Keywords
Lymph Nodes; Pancreatic Neoplasms; C-Reactive Protein
INTRODUCTION
Pancreatic ductal adenocarcinoma is the second most common cause of death from cancer of all gastrointestinal malignancies [1]. The 5-year survival rates are poor and remain unchanged over the last 25 years [2, 3]. Surgical resection remains the mainstay of treatment with 5-year post-curative resection survival rates between 7-25% [3]. Several pathological predictors have been identified that predict survival following resection, and include vascular and perineural invasion, tumour grade, tumour size and resection margin status [4, 5]. Nevertheless, the majority of these histological predictors are only amenable for assessment after surgery. More recently, several studies have independently identified potential prognostic indices predicting survival preoperatively, including serum C-reactive protein (CRP) levels [6, 7] lymphocyte count [8], platelet/lymphocyte ratio [9] and neutrophil/lymphocyte ratio [10] in patients with pancreatic ductal adenocarcinoma whilst some studies did not show any potential benefit [11]. This study has investigated the prognostic role of the pre-operative inflammatory response including platelet count, lymphocyte count, neutrophil/lymphocyte ratio, platelet/lymphocyte ratio and serum CRP levels on survival after curative resection for pancreatic ductal adenocarcinoma. In addition this study has evaluated the prognostic importance of lymph node status and lymph node ratio on post-operative patient survival, as these factors may help tailor neo-adjuvant and adjuvant therapies for high risk patient cohorts in pancreatic cancer.
METHODS
Patients
Ninety-one patients who underwent pancreaticoduodenectomy (PD) with a curative intent between 2002 and 2008 were identified from the prospectively maintained database at Ninewells Hospital, Dundee, United Kingdom. Patients with preoperative ERCP were specifically excluded from the study to exclude patients with raised CRP levels secondary to biliary instrumentation. Fifty-one patients with histologically confirmed pancreatic ductal adenocarcinoma were included in the analysis whilst other pathologies such as periampullary carcinomas, cystic neoplasms of the pancreas and neuroendocrine tumours were excluded. Two patients with cholangitis had surgery deferred for 6 weeks to allow normalisation of acute inflammatory response prior to surgery.
Data Collection
Data collected included patient demographics, surgical details, and standard histological tumour characteristics. Preoperative blood counts and serum CRP levels were obtained for all patients one day before surgery. The impact of preoperative inflamematory markers including serum CRP level, white cell count, neutrophil count, platelet count, neutrophil/ lymphocyte ratio, preoperative lymphocyte count and platelet/lymphocyte ratio on survival was assessed. Hospital computer and radiology records were reviewed to identify dates of death to calculate survival. In addition the impact of tumour characteristics such as tumour size (less than, or equal to, 2 cm vs. more than 2 cm), lymph node status, lymph node ratio, perineural invasion, resection margin status (positive/negative), and development of post-operative pancreatic fistula on survival was assessed. Pancreatic fistula was defined according to the International Study Group on Pancreatic Fistula [12] Drain fluid was routinely tested for amylase on postoperative days 5, 10, 15 and every 5 days thereafter if appropriate.
ETHICS
The secure prospective database was created after approval from the University of Dundee. The written informed consent was obtained for all investigations made according to the usual clinical practice. The study protocol was approved by the institutional review committee. The study protocol conforms to the ethical guidelines of the World Medical Association Declaration of Helsinki.
STATISTICS
Statistical analysis was performed using SPSS software version 17 (SPSS, Chicago, IL, USA). Continuous data were described using median and range. The Fisher’s exact tests were used to analyse categorical data. Kaplan-Meier curves were generated to illustrate survival trends. Univariate and stepwise multivariate Cox proportional hazards models were applied in order to identify the significance overall survival and hazard ratios (HRs) and 95% confidence intervals (CIs) were also computed. A two-tailed P value less than 0.05 was considered statistically significant.
RESULTS
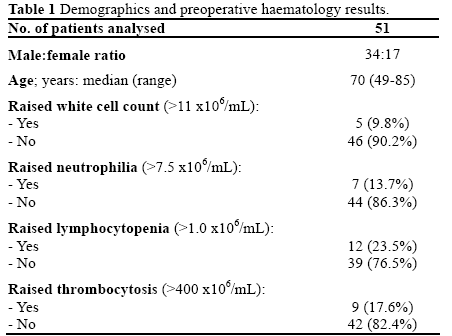
Ninety-one patients underwent pancreaticoduodenectomy during the study period, of which 51 patients (56.0%) had histologically confirmed pancreatic ductal adenocarcinoma. The median age of the study group was 70 years (range: 49-85 years). The male to female ratio was 2:1. Demographic and haematological data are shown in Table 1. The median overall survival was 13 months (range: 2.5-70 months).
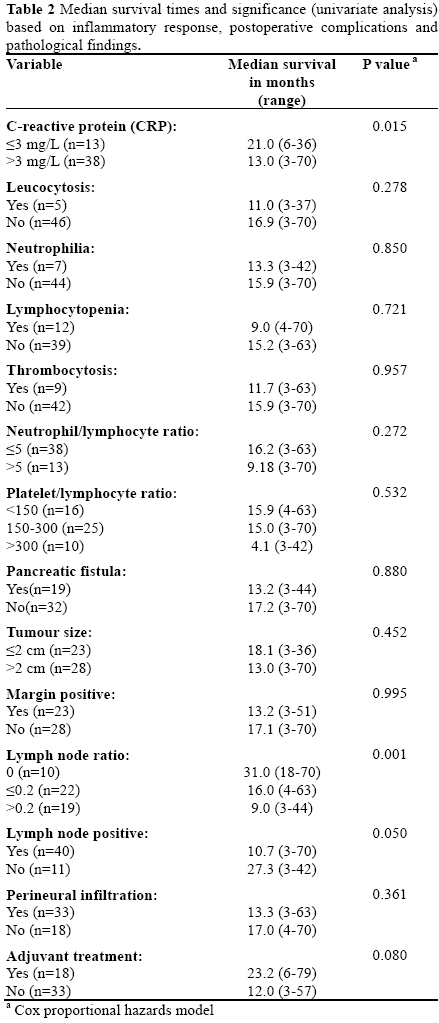
The results of univariate analysis of patient survival for each of the hematologic parameters of the inflammatory response, postoperative complications and pathological findings are shown in Table 2. An elevated preoperative serum CRP level greater than 3 mg/L was found to be a significant adverse prognostic factor (P=0.015) predicting a poor survival, whereas white cell count (P=0.278), neutrophil count (P=0.850), neutrophil/lymphocyte ratio (P=0.272), platelet/ lymphocyte ratio (P=0.532) and lymphocyte count (P=0.721) were not significant prognosticators at univariate analysis. Presence of metastatic lymph nodes (P=0.050), resection margin positivity (P=0.995), and peri-neural invasion (P=0.361) did not adversely affect survival at univariate analysis. However, raised lymph node ratio did predict poor survival at univariate analysis (P<0.001). The median number of lymph nodes harvested for the study group were 20 (range: 0- 41). Eleven (21.6%) of 51 patients had negative peripancreatic lymph nodes. The median survival was 27.3 months in lymph node negative (N0) patients and 10.7 months in those with lymph node positive disease (N1) (P=0.050). Nineteen (50.0%) out of the 38 patients with elevated CRP preoperatively had margin positivity compared to 4 out 13 (30.8%) patients with normal CRP. Elevated CRP preoperatively was not associated with an increased rate of margin positivity in resected specimens (P=0.336; Fisher’s exact test).
Kaplan-Meier cumulative survival curves for patients stratified into two groups according to serum CRP level less than, or equal to, 3 mg/L and greater than 3 mg/L are shown in Figure 1. Patients with a pre-operative serum CRP level greater than 3 mg/L had a significantly poorer median survival (13.0 months) when compared to patients with a serum pre-operative CRP level less than, or equal to, 3 mg/L (21.0 months). The median overall survival of patients with a lymph node ratio equal to 0, less than, or equal to, 0.2 and greater than 0.2 was 31, 16, and 9 months, respectively (P<0.001; Figure 2).
Figure 1. Kaplan-Meier cumulative survival curves for patients with
C-reactive protein (CRP) less than, or equal to, 3 mg/L versus CRP
greater than 3 mg/L. (Cox proportional hazards model: P=0.015).
Figure 2. Kaplan-Meier cumulative survival curves for patients with
lymph node ratio 0, less than, or equal to, 0.2 and greater than 0.2.
(Cox proportional hazards model: P<0.001).
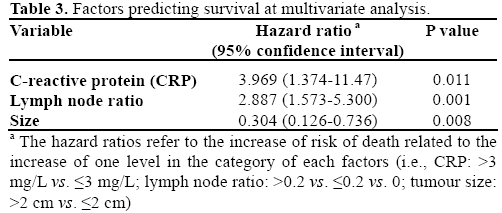
The preoperative serum CRP level retained statistical significance at multivariate analysis (P=0.011), along with lymph node ratio (P<0.001) and tumour size greater than 2 cm (P=0.008) (Table 3).
DISCUSSION
The present study has investigated the prognostic significance of the pre-operative inflammatory response, and post-operative lymph node ratio on survival after pancreatic-head resection for pancreatic ductal adenocarcinoma, and has demonstrated that a pre-operative elevated serum CRP level greater than 3 mg/L and a raised post-operative lymph node ratio are significant independent prognostic factors that predict poor prognosis in patients undergoing curative resection for pancreatic ductal adenocarcinoma.
Previous studies have reported that a number of pathological features related to pancreatic cancer, such as tumour grade, tumour size, vascular and perineural invasion and resection margin status affect prognosis [13, 14, 15]. However, these parameters are assessed post-operatively and are therefore only relevant to predicting prognosis in resected patients. Other prognostic factors have similarly been described primarily for patients with inoperable pancreatic cancer, and these prognosticators of survival have included patient age and gender, clinical presentation, performance status, levels of carbohydrate antigen (CA) 19-9 [16], and, more recently, serum CRP levels [6, 7]. It has been demonstrated that tumour infiltration with CD4+ lymphocytes carries a good prognostic outcome [17] and that plasma CRP levels are inversely related to infiltration of the tumour microenvironment by CD4+ lymphocytes and this in turn carries a poor prognosis [18]. This has been further investigated in pancreatic cancer patients and recent studies have suggested that an elevated serum CRP level is inversely correlated with survival in the palliative setting [6, 7]. Tingstedt et al. [6] recently analysed the role of preoperative elevated preoperative CRP, s-bilirubin and b-haemoglobin levels on survival and have shown that an elevated preoperative CRP level is a strong independent predictor of survival in patients with non resectable pancreatic cancer. Pine et al. [7] also reported that a raised preoperative CRP level at the time of presentation of advanced pancreatic cancer carries a poor prognosis. Patients with preoperative biliary intervention were specifically excluded from the study to exclude patients with raised CRP levels secondary to biliary intervention. Garcia et al. [10] in a recent study did not show any negative impact on elevated preoperative CRP on survival; however, a raised neutrophil/lymphocyte ratio preoperatively was associated with early recurrence post pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. However it was not clear from their data if patients with elevated preoperative CRP secondary to ERCP cholangitis were excluded. This is in contrast to our study where in patients with elevated CRP secondary to ERCP cholangitis were excluded and CRP, but not neutrophil/lymphocyte ratio, was of prognostic significance. Nevertheless, the survival in patients with a low neutrophil/lymphocyte ratio was longer compared to those with high neutrophil/lymphocyte ratio but did not reach statistical significance. Interestingly, preoperative elevated CRP was not associated with increased rates of margin positivity for pancreatic ductal adenocarcinoma and margin positive patients (R1) had similar survival to R0 patients in this study. There is still considerable variation in the literature regarding the role of markers and their value especially platelet/lymphocyte ratio with some studies showing benefit [9] and some showing no benefit [11]. Nevertheless, there is paucity of data in the literature analysing the potential influence of the preoperative inflammatory response in patients with resectable pancreatic cancer, especially CRP, and it is this aspect specifically that was evaluated in this study, as this may help identify a cohort of patients that are most likely to benefit from neo-adjuvant multimodal therapy [19].
In addition to the preoperative inflammatory response, post-operative tumour morphology and histology was analysed to evaluate the role of these factors in prediction of patient survival. Tumour size, margin status, lymph node status, peri-neural invasion, and post-operative lymph node ratio were assessed in this study. Numerous studies have demonstrated that patients with lymph node metastasis have significantly worse survival than do patients with node negative disease [20, 21]. This has led to some surgeons advocating an extended lymphadenectomy for pancreatic cancer but it has never been shown conclusively to improve survival [22]. Evidence extrapolated from studies in colon [23] and gastric cancer [24] suggests that it is the actual number of lymph nodes involved that has an effect on survival, rather than an absolute positive or negative lymph node status. Several series have recently reported that a high lymph node ratio (lymph node ratio greater than 0.2) may in fact be the more critical and relevant independent prognostic factor after resection of pancreatic cancer [25, 26, 27, 28, 29].
Pawlik et al. [21] demonstrated that a high lymph node ratio was an adverse prognostic factor, but also that N0 patients with less than 12 lymph nodes harvested had a bad prognosis when compared to patients with more than 12 lymph nodes harvested. In addition a total of less than 12 lymph nodes examined tended to be associated with a worse long term survival. The impact of absolute numbers of lymph nodes harvested on patient survival was also reported in the study by Berger et al. [25]. It is therefore important that pathology reporting is standardised and that the reporting pathologist locates and examines a minimum number of lymph nodes to ensure accuracy of staging. In the United Kingdom the accepted minimum number of lymph nodes that should be examined after pancreaticoduodenectomy is 15 [30].
There is further recent data suggesting that development of a pancreatic fistula in the postoperative period is associated with early disease recurrence and poor survival after pancreaticoduodenectomy [31]. However, in the present study no such negative or adverse association was noted between post-operative pancreatic fistula and overall patient survival (median survival 13.2 versus 17.2 months; P=0.880).
This study has shown that the lymph node ratio is an independent prognostic factor that predicts overall survival in patients following curative resection of ductal adenocarcinoma of the pancreas, and concurs with recently published studies that suggest that lymph node ratio rather than total numbers of metastatic lymph nodes involved is the key to risk stratification and potential tailoring of multi-modal adjuvant treatment strategies [32].
In addition this study has evaluated the impact of preoperative inflammatory markers on survival following curative resection for pancreatic ductal adenocarcinoma, and the results show that an elevated preoperative serum CRP level is an independent prognostic indicator for post-operative survival in pancreatic adenocarcinoma. Therefore, a serum CRP level may be a useful marker that can be used to stratify patients into prognostic categories preoperatively along with other potential prognostic markers such as serum CA 19-9 levels [16, 27].
In conclusion this study adds to the body of evidence suggesting that an elevated preoperative CRP and postoperative lymph node ratio may predict a poor prognosis of pancreatic ductal adenocarcinoma. The ability to identify high-risk patient cohorts has potential benefit in both the pre-operative and post-operatively setting and may help to tailor neo-adjuvant and adjuvant multi-modal treatment strategies.
Acknowledgements
Presented as a poster at the 9th World Congress of the International Hepato-Pancreato- Biliary Association, Buenos Aires, Argentina; April 18- 22, 2010. Published as abstract [33]
Conflicts of interest
The authors have no potential conflicts of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer Statistics, 2009. CA Cancer J Clin. 2009 Jul-Aug;59(4):225-49
- Office of National Statistics. Cancer survival rates, Cancer Survival: England and Wales. Newport, South Wales, United Kingdom: 03 January, 2005. (https://www.ons.gov.uk/ons/publications/re-reference-tables.html?edition=tcm%3A77-252716).
- Richter A, Niedergethmann M, Sturm JW, Lorenz D, Post S,Trede M. Long-term results of partial pancreatico duodenectomy forductal adenocarcinoma of the pancreatic head: 25-year experience.World J Surg 2003;27:324-9.
- Benassi G, Mastrorilli M, Quarto G, et al. Factors influencing survival after resection for ductal adenocarcinoma of the head of the pancreas. J Surg Oncol 2000;73:212-8.
- Yeo CJ, Cameron JL, Sohn TA, et al. Six hundred fifty consecutive pancreatico duo denectomies in the 1990s: pathology, complications, and outcomes. Ann Surg 1997;226:248-60.
- Tingsted B , Johansson P , Andersson A, Andersson R. Predictive factors in pancreatic ductal adenocarcinoma: Role of the inflammatory response. Scandinavian Journal of Gastroenterology. 2007, Vol. 42, No. 6, Pages 754-759.
- Pine JK, Fusai KG, Young R, Sharma D, Davidson BR, Menon KV, Rahman SH. Serum C-reactive protein concentration and theprognosis of ductal adenocarcinoma of the head of pancreas. Eur J Surg Oncol 2009;35: 605-610.
- Clark EJ, Connor S, Taylor MA, Madhavan KK, Garden OJ, Parks RW. Preoperative lymphocyte count as a prognostic factor inresected pancreatic ductal adenocarcinoma. HPB, 2007; 9: 456-460
- Smith RA, Bosonnet L, Raraty R, Sutton R, Neoptolemos JP, Campbell F, Ghaneh P. Preoperative platelet-lymphocyte ratio is anindependent significant prognostic marker in resected pancreatic ductal adenocarcinoma. Am J Surg 2009; 197, 466-472.
- Garcea G, Ladwa N, Neal CP, Metcalfe MS, Dennison AR, Berry DP. Preoperative neutrophil-to-lymphocyte ratio (NLR) is associated with reduced disease-free survival following curative resection of pancreatic adenocarcinoma. World J Surg. 2011 Apr;35(4):868-72.
- Bhatti I, Peacock O, Lloyd G, Larvin M, Hall. Preoperative hematologic markers as independent predictors of prognosis inresected pancreatic ductal adenocarcinoma: neutrophil-lymphocyte versus platelet-lymphocyte ratio. Am J Surg. 2010 Aug;200(2):197-203.
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J,et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005 Jul;138(1):8-13
- Greer RJ, Brennan MF. Resection of pancreatic adenocarcinoma: prognostic indicators for survival. Am J Surg 1993;195:68-73.
- Yeo CJ, Cameron JL, Lillemoe KD, et al. Pancreatico duo denectomy with or without distal gastrectomy andextended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, part 2: randomised controlled trial evaluating survival, morbidity and mortality. Ann Surg 2002;236:355-68.
- Verbeke CS, Leitch D, Menon KV, McMahon MJ, Guillou PJ, Anthoney A. Redefining the R1 resection in pancreatic cancer. Br J Surg 2006;93:1232-7.
- Kau SY, Shyr YM, Su CH, et al. Diagnostic and prognostic values of CA19-9 and CEA in periampullary cancers. J Am Coll Surg 1999; 188:415-20.
- Ali AA, Mc Millan DC, Matalka II, Mc Nicol AM, Mc Ardle CS.Tumour T-lymphocyte subset infiltration and tumour recurrence following curative resection for colorectal cancer. Eur J Surg Oncol 2004;30:292-5.
- Canna K, Mc Ardle PA, Mc Millan DC, et al. The relationship between tumour T-lymphocyte infiltration, the systemic inflammatory response and survival in patients undergoing curative resection for colorectal cancer. Br J Cancer 2005;92:651-4.
- Artinyan A, Anaya DA, McKenzie S, Ellenhorn JD, Kim J.Neoadjuvant therapy is associated with improved survival inresectable pancreatic adenocarcinoma. Cancer 2011;15:2044-9.
- Lim JE, Chien MW, Earle CC. Prognostic factors following curative resection for pancreatic adenocarcinoma: a population based, linked database analysis of 396 patients. Ann Surg2003;237:74-85.
- Pawlik TM, Abdalla EK, Barnett CC, Ahmad SA, Cleary KR,Vauthey JN, et al. Feasibility of a randomized trial of extended lymphadenectomy for pancreatic cancer. Arch Surg 2005;140:589-91.
- Kennedy EP, Yeo CJ. Pancreatico duo denectomy with extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma.Surg Oncol Clin N Am. 2007 Jan;16(1):157-76
- Vaccaro CA, Im V, Rossi GL, Quintana GO, Benati ML, Perezde Arenaza D, Bonadeo FA. Lymph node ratio as prognosis factor forcolon cancer treated by colorectal surgeons. Dis Colon Rectum. 2009Jul;52(7):1244-50.
- Huang C, Lin J, Zheng C, Li P, Xie J, Lin B, Wang J. Prognostic impact of metastatic lymph node ratio on gastric cancer after curativedistal gastrectomy. World J Gastroenterol 2010 April 28; 16(16):2055-2060
- Berger AC, Watson JC, Ross EA, Hoffman JP. Themetastatic/examined lymph node ratio is an important prognostic factor after pancreatico duo denectomy for pancreatic adenocarcinoma. Am Surg 2004;70:235-40
- Riediger H, Keck T, Wellner U, zurHausen A, Adam U, HoptUT, Makowiec F. The lymph node ratio is the strongest prognostic factor after resection of pancreatic cancer. J Gastrointest Surg. 2009Jul;13(7):1337-44.
- Smith RA, Bosonnet L, Ghaneh P, Raraty M, Sutton R, Campbell F, Neoptolemos JP. Preoperative CA 19-9 levels and lymphnode ratio are independent predictors of survival in patients with resected pancreatic ductal adenocarcinoma. Dig Surg. 2008;25(3):226-32.
- Partelli S, Fernandez-Del Castillo C, Bassi C, Mantovani W,Thayer SP, Crippa S, et al. Invasive intraductal papillary mucinouscarcinomas of the pancreas: predictors of survival and the role of lymph node ratio. Ann Surg. 2010 Mar;251(3):477-82
- Bhatti I, Peacock O, Awan AK, Semeraro D, Larvin M, Hall RI.Lymph node ratio versus number of affected lymph nodes aspredictors of survival for resected pancreatic adenocarcinoma. World J Surg. 2010 Apr;34(4):768-75.
- The Royal College of Pathologists of UK. Dataset for the histopathological reporting of carcinomas of the pancreas, ampulla ofVater and common bile duct. May 2010. https://www.rcpath.org/resources/pdf/datasethistopathologicalreportingcarcinomasmay10.pdf
- Nagai S, Fujii T, Kodera Y, Kanda M, Sahin TT, Kanzaki A, etal. Recurrence pattern and prognosis of pancreatic cancer after pancreatic fistula. Ann Surg Oncol . 2011 Aug;18(8):2329-37.
- Li J, Yee Merl M, Chabot J, Saif MW. Updates of Adjuvant Therapy in Pancreatic Cancer: Where Are We and Where Are WeGoing? JOP. J Pancreas (Online) 2010 Jul 5; 11(4):310-312.
- Sanjay P, Leaver H, Polignano FC, Kulli C, Tait I. Preoperative C-reactive protein and lymph node ratio are important predictors ofsurvival for pancreatic ductal adenocarcinoma. HPB 2010;12(S1):223.


