Keywords
Body Weight Changes; Insulinoma; signs and symptoms
INTRODUCTION
An insulinoma is an insulin-secreting neoplasm of
the pancreas. A common symptom of insulinoma is a
hypoglycemic state which presents clinically as Whipple's
triad, although symptoms are reported as varied with an
insulinoma [1]. The estimated incidence of insulinoma is
1–4 cases per million person-years making it a rare disease
[2]. Consequently, the diagnosis of insulinoma is difficult
and often delayed [1, 3]. In the period from first symptoms
until treatment, insulinoma patients can experience
repeated hypoglycemic events. Some patients gain weight
when they relieve insulinoma-induced hypoglycemic
symptoms by ingesting excess food [1]. In this study, we
focus on the changes in body weight in patients with an
insulinoma and the relationships of those changes to other
clinicopathological factors and clinical data.
PATIENTS AND METHODS
Nineteen patients with insulinoma who underwent
curative surgical treatment at Kagoshima University
Hospital, Kagoshima, Japan, between 1995 and 2016 were
enrolled in this study. Clinical information, including age, gender, symptoms, and various data from examinations
were obtained from medical records retrospectively. The
onset of insulinoma was defined at the time when first
syndrome related with insulinoma was appeared. The
time was decided by the interview for the patients and
information from their previous doctors. Body weight
change from the first syndrome to the operation was taken
by interviews for each patient. All interviews were done
before the operation independently from this study.
Patients had undergone several blood chemistry tests
before treatment, so we collected as much data as possible.
Excluding data during various load tests, we extracted the
minimum serum glucose and maximum serum insulin
concentrations among collected data and adopted them as
data representative of each patient. All patients provided
written informed consent before data acquisition. This
study was approved by the Institutional Review Board of
Kagoshima University Hospital.
Statistical analysis was performed using JMP Pro,
version 12.1.0 for Mac OS (SAS Institute Japan Ltd.,
Tokyo, Japan). P values of less than 0.05 were considered
statistically significant.
RESULTS
Patient characteristics
The clinicopathological features of our cohort are
shown in Table 1. This study included 19 patients (14
women [74%] and five men), average age 52.5 years,
average weight just before operation 70.0 kg. All patients
had been diagnosed with insulinoma before surgery and were confirmed pathologically. One patient (5%) had
multiple lesions, and the one other patient (5%) had a
malignant insulinoma. Two patients (11%) were found
to also have multiple endocrine neoplasia type 1 (MEN1).
Between the first symptom and surgery, the median time
that elapsed was 31.2 months (range, 2 to 216). Eighteen of
19 patients had obvious symptoms related hypoglycemic
state, but 1 patient had only epigastric pain. For him, we
consider epigastric pain was the symptom by insulinoma.
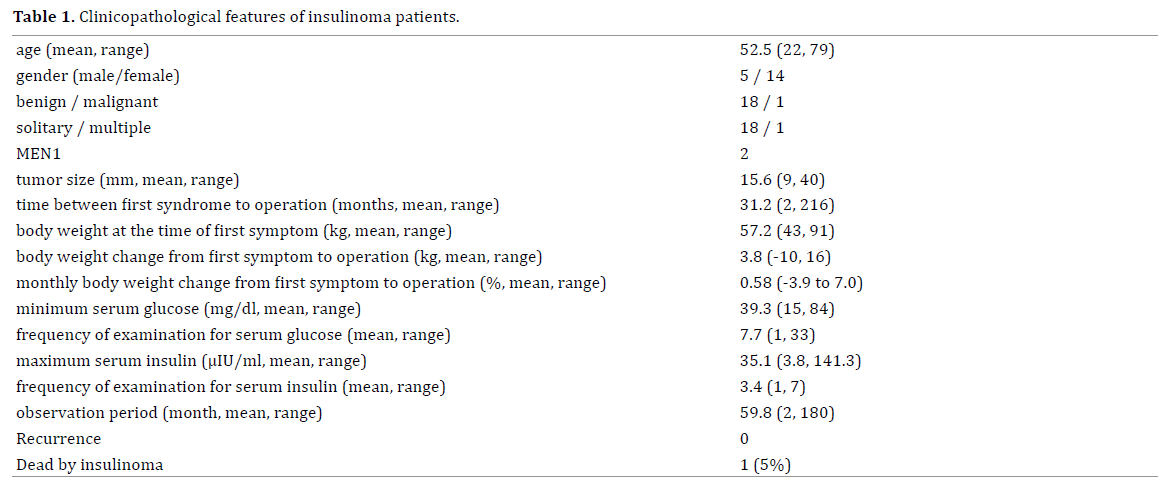
Of the 19 patients, 8 patients (42%) gained weight
and 1 patient (5%) lost weight. The median monthly
net change in body weight was 0.58 (range, -3.9 to 7.0)
between the first symptom and surgery. Overall, among
patients the average minimum serum glucose was 39.3
mg/dL and the average maximum serum insulin was 35.1
μIU/mL. After a mean follow-up period of 59.8 months, no
patients, other than the patient with a malignancy who had
a 40 mm tumor, was dead by insulinoma. This patient had
liver metastasis before operation and died 39 months after
operation. This patient had a minimum serum glucose of
33 mg/dL and his maximum serum insulin was 141.3 μIU/
mL. Within the 3 months prior to surgery, this patient had
an 18% increase in his body weight.
Relationships among Various Clinical Data
First, the relationships between tumor size, serum
blood glucose, and serum insulin concentrations were
examined. The size of each tumor was based on pathological
findings, and the one multiple tumor case was excluded.
Among the many preoperative serum values documented
for glucose and insulin, we elected to evaluate minimum
serum glucose values and maximum serum insulin values.
The relationships between these values are shown in Figure 1. A significant correlation was evident only
between tumor size and serum insulin concentrations.
The analysis of monthly changes in body weight from the
time between the first symptoms until surgery showed
significant correlations with tumor size and serum insulin
concentrations, but not significant correlation with serum
glucose concentrations (Figure 2).
Figure 1. The relationship between (a). tumor size and serum glucose and (b). tumor size and serum insulin and (c). serum insulin and serum glucose. Each
correlation coefficient and p-value is shown.
Figure 2. The relationships between (a). tumor size and change in body weight (b). serum glucose and change in body weight, and (c). serum insulin values
and change in body weight. *Change in body weight is from first symptoms until surgery. Each correlation coefficient and p-value is shown.
DISCUSSION
In this study, we examined the relationships between
various preoperative clinical laboratory data of patients
with insulinoma who had a varied disease presentation.
This disease characteristic can make the diagnosis of
insulinoma difficult. These patients typically report a
variety of hypoglycemic symptoms that differ in frequency
from patient to patient. Frequent symptoms often induce
patients with insulinoma to eat many times in a day in
order to mitigate their symptoms which can result in a net
increase in their body weight. In fact, a gain in body weight
is one of the most common signs of insulinoma and occurs
in 39–42% of patients [1, 4]. In our analysis, eight patients
(42%) gained weight and one patient (5%) lost weight,
a finding that is consistent with previous reports [1, 4].
We hypothesized that changes in body weight occurring
from symptom onset until the time of surgery reflect the
severity of the disease process in patients with insulinoma.
The duration of this period differed among patients, so we
used monthly changes in body weight during our analysis.
When we evaluated the relationships between tumor size
and serum glucose, as well as between tumor size and
serum insulin, only serum insulin concentrations were
significantly correlated (Figure 1). And we determined
that monthly changes in body weight were significantly
correlated with tumor size and serum insulin concentration
(Figure 2). Based on these results, we propose that
changes in body weight reflect the clinical characteristics
of insulinoma as well as the severity of clinical findings for
this disease to some extent. To the best of our knowledge,
correlations between changes in body weight and other
clinical factors in patients with insulinoma have not been
reported previously.
In our study cohort, the one patient who lost weight
preoperatively was treated with diazoxide after diagnosis
and experienced nausea and loss of appetite, adverse
effects that contributed to the decrease in body weight
at that time. Diazoxide is a nondiuretic benzothiadiazine
derivative used for relieving hypoglycemic symptoms in patients with insulinoma [5, 6]. In total, adverse effects
were reported for 4 out of 4 patients treated with diazoxide
in our cohort and overall, diazoxide use was intermittent.
Three of these patients gained weight, and as previously
described, one patient lost weight preoperatively indicating
our data were not affected by diazoxide usage, but rather
the outcomes reflect the natural course of insulinoma in
these patients.
The criteria for insulinoma are plasma glucose <55
mg/dL, serum insulin of at least 3.0 μU/mL, and C-peptide
of at least 0.6 ng/mL [7, 8]. In our cohort, the criteria
were met by 17 out of 19 patients (89%) for glucose
and all 19 patients (100%) met the insulin criteria.
Laboratory data were collected for patients across several
hospitals at multiple time points, yielding several values
for each patient; however, we elected to evaluate the
minimum glucose concentrations and maximum insulin
concentrations of patients. C-peptide was not evaluated
in this study because it was not consistently examined or
documented for our cohort. Various load tests, such as
the leucine loading test, tolbutamide test, and glucagon
test [9, 10] were also not routinely performed; hence, we
could not properly evaluate those results in this study.
Fifteen patients (79%) underwent arterial stimulation
venous sampling [11, 12] for diagnosis of localization of
insulinoma preoperatively.
Limitations of this study include the small number of
patients given the rarity of this disease and our cohort
did not include patients with insulinoma who were
not treated surgically. To further elucidate the clinical features of insulinoma, it will be necessary to evaluate
a larger number of patients independent of treatment
procedures.
CONCLUSION
Preoperative changes in body weight were significantly
correlated with tumor size and serum concentrations
of insulin, but not with serum concentrations of glucose.
Preoperative changes in body weight are one of important
parameters indicative of the severity of insulinoma.
Conflict of Interest
All authors had no conflicts of interest.
References
- Dizon AM, Kowalyk S, Hoogwerf BJ. Neuroglycopenic and other
symptoms in patients with insulinomas. Am J Med 1999; 106:307-10.
[PMID: 10190379]
- Okabayashi T, Shima Y, Sumiyoshi T, Kozuki A, Ogawa Y, Kobayashi
M, et al. Diagnosis and management of insulinoma. World J Gastroenterol
2013; 19: 829-37. [PMID: 23430217]
- Service FJ, McMahon MM, O'Brien PC, Ballard DJ. Functioning
insulinoma--incidence, recurrence, and long-term survival of patients: a
60-year study. Mayo Clin Proc 1991; 66:711-9. [PMID: 1677058]
- Chen X, Cai WY, Yang WP, Li HW. Pancreatic insulinomas: diagnosis
and surgical treatment of 74 patients. Hepatobiliary Pancreat Dis Int
2002; 1:458-61. [PMID: 14607727]
- Gill GV, Rauf O, MacFarlane IA. MacFarlane, Diazoxide treatment
for insulinoma: a national UK survey. Postgrad Med J 1997; 73:640-1.
[PMID: 9497974]
- Komatsu Y, Nakamura A, Takihata M, Inoue Y, Yahagi S, Tajima K, et al.,
Safety and tolerability of diazoxide in Japanese patients with hyperinsulinemic
hypoglycemia. Endocr J 2016; 63:311-4. [PMID: 26598136]
- Tseng HC, Yao CZ, Zhong SX, Zhang JX, Zhu Y. Percutaneous
transhepatic portal vein catheterization for localization of insulinoma.
World J Surg 1984; 8:575-82. [PMID: 6091348]
- Anakal MG, Kalra P, Dharmalingam M, Indushekhar S, Rao V, Prasanna
Kumar KM. Insulinoma case series: Experience of a tertiary care center.
Indian J Endocrinol Metab 2014; 18:858-62. [PMID: 25364684]
- Ohneda A, Maruhama Y, Itabashi H, Horigome K, Yanbe A, Ishii S, et al.
Diagnostic value of intravenous glucagon test in insulinoma. Tohoku J Exp
Med 1975; 116: 205-11. [PMID: 170711]
- Marks V, Samols E. Glucagon test for insulinoma: a chemical study in
25 cases. J Clin Pathol 1968; 21:346-52. [PMID: 4301688]
- Tseng LM, Chen JY, Won JG, Tseng HS, Yang AH, Wang SE, et al.
The role of intra-arterial calcium stimulation test with hepatic venous
sampling (IACS) in the management of occult insulinomas. Ann Surg
Oncol 2007; 14:2121-7. [PMID: 17431724]
- Morganstein DL, Lewis DH, Jackson J, Isla A, Lynn J, Devendra
D, et al. The role of arterial stimulation and simultaneous venous
sampling in addition to cross-sectional imaging for localisation of
biochemically proven insulinoma. Eur Radiol 2009; 19:2467-73.
[PMID: 19597822]



