Keywords
Pancreatitis; Morbidity; Mortality
Abbreviations
SPSS Statistical Package for the Social Sciences
INTRODUCTION
Acute pancreatitis (AP) is an inflammatory process
of the pancreas that affects approximately 4.9 to 35 per
100,000 in the general population [1]. It is the leading
cause of gastrointestinal hospital admission [2]. A large
epidemiological study found that between 1988 and 2003,
the mortality from acute pancreatitis decreased from 12% to
2% with a higher incidence of mortality among black males
in their early 50’s [3]. Overall mortality of patients with acute
pancreatitis admitted to the hospital is estimated to be 5% to
10% varying from 3% in mild AP to 30% in severe AP [4, 5].
With significant risk of morbidity and mortality
associated with acute pancreatitis, multiple scoring
systems have been developed to assess its severity.
However, no single scoring system has been shown to be
superior to others in predicting in-hospital mortality [6, 7]. One of the early systems, Ranson’s criteria, focuses
on 11 factors with 5 assessed at the time of admission
and 6 assessed 48 hours into admission. For scores <3,
mortality was estimated to be 0% to 3%, scores ≥3 were
associated with a 11% to 15% mortality, and scores ≥6 were associated with a 40% mortality. Although used
widely, a meta-analysis showed that Ranson’s criteria had
poor predictive value for acute pancreatitis severity [8].
Acute Physiology and Chronic Health Examination
(APACHE) II, another cumbersome scoring system, was
developed for use with critically ill patients, limiting
its applicability. The APACHE II score uses age and 12
physiologic measures and can be calculated each day.
Several studies have shown that an APACHE II score of less
than 8 has a mortality rate <4% while a score greater than
8 results in mortality between 11% to 18% [5, 9].
Bedside Index of Severity in Acute Pancreatitis (BISAP)
is a simpler calculation for determining early in-hospital
mortality of patients admitted for acute pancreatitis. A
BISAP score uses point assignments: 1 point for each of the
following - BUN >25 mg/dL, abnormal mental status with
Glasgow Coma Scale score <15, evidence of Systematic
Inflammatory Response Sydrome (SIRS), >60 years of age,
and imaging revealing pleural effusion. Patients with a
score of zero have less than 1% mortality while a score of
3 to 5 is associated with >15% mortality.
A recent validation study found that BISAP had similar
performance to APACHE II and Ranson’s criteria [10].
Moreover, BISAP compares favorably with newer scoring
systems for bedside AP assessment, such as the “harmless
acute pancreatitis score” and the “CT severity index” [10, 11].
In sum, AP severity scores are often unwieldy to measure
and may require recalculation at later times during the
hospital admission. In contrast, rather than focus on an AP score or index, other studies have investigated patient
demographics (e.g., age), clinical characteristics (e.g., BMI,
SIRS), various laboratory values, and radiological findings
to determine AP severity and risk of mortality [12, 13, 14].
We examined selected demographic factors,
comorbidities, and health care system characteristics that
might be predictors of morality in hospitalized patients
with acute pancreatitis.
METHODS
Study data was acquired from the National Hospital
Discharge Survey (NHDS), which is collected every year
through the National Center for Health Statistics.
The NHDS collects patient hospitalizations and
discharges from nonfederal hospitals across the United
States with average length of stay of <30 days and ≥6 beds.
Patient data in the NHDS is de-identified and made available
to the public via the Center for Disease Control, making it
exempt from an Institutional Review Board. The NHDS
database was searched using International Classification
of Diseases – Ninth Revision (ICD-9) diagnosis codes for
patients admitted to hospitals with acute pancreatitis
(ICD-9 code 577.0) from 2001-2010. For all patients
included in the study, the following data was obtained:
patient demographics (age, sex, race, marital status),
hospital length of stay (LOS), hospital size (by number of
beds), location/ownership (proprietary, government, or
church/nonprofit), type of admission (emergency/urgent/
elective), source of admission, comorbidity burden, and
mortality. This cohort was separated into two groups:
those who died during the hospitalization and those who
survived the hospitalization.
Means and standard deviations are reported for
continuous variables, and counts and percents for
categorical variables. The independent samples Mann-
Whitney Test was used for comparisons involving the two
groups (mortality vs. no mortality) and a second variable
measured on a continuous scale. The chi square test was
used to compare the two groups on categorical variables.
Inferences for these univariate statistical tests were made
at the 0.05 level of significance with no corrections for
multiple comparisons. Multivariable logistic regression
was used to identify independent risk factors of mortality.
Data was first recorded in Excel, and analyses were conducted
using IBM SPSS Statistics 23.0 (IBM, Armonk, NY).
RESULTS
Table 1 shows the results for 27,259 patients admitted
for acute pancreatitis during the 2001-2010 periods. Of
this group, 573 (2.1%) suffered in-hospital mortality. The
mean age of patients who died was 64.5 years, which was
significantly higher than the survival group’s mean age of
51.8 years (p<0.001). Only two races had a large number
of patients: white (n=13,610) and African-American/
black (n=4984), and there was no difference in mortality
between these two groups (white 2.3% vs. A-A/black
2.2%; p=0.55).
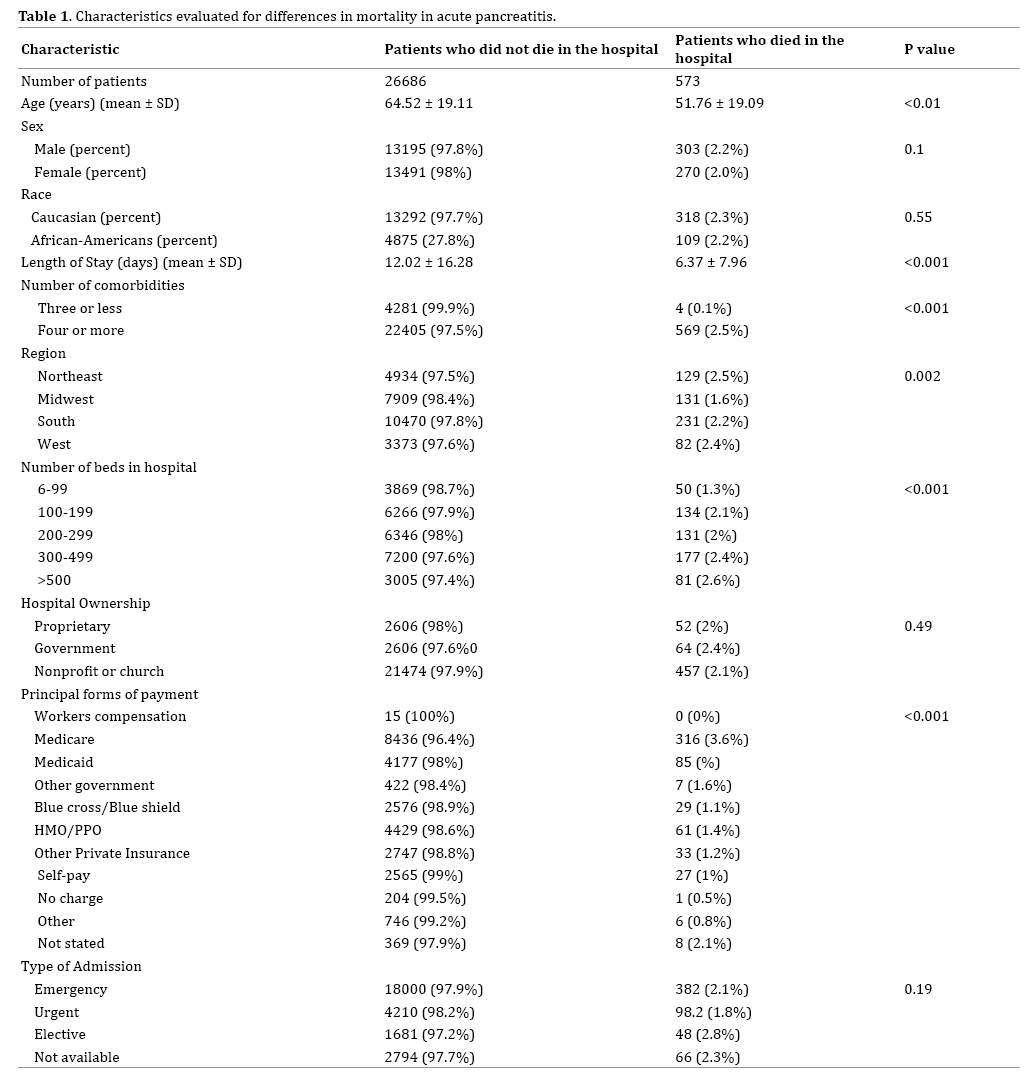
Mean length of stay was nearly double (12.0 vs. 6.4
days, p<0.001) in the mortality group. Patients with four
or more comorbidities had a significantly higher mortality
rate (2.5%) compared to those with three or fewer
comorbidities (0.1%) (p<0.001).
Mortality was greater as hospital size increased,
with the largest hospitals having the highest mortality
rate (2.6%) and the smallest hospitals having the lowest
mortality rate (1.3%) (p<0.001). Mortality did not differ
by type of hospital ownership (p=0.49). Of the 10 principal
forms of payment, Medicare patients had significantly
higher mortality (3.6%) than patients with other insurers
– e.g., Medicaid (2.0%), HMO/PPO (1.4%), and self-pay
(1.0%) (p<0.001).
Mortality did not differ by type of admission (emergency
n=18,382; urgent n=4,287; and elective n=1,729). Elective
patients had a mortality rate of 2.8%, emergency 2.1%, and
urgent 1.8% (p=0.06). The hospitals in the Midwest had a
lower mortality rate (1.6%) compared to the Northeast
(2.5%), South (2.2%), and West (2.4%) (p=0.002).
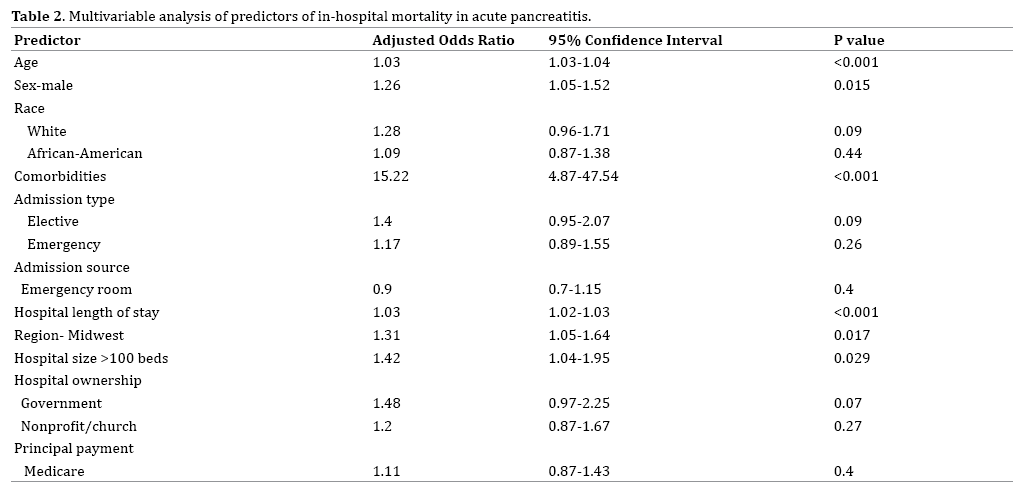
Multivariable logistic regression (MLR) analysis was
used to identify independent predictors of mortality.
Predictors entered into the MLR equation were: age, sex,
race (white, African-American, other), comorbidities (3
or fewer, 4 or more), admission type (emergency, urgent,
elective), hospital length of stay, hospital region (Midwest,
other 3 regions), hospital size (99 or fewer beds, 100 or
more beds), hospital ownership (proprietary, government,
church/nonprofit), and principal payment (Medicare, 9
other insurers)
Table 2 shows the six independent risk factors.
The highest adjusted odds ratio (AOR) was four or
more comorbidities (AOR=15.22 [95% CI=4.87-47.54];
p<0.001), followed by hospital size of 100 beds or more
(AOR=1.42 [95% CI=1.04-1.95]; p=0.029), Midwest
region (AOR=1.31 [95% CI=1.05-1.64]; p=0.017), male
sex (AOR=1.26 [95% CI=1.05-1.52]; p=0.015), increasing
age (AOR=1.03 [95% CI=1.03-1.04]; p<0.001), and longer
hospital LOS (AOR=1.03 [95% CI=1.02-1.03]; p<0.001).
DISCUSSION
Using the National Hospital Discharge Survey (NHDS)
database, we identified six independent risk factors of
in-hospital mortality in acute pancreatitis patients: four
or more comorbidities, larger hospital size, treatment
outside the Midwest region, male sex, older age, and longer
hospital length of stay.
Our finding that AP patients with four or more
comorbidities are at increased risk of mortality is in
agreement with earlier studies [15, 16, 17]. Singh et al.
found a number of associations between various comorbid
conditions and mortality in patients with interstitial
pancreatitis [15]. Frey et al. reported that an increasing
number of chronic comorbidities were associated with
higher morality for acute pancreatitis [16]. These authors
also noted that older patients were more likely to die during their hospitalization with AP. An epidemiological study
conducted in Japan found that patients older than 70 years
with severe comorbidities (>3 comorbid conditions) had
twice the risk of in-hospital mortality [17]. Also, Murata
et al. showed that cardiovascular and renal diseases are
factors that increase hospital length of stay and mortality
among AP patients [14]. With more comorbid conditions,
patients increase their likelihood of developing end organ
damage [18]. In our study, patients in the in-hospital
mortality group had a longer LOS. However, due to
multiple pre-existing comorbidities, those with longer LOS
may have had more complications. Others have found that
in-hospital mortality was higher in obese patients [19].
We found that in-hospital mortality varied by
geographical location. Midwestern states had a lower
mortality rate compared to Southern, Western, and
Northeastern states. These regional differences amongst
hospitals may be related to demographic (e.g., age),
clinical (e.g., obesity, number of comorbidities), and
socioeconomic (e.g., poverty) factors, population size, and
number of medical facilities per capita.
The scoring systems currently utilized to predict
mortality in patients with acute pancreatitis are often
inconvenient to calculate and do not facilitate efficient
triaging. Investigators have used serum markers and
radiological findings to predict AP severity and mortality. To our knowledge, no prior research has used the NHDS
database to examine demographic factors, comorbidities,
and health care system characteristics that may be
related to in-hospital mortality in patients with acute
pancreatitis.
While type of hospital ownership (proprietary,
government, or owned by a non-profit organization or
church) had similar rates of in-patient mortality, smaller
hospitals had lower mortality rates. Smaller hospitals
may manage primarily milder cases of acute pancreatitis
with patients having severe pancreatitis and related
complications transferred to large facilities more capable
of handling critically ill patients. Future investigations of
facility transfer related to pancreatitis may reveal why
mortality is lower in smaller hospitals.
Additionally, patients with Medicare as their primary
insurance had higher in-hospital mortality compared
to other forms of payment. However, the Medicare/
mortality relationship found with the univariate analysis
was not significant in the multivariable model. As
mentioned earlier, unfavorable demographic, clinical, and
socioeconomic factors may be more prevalent in Medicare
patients than with those having commercial and private
insurance coverage.
Mortality among elective and emergency admissions
was marginally higher than urgent admissions, but neither
hospitalization for elective or emergency reasons was
an independent predictor when urgent admission was
used as the reference standard. Emergency admissions
receive aggressive treatment and higher acuity of care
once admitted in comparison to those admitted electively.
Without access to individual patient data, we were not able
to examine clinical characteristics that might be related to
the type of admission.
Our study has several limitations. First, only non-federal
hospitals were included in the National Hospital Discharge Survey database; thus, generalizability to Veterans Affairs
medical centers and other institutions should be done with
caution. Second, the NHDS database included readmissions
for acute pancreatitis; thus, the unit of analysis for the study
was events of AP and not independent patients with AP.
Finally, the NHDS data did not include lab values, treatment
choices, or longitudinal follow-up information; thus, the
impact of clinical characteristics could not be examined.
CONCLUSION
Our analysis of National Hospital Discharge Survey
data shows that demographic factors (sex and age),
clinical characteristics (comorbidities, length of stay),
and features of the health care system (geographic
location, hospital size) may be utilized as predictors
of in-patient mortality for those diagnosed with acute
pancreatitis. Future research may identify other
predictors of mortality that would improve the scoring
systems now used with acute pancreatitis patients.
As more research is conducted, a more accurate, less
cumbersome, and easily calculated scoring system may
be developed aiding in the reduction of in-hospital
mortality in patients with acute pancreatitis.
Conflict of Interest
We declare that we have no conflict of interests.
References
- Vege SS, Yadav D, Chari ST. Pancreatitis. In: GI Epidemiology, 1st ed, Talley NJ, Locke GR, Saito YA (Eds), Blackwell Publishing, Malden, MA 2007.
- Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, et al. "Burden of Gastrointestinal Disease in the United States: 2012 Update.Gastroenterology 2012; 143: 1179-87.e1-3. [PMID: 22885331]
- Fagenholz PJ, Castillo CF, Harris NS, Pelletier AJ, Camargo CA Jr. "Increasing United States Hospital Admissions for Acute Pancreatitis, 1988–2003. Ann Epidemiol 2007; 17:491-7. [PMID: 17448682]
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA Evidence-based Guidelines for the Management of Acute Pancreatitis. Pancreatology 2013; 13:e1-15. [PMID: 24054878]
- Banks PA, Freeman ML; Practice Parameters Committee of the American College of Gastroenterology. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379-400.[PMID: 17032204]
- Mounzer R, Langmead CJ, Wu BU, Evans AC, Bishehsari F, Muddana V, et al. Comparison of Existing Clinical Scoring Systems to Predict Persistent Organ Failure in Patients With Acute Pancreatitis.Gastroenterology 2012; 142:1476-482. [PMID: 22425589]
- Wang X1, Xu Y, Qiao Y, Pang X, Hong L, Fu J, et al. An Evidence-Based Proposal for Predicting Organ Failure in Severe Acute Pancreatitis. Pancreas 2013; 42:1255-261. [PMID: 24152952]
- De Bernardinis M, Violi V, Roncoroni L, Boselli AS, Giunta A, Peracchia A. Discriminant Power and Information Content of Ranson's Prognostic Signs in Acute Pancreatitis: A Meta-analytic Study.Crit Care Med 1999; 27:2272-83. [PMID: 10548220]
- Larvin M. Assessment of clinical severity and prognosis. In: The Pancreas, Beger HG, Warshaw AL, Buchler MW, et al (Eds), Blackwell Science, Oxford 1998. p.489.
- Papachristou GI, Muddana V, Yadav D, O'Connell M, Sanders MK, Slivka A, et al. Comparison of BISAP, Ranson's, APACHE-II, and CTSI Scores in Predicting Organ Failure, Complications, and Mortality in Acute Pancreatitis. Am J Gastroenterol 2010; 105:435-41. [PMID: 19861954]
- Wu BU, Johannes RS, Sun X, Conwell DL, Banks PA. Early Changes in Blood Urea Nitrogen Predict Mortality in Acute Pancreatitis. Gastroenterology 2009; 137:129-35. [PMID: 19344722]
- Mofidi R, Duff MD, Wigmore SJ, Madhavan KK, Garden OJ, Parks RW. Association between Early Systemic Inflammatory Response, Severity of Multiorgan Dysfunction and Death in Acute Pancreatitis. Br J Surg 2006; 93:738-44. [PMID: 16671062]
- Premkumar R, Phillips AR, Petrov MS, Windsor JA. The clinical relevance of obesity in acute pancreatitis: targeted systematic reviews.Pancreatology 2015;15:25-33. [PMID: 25464938]
- Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute Pancreatitis: Value of CT in Establishing Prognosis. Radiology 1990; 174:331-36. [PMID: 2296641]
- Singh VK, Bollen TL, Wu BU, Repas K, Maurer R, Yu S, et al. An assessment of the severity of interstitial pancreatitis. Clin Gastroenterol Hepatol 2011;9:1098-1103. [PMID: 21893128]
- Frey C, Zhou H, Harvey D, White RH. Co-morbidity is a strong predictor of early death and multi-organ system failure among patients with acute pancreatitis. J Gastrointest Surg 2007;11:733-742. [PMID: 17417710]
- Murata A, Ohtani M, Muramatsu K, Matsuda S. Influence of comorbidity on outcomes of older patients with acute pancreatitis based on a national administrative database. Hepatobiliary Pancreat Dis Int 2015;14:422-8. [PMID: 26256088]
- Li XY, Wang XB, Liu XF, Li SG. Prevalence and risk factors of organ failure in patients with severe acute pancreatitis. World J Emerg Med 2010;1:201-204. [PMID: 25214968]
- Murata A, Ohtani M, Muramatsu K, Kobori S, Tomioka S, Matsuda S. Impact of obesity on outcomes of paediatric acute pancreatitis based on a national administrative database. Pediatr Obes 2015; 11:174-80. [PMID: 26061540]

