Hazelzet T1*, Patrier S2, Barre E1, Labadie G3, Wilmort V3, Durand II1 and David N1
1Department of Congenital Cardiology, Rouen University Hospital, 1 Rue de Germont, 76031 Rouen, France
2Department of Pathology, Rouen University Hospital, 1 Rue de Germont, 76031 Rouen, France
3Department of Gynaecology and Obstetrics, Hopital du Belvedere, 72 Rue Louis Pasteur, 76131 Mont Saint Aignan, France
*Corresponding Author:
Tristan Hazelzet
Department of Congenital Cardiology, Rouen University Hospital, Rue de Germont, 76031 Rouen, France
Tel: (33)-232888755
Fax: (33)-23288
E-mail: tristan.hazelzet@chu-rouen.fr
Received date: February 29, 2016 Accepted date: March 14, 2016 Published date: March 17, 2016
Keywords
Foetus; Pulmonary agenesis; Left pulmonary artery sling; Total anomaly of pulmonary venus return
Case Report
A 32 year-old woman, gravida 3, para 2 was referred for fetal echocardiographic investigation of dextrocardia at 23 weeks’ of gestation. No extrathoracic anomalies were observed except for bilateral preauricular tags.
Cardiac ultrasound examination (ALOKA alpha 10 echograph) demonstrated that dextrocardia was caused by right pulmonary agenesis (PA). There was no left pulmonary artery (LPA) in the expected location (Figure 1a).
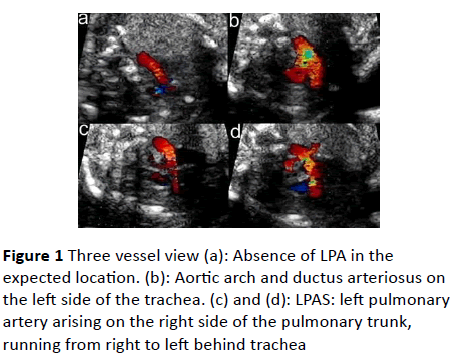
Figure 1 Three vessel view (a): Absence of LPA in the expected location. (b): Aortic arch and ductus arteriosus on the left side of the trachea. (c) and (d): LPAS: left pulmonary artery arising on the right side of the pulmonary trunk, running from right to left behind trachea
A small pulmonary artery araised from the right side of the pulmonary trunc, ran posteriorly between the trachea and oesophagus and reached the left hilum (Figure 1c and 1d). The trachea seemed narrow (Figure 1d).
Cardiothoracic index was higher than normal with no hemodynamic anomaly. Pulmonary veins were not visible in the left atria and an abnormal vein was seen running along the left atrial roof, from the left lung to the superior vena cava (Figure 2). There were no other intracardiac defects. Genetic investagation showed a normal karyotype 46XX and absence of 22Q1.1. microdeletion. The patient opted for pregnancy termination.
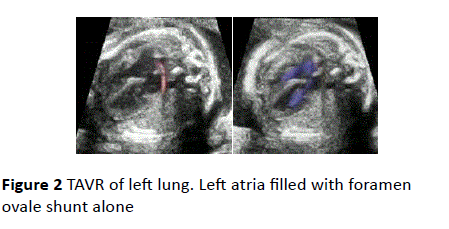
Figure 2 TAVR of left lung. Left atria filled with foramen ovale shunt alone
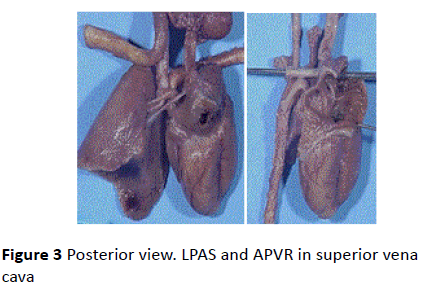
Figure 3 Posterior view. LPAS and APVR in superior vena cava
Post-Mortem Examination
Post-mortem analysis confirmed agenesis of the right lung with no parenchyma, right pulmonary artery or veins and no right bronchus. The thymus filled the upper right chest, and the right hemidiaphragm was elevated. The left lung had only one lobe. A single left pulmonary vein was connected to superior vena cava. The left lung was vascularised by the LPAS, arising from the right side of the pulmonary trunk and circumventing the trachea. The LPAS compressed the lower part of the trachea but there was no structural anomaly.
Discussion
PA is defined by a total absence of the pulmonary parenchyma, vascular structures and bronchi. It is an uncommon anomaly in which there are frequent pulmonary, cardiovascular, tracheal, renal, facial, skeletal and urogenital associated anomalies. Association of PA with syndromes (DiGeorge, Goldenhar, VACTERL) is frequent [1]. In our case, the presence of bilateral preauricular tags raised the question of a genetic syndrome.
The clinical presentation of unilateral PA is variable. Symptoms may appear soon after delivery, or the patient may remain asymptomatic, and be diagnosed during routine examination.
LPAS is a rare vascular anomaly in which the left pulmonary branch originates from the right pulmonary artery, passes over the right main stem bronchus, turns to the left, and courses between the trachea and oesophagus to reach the left lung. One case of prenatal diagnosis has been reported [2]. Neonatal presentation depends on associated tracheal and cardiac anomalies [3,4]. Tracheal narrowing is constant in LPAS with right pulmonary agenesis. Prenataly, it is difficult, to differentiate intrinsic tracheal stenosis with cartilaginous rings, from vascular compression [4]. Cardiac malformation is a major pronostic factor when early hemodynamic changes occur. In our case, early congestive heart failure and severe pulmonary hypertension could have been expected because of total TAVR. Left pulmonary hypoplasia was suspected due to enlarged cardio thoracic ratio without hemodynamic disease. Left pulmonary hypoplasia would have worsened prognosis.
Despite surgical progress, the management of very young infants with LPAS and major associated malformations remains of very poor prognosis [5-9]. Accurated expertise is required in prenatal diagnosis to assess the risk of surgical correction.
References
- Lin JH, Chen SJ, Wu MH, Wang JK, Li YW, et al. (2000) Right lung agenesis with left pulmonary artery sling. Pediatr Pulmonol 29(3): 239-241.
- Yorioka H, Kasamatsu A, Kanzaki H, Kawataki M, Yoo SJ (2011) Prenatal diagnosis of fetal left pulmonary artery sling. Ultrasound Obstet Gynecol 37(2): 245-246.
- Chen SJ, Lee WJ, Lin MT, Wang JK, Chang CI, et al. (2007) Left pulmonary artery sling complex: computed tomography and hypothesis of embryogenesis. Ann Thorac Surg 84(5): 1645-1650.
- Wang JH, Ding GC, Zhang MY, Liu M, Niu HY (2011) Clinical and imaging features of pulmonary artery sling in infants without significant hemodynamic changes. Chin Med J 124(20): 3412-3414.
- Backer CL, Kelle AM, Mavroudis C, Rigsby CK, Kaushal S, et al. (2009) Tracheal reconstruction in children with unilateral lung agenesis or severe hypoplasia. Ann Thorac Surg. 88(2): 624-630.
- Backer CL, Russell HM, Kaushal S, Rastatter JC, Rigsby CK et al. (2012) Pulmonary artery sling: current results with cardiopulmonary bypass. J Thorac Cardiovasc Surg 143(1): 144-151.
- Berdon WE, Muensterer OJ, Zong YM, Backer CL (2011) The triad of bridging bronchus malformation associated with left pulmonary artery sling and narrowing of the airway: the legacy of Wells and Landing. Pediatr Radiol 42(2): 215-219.
- Pierron C, Sigal-Cinqualbre A, Lambert V, Le Bret E (2011) Left pulmonary artery sling with right lung aplasia. J Pediatr Surg 46(11): 2190-2194.
- Zhong YM, Jaffe RB, Zhu M, Gao W, Sun AM, et al. (2010) CT assessment of tracheobronchial anomaly in left pulmonary artery sling. Pediatr Radiol 40(11):1755-1762.

