction with biliary tract cancers. Proc (Bayl Univ Med Cent) 2000; 13:11-3. [PMID 16389319]
- Kuga H, Yamaguchi K, Shimizu S, Yokohata K, Chijiiwa K, Tanaka M. Carcinoma of the pancreas associated with anomalous junction of pancreaticobiliary tracts: report of two cases and review of the literature. J Hepatobiliary Pancreat Surg 1998; 5:113-6. [PMID 9683764]
- Chowdhury A, Chatterjee BK, Dutta P, Roy J, Chowdhury T, Das K, Goenka MK. Pancreas divisum with chronic calcific pancreatitis: cause or coincidence. Trop Gastroenterol 1997; 18:172- 3. [PMID 9612101]
- Dhar A, Goenka MK, Kochhar R, Nagi B, Bhasin DK, Singh K. Pancrease divisum: five years' experience in a teaching hospital. Indian J Gastroenterol 1996; 15:7-9. [PMID 8840617]
- Yamaguchi M. Congenital choledochal cyst. Analysis of 1,433 patients in the Japanese literature. Am J Surg 1980: 140:653-7. [PMID 6776832]
- Taneja S, Nagi B, Kochhar R, Bhasin DK, Lal A, Singh K. Intraductal pancreatic calculi in patients with choledochal cyst. Australas Radiol 2004; 48:302-5. [PMID 15344977]
- Kaneko K, Ando H, Ito T, Watanabe Y, Seo T, Harada T, Ito F. Protein plugs cause symptoms in patients with choledochal cysts. Am J Gastroenterol 1997; 92:1018-21. [PMID 9177522]
- Hata Y, Sasaki F, Takahashi H, Tamura M, Ohkawa Y, Saji Y, et al. Surgical treatment of congenital biliary dilatation associated with pancreaticobiliary maljunction. Surg Gynecol Obstet 1993; 176: 581-7. [PMID 8322133]



