Keywords
Ablation catheter; Refractory hypertension; Impedance; Renal denervation
Abbreviations
RDN: Renal Denervation; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; eGFR: Estimated Glomerular Filtration Rate; ABPM: Ambulatory Blood Pressure Monitoring; RF: Radiofrequency; ACEI: Angiotensin Converting Enzyme Inhibitors; ARB: Angiotensin Receptor Blocker; BMI: Body Mass Index; T2DM: Type 2 Diabetes Mellitus
Introduction
Hypertension is one of the most common cardiovascular diseases and the largest single cause of human death in the world with the adult prevalence rate of approximately 18.8% [1], which significantly increases risks of stroke, myocardial infarction, congestive heart failure and kidney disease [2,3]. There are still a considerable number of patients with uncontrolled blood pressure who have been prescribed sufficient quantities of antihypertensive medications including diuretics [4,5]. Catheterbased renal denervation (RDN) seemed to be a promising technology to treat patients with refractory hypertension, which could lead to a persistent and long-term decline of blood pressure without significant side effects, but this effect has still been controversial, and the ablation catheters used in the procedure have also been argued. It’s believed that newer special catheters would be used for RDN in the future, but there are hardly reports concerning the application of standard radiofrequency catheters in RDN, especially in Chinese population. This prospective unrandomized controlled study was aimed to determine antihypertensive efficacy and safety of RDN with standard radiofrequency catheters in Chinese patients with refractory hypertension, and to explore the predictive factors correlated to the antihypertensive effect.
Methods
Study design
It was designed as a prospective, comparative unrandomized study aimed to determine the efficacy and safety of renal denervation with standard ablation catheter in Chinese population and to evaluate the factors related to the effectiveness. Patients with refractory hypertension aged from 18 to 80 underwent renal denervation or drug therapy, and were followed up for 3 months. This study was approved in China by the Ethics Committee of the Third Xiangya Hospital, Central South University, and all patients provided written informed consent.
Study population
A total of 60 patients of refractory hypertension were enrolled in the Third Xiangya Hospital, Central South University, from October 2011 to February 2015. All of them had an office systolic blood pressure of 160 mmHg or higher (150 mmHg or higher in patients with type-2 diabetes) in spite of improving lifestyles and taking three or more kinds of antihypertensive drugs, including a diuretic, in maximum tolerated doses. The participants would be excluded if they were diagnosed as secondary hypertension, type-1 diabetes or kidney diseases with glomerular filtration rate lower than 45 mL/min/1.73 m2 or had anatomical abnormalities or stenosis of renal arteries. All patients were evaluated previously by initial screening and were prescribed maximum tolerated doses of antihypertensive drugs with a diuretic included and they were required to maintain their baseline medications unchanged for at least 8 weeks before RDN procedure. Renal artery imaging with computed tomography was performed for all of them, eight of whom were excluded due to stenosis or anatomical abnormalities of renal arteries. Forty-two patients received catheter-based renal denervation and the other ten did not undergo this procedure as controls who were required to keep the baseline medications unchanged until at 3-month follow-up.
Blood pressure measurement and examinations
Office sitting blood pressure was measured for three times with an interval of one minute on both arms of the patients after resting for at least 15 minutes with validated devices (Omron HEM-7201) and would be recorded as the calculated average value at baseline and during the whole follow-up period. 24- hour ambulatory blood pressure monitoring (ABPM) was also performed at baseline and at 3-month follow-up with validated devices (Spacelabs 90217 Ambulatory Blood Pressure monitors). However, 6 among 52 patients could not tolerate it and failed to accomplish the baseline ABPM owing to sleep disturbances and only 36 of them had valid ABPM data at 3-month follow-up.
Routine blood tests were performed at baseline and at 3-month follow-up such as complete blood count, serum electrolyte analysis and liver function etc. A chemiluminescence immunoassay was developed to test serum creatinine. Estimated glomerular filtration rate (eGFR) was obtained by Cockcroft- Gault equation via creatinine clearance. All participants underwent other examinations such as electrocardiogram, echocardiography, urinary ultrasonography and 64-slice spiral computed tomography angiography of renal arteries, and the ones who underwent RDN procedure would re-take renal artery imaging with computed tomography at 3-month follow-up.
Catheter-based renal denervation procedure
The patient had his right or left femoral artery catheterized with an 8F arterial sheath in a supine position, then a 5F JR4 angiography catheter was introduced into the bilateral renal artery openings successively to conduct bilateral renal artery angiography. After that, the angiography catheter was retreated and an 8F RDC guiding catheter (Cordis) was inserted into the abdominal aorta. Next, the head-end of a 5F standard radiofrequency (RF) catheter (Irvine Biomedical Inc.) was placed to the distal renal artery through the guiding catheter in order to conduct rotated ablations at four different points in each renal artery with RF energy of 8~10 Watts (Figures 1a-1f) for at least 2 minutes at each ablation point. During the ablation process, renal angiography was simultaneously performed if needed, temperature and impedance at the catheter tip were monitored on the radiofrequency ablation generator (Irvine Biomedical Inc. 1500T) and values of those variables were recorded at different time points. The average impedance changes of both sides were marked as ΔL and ΔR, respectively. Patients were premeditated with morphine or fentanyl, and heparin was administrated for anticoagulation [6].
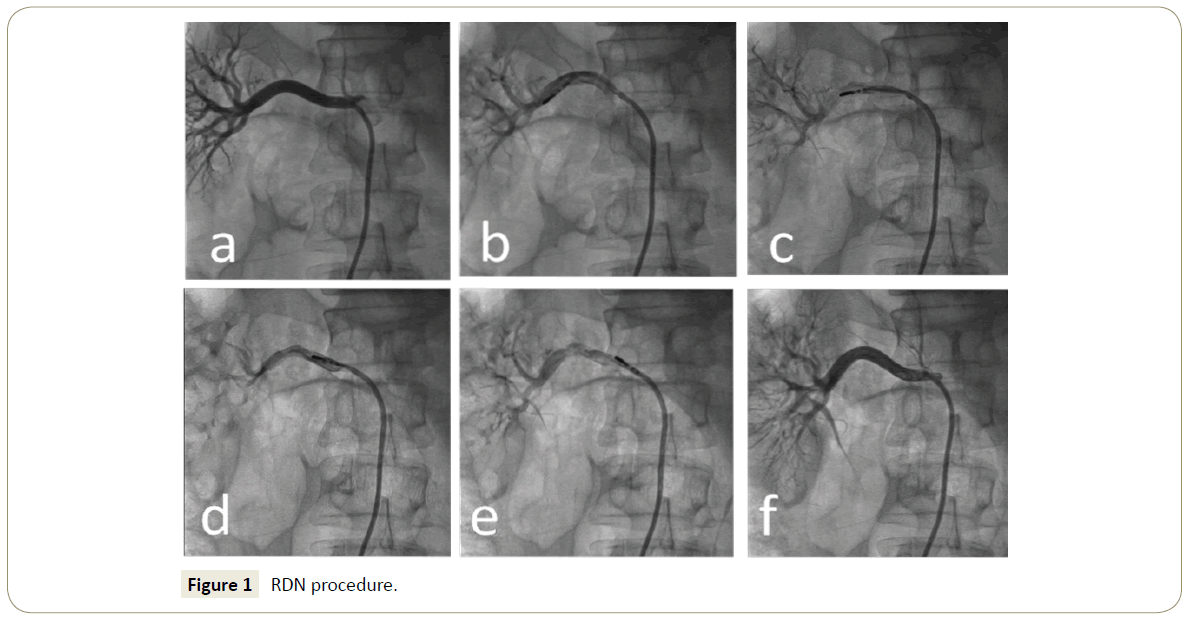
Figure 1: RDN procedure.
Statistical analysis
Quantitative data were presented as mean ± standard deviation. Paired t-test was used to test differences from baseline to the 3-month follow-up assessment. Differences between groups were tested in the use of independent-samples t-test. Discrete variables were compared with a chi-squared analysis. Multiple linear model was performed to test the correlation of predictive factors with blood pressure reduction. All data were normally distributed. A P value of less than 0.05 was considered statistically significant. All statistical analyses were performed in the use of SPSS software version 20.0.
Results
Baseline clinical characteristics
Those patients in RDN group had an average age of 55.0 ± 12.6 years, and 35.7% of them were diagnosed as type 2 diabetes mellitus. The BMI was 25.4 ± 3.3 kg/m2, and the eGFR or creatinine clearance rate 92.2 ± 36.3 mL/min. They had a mean SBP of 166.5 ± 12.6 mmHg and DBP of 99.8 ± 12.2 mmHg, even though they had taken 3.8 ± 1.0 kinds of anti-hypertensive drugs on average, which included ACEI/ARB (73.8%), β-blockers (52.4%), calcium channel blockers (85.7%), diuretics (100%), α-blockers (21.4%) or spironolactone (42.9%). Similarly, the average age of control patients was 56.7 ± 10.3 years, and 20% of them had type 2 diabetes mellitus. Their average BMI was 26.2 ± 2.4 kg/m2, and eGFR 86.4 ± 27.8 mL/min. They had taken 4.3 ± 1.2 types of antihypertensive drugs; their mean SBP and DBP were 170.4 ± 17.8 mmHg, 102.5 ± 16.2 mmHg, respectively.
There were no statistically significant differences of those parameters between two groups (P>0.05). Baseline clinical characteristics of all the patients were listed in Table 1.
| Parameters |
RDN group (n=42) |
Control group (n=10) |
P |
| Sex (male/female) |
19/23 |
3/7 |
0.488 |
| Age (years) |
55.0 ± 12.6 |
56.7 ± 10.3 |
0.698 |
| T2DM |
15 (35.7%) |
2 (20.0%) |
0.467 |
| BMI (kg/m2) |
25.4 ± 3.3 |
26.2 ± 2.4 |
0.481 |
| eGFR (mL/min) |
92.2 ± 36.3 |
86.4 ± 27.8 |
0.643 |
| Mean SBP (mmHg) |
166.5 ± 12.6 |
170.4 ± 17.8 |
0.415 |
| Mean DBP (mmHg) |
99.8 ± 12.2 |
102.5 ± 16.2 |
0.551 |
| Types of anti-hypertensive drugs |
3.8 ± 1.0 |
4.3 ± 1.2 |
0.155 |
| ACEI/ARBs |
31 (73.8%) |
10 (100%) |
0.096 |
| β-blockers |
22 (52.4%) |
3 (30.0%) |
0.296 |
| Calcium channel blockers |
36 (85.7%) |
10 (100%) |
0.582 |
| Diuretics |
42 (100%) |
10 (100%) |
- |
| α-blockers |
9 (21.4%) |
4 (40.0%) |
0.244 |
| Spironolactone |
18 (42.9%) |
6 (60.0%) |
0.483 |
Table 1: Baseline clinical characteristics of RDN-treated patients (RDN group) and controls (control group).
Effects of RDN with standard ablation catheters
Figure 2A showed the mean SBP changes in two groups. The mean SBP was significantly decreased to 153.0 ± 16.8 mmHg from 166.5 ± 12.6 mmHg at baseline in 3 months after RDN (P0.001), while the mean SBP of control patients remained nearly unchanged from 170.4 ± 17.8 mmHg at baseline to 169.5 ± 20.2 mmHg (P=0.692). The patients in RDN group had a significantly lower mean SBP at 3-month follow-up compared to controls (P=0.010).
Similarly, the patients who had undergone bilateral RDN had their mean DBP reduced significantly from 99.8 ± 12.2 mmHg to 90.5 ± 11.5 mmHg in 3 months after RDN (P=0.001). No significant DBP drop was observed in controls (102.5 ± 16.2 VS 97.2 ± 9.4 mmHg, P=0.109). The patients in RDN group had a tendency to have a lower mean DBP than controls, but the differences were not significant (P=0.093). The changes of mean DBP were illustrated in Figure 2B.

Figure 2: A and 2B Distribution of Infarct related artery in study population.
Safety of RDN with standard ablation catheters
No severe cardiovascular events happened to any individual during or after the RDN procedure. None of the patients had dissection or stenosis of renal arteries, which was confirmed by spiral computed tomography angiography of renal arteries. Hematoma of femoral artery was observed in three participants after RDN procedure but not exacerbated when compression bandage was applied and totally vanished without any sequela as showed by re-examination one month later. Two patients suffered from vomiting frequently, which was assumed to be associated with fentanyl, and finally the symptoms disappeared after symptomatic treatment.
Predictive factors for blood pressure reduction
We performed a multiple linear model to explore the associations between blood pressure induction and factors which were entered including age, sex, BMI, type 2 diabetes mellitus, eGFR, number of anti-hypertensive drugs taken, impedance changes of both sides by an enter method. The percentage of variation of SBP and DBP changes (adjusted R-squared) was described as 60.3% and 46.7%, respectively (Tables 2A and 2B).
| Factors |
Unstandardized coefficients |
Standardized Beta |
P |
| Beta |
Std. error |
| (Constant) |
11.880 |
20.025 |
-- |
0.557 |
| Sex |
-9.222 |
3.068 |
-0.310 |
0.005 |
| Age |
0.059 |
0.174 |
0.049 |
0.738 |
| BMI |
-0.351 |
0.470 |
-0.078 |
0.459 |
| T2DM |
-3.485 |
3.219 |
-0.113 |
0.287 |
| eGFR |
0.079 |
0.058 |
0.192 |
0.186 |
| Number of drugs taken |
0.480 |
1.559 |
0.031 |
0.760 |
| Impedance change (ΔL) |
0.202 |
0.094 |
0.276 |
0.040 |
| Impedance change (ΔR) |
0.509 |
0.124 |
0.590 |
0.000 |
Table 2A: Relationship between impedance reduction and blood pressure reduction of hypertensive patients in RDN group (x ± S) A. Multiple linear regression analysis for association between SBP change and factors sex was negatively correlated to change of SBP, while impedance change (ΔL) and impedance change (ΔR) were positively correlated to change of SBP.
| Factors |
Unstandardized coefficients |
Standardized beta |
P |
| Beta |
Std. error |
| (Constant) |
29.004 |
16.747 |
-- |
0.093 |
| Sex |
-5.197 |
2.566 |
-0.243 |
0.051 |
| Age |
-0.023 |
0.145 |
-0.027 |
0.875 |
| BMI |
-1.033 |
0.393 |
-0.319 |
0.013 |
| T2DM |
-3.640 |
2.692 |
-0.164 |
0.186 |
| eGFR |
0.103 |
0.049 |
0.347 |
0.043 |
| Number of drugs taken |
0.324 |
1.304 |
0.029 |
0.806 |
| Impedance change (ΔL) |
0.178 |
0.079 |
0.336 |
0.031 |
| Impedance change (ΔR) |
0.168 |
0.104 |
0.270 |
0.115 |
Table 2B: Multiple linear regression analysis for association between DBP change and factors BMI was negatively correlated to change of DBP, while eGFR and impedance change (ΔL) were positively correlated to change of DBP.
As Table 2A showed, multiple linear regression analysis revealed the highly positive correlation of impedance reduction with decrease of SBP, and impedance changes of ablation catheter in bilateral renal artery were both statistically correlated to SBP reduction (P=0.05).
In addition, sex was also related to SBP change and female patients could reach a significantly better efficiency of RDN in reducing SBP (P=0.005). No correlations were found of age, BMI, T2DM, eGFR or number of anti-hypertensive drugs taken with SBP change (P=0.05).
Impedance change of ablation catheter in left renal artery was also correlated to DBP reduction (P=0.031), and similar tendency was observed in the right renal artery but there was no significant correlation of it (P=0.115). Gender was almost related to DBP change (P=0.051). It’s interesting that BMI and eGFR were both found to be correlated to reduction of DBP as Table 2B illustrated (P=0.05).
Discussion
Discussion A large amount of clinical trials and animal studies has proved that the sympathetic nervous system plays an important role in the pathophysiology of hypertension. Abnormality of sympathetic activity is not only an initiating factor of hypertension, but also acts in maintaining high blood pressure, especially in the pathogenesis of refractory hypertension. Excessive sympathetic activation has even been a treatment target for hypertension and many other cardiovascular diseases [7]. Early studies concerning the effects of excessive adrenaline on hypertension revealed that the concentration of norepinephrine spilled out of kidneys or overall body were significantly increased in hypertensives [8,9]. Recent studies have found that destroy can be achieved of afferent and efferent fibres of renal sympathetic nerves by RDN procedure, so that it could constrict the activation of renal sympathetic nerves, cut down the concentration of systemic norepinephrine and blood pressure [10]. In addition, the central sympathetic efferent activity could even be significantly decreased by RDN procedure [11]. Therefore, RDN provides one more choice for those patients with refractory hypertension who are treated with medications only but cannot achieve target blood pressures [12]. In a metaanalysis of 61 prospective studies, Lewington S. and colleagues showed us that an increase of 20/10 mmHg in blood pressure resulted in double cardiovascular death rate. It is indicative that RDN procedure would provide meaningful benefits by reducing blood pressure for those patients who had already presented blood pressure drop but the blood pressure was still above the target value. Although there were unexpected contrasts sharply with the results of Symplicity HTN-1 and HTN-2 trials [13-15], Symplicity HTN-3 trial had stimulated interests in exploring the mystery of RDN.
There might be various potential factors contributing to the negative results of Symplicity HTN-3 trial [16], in which methodology taken in that trial was arguable, as the ablation catheter sponsored by Medtronic was a kind of single-tip one which might only produce lesions of no more than 3 mm in diameter or depth. Therefore, incomplete denervation would not bring along significant decrease of blood pressure. We used standard radiofrequency ablation catheters in our studies. The material quality and methodology of these catheters are nearly the same as those used in Symplicity HTN-3 trial, but the electrode length of a standard RF catheter is 4 mm, and it might enlarge the contact area and conduct complete ablation of renal sympathetic fibres. The effectiveness of standard radiofrequency ablation catheter in RDN have been reported in a few studies [17,18], but related data are seldom available for Chinese people. Similar to previous studies, our findings again confirmed the validity of RDN treatment in patients with refractory hypertension. The office means SBP dropped significantly after RDN procedure, and the mean DBP also tended to decrease, though the change of DBP was not statistically significant. These results reinforced the potential benefit of RDN. Moreover, reduction of blood pressure could be attained in Chinese population by RDN treatment with standard radiofrequency catheters in addition to some special RDN catheters.
Standard radiofrequency ablation catheter could be more efficient in complete denervation and reducing blood pressure, but it was probably presumed to produce more severe complications simultaneously. During the 3-month follow-up, some events were observed in our study, but those side effects seemed to be procedure-related complications or associated to adverse drug reactions. We don’t think standard radiofrequency ablation catheters will increase the risks of RDN, although we failed to obtain some new-born ablation catheters to make one-to-one comparisons. What’s more, no macroscopic vascular lesions were detected in those patients undergoing RDN procedure with standard ablation catheters. Although slight damages of vascular endothelial cells could be spotted in animal studies after RDN procedure, no delayed stenosis was ever discovered due to rapid endothelialisation process of renal artery [19].
Whatever methodology is applied in RDN procedure, there has still been a difficult situation that we have no simple and useful evaluation strategy to predict and determine the effectiveness of RDN. In other words, we never know whether it will be useful even when we have finished the RDN procedure. Therefore, we intended to pursue the related factors possibly affecting the effectiveness of RDN in our study. Tissue heating can be affected by a variety of factors, such as blood flow velocity and volume, catheter contact area, contact pressure, and power output. Among these factors, blood flow velocity and volume are uncontrollable. Taking into account the safety concern of increasing power output, a modest increase in catheter contact area and contact pressure is more alterable. Standard ablation catheter with 4 mm head end used in our study was supposed to make larger contact area as previously referred and in the use of it, good catheter contact could result in effective tissue heating and durable ablation lesions. Early study revealed the relationship between the initial impedance change and tissue heating, and indicated that an initial fall in impedance beyond 10 ohms would predict interruption of accessory pathways’ conduction [20]. Until now, impedance decrease has even been an indicator of good catheter contact as evidenced by force sensing catheterization technique [21]. Our study results showed the correlation between impedance fall and reduction of blood pressure. It meant that complete denervation would make blood pressure decrease as the impedance fell and impedance change could be a predictive factor for the effectiveness of RDN. However, greater fall of impedance would not always be better. Impedance decrements of more than 10 ohms were even considered to increase the risk of excessive tissue and coagulum formation in another study [22]. We supposed that excessive decrements of impedance would probably increase risks of vascular complications.
Not only impedance change but gender was found to be correlated with blood pressure response as well. It seemed to be easier for female patients to have blood pressure reduced after RDN procedure than male ones, which might be attributed to greater inhibition of sympathetic nerve activity in females. With a greater baroreflex sensitivity, women could have alterations more efficiently in blood pressure than men [23]. BMI was negatively correlated to reduction of DBP as the results in our study showed and the patients with lower BMI would respond better to RDN treatment. This situation was not unexpected. There were close connections between metabolic syndrome and insufficient control of blood pressure, and hypertensive patients with metabolic syndrome had higher risk of uncontrolled blood pressure in spite of the use of increased number of medications [24,25]. eGFR was also reasonably associated with the reduction of DBP as Chinese adults might be vulnerable to renal function decline with elevated blood pressure while lower eGFR would decrease kidney’s ability to remove salt and make the patients be refractory to anti-hypertensive treatment [26,27].
Study Limitations
Although the results of our study can effectively reflect the efficacy and safety of the RSD procedure with standard radiofrequency catheters, there are still some limitations. At first, we have only managed to enrol a limited number of patients and follow them up for only three months. We need make further researches by large multi-cantered randomized clinical trials with long-term follow-up periods in the future. Secondly, we failed to collect full data of 24-hour ambulatory blood pressure monitoring for all the patients, as there was accumulative evidence to demonstrate that ABPM played a major role in decision-making in the management of hypertension [28,29]. Finally, the investigators who followed up the patients were not blind to the treatment, and it’s impossible to avoid bias.
Conclusion
In conclusion, reduction of blood pressure could be safely achieved by RDN treatment with standard radiofrequency catheters in Chinese population, and the effectiveness is closely associated with impedance change of ablation catheter. Sex, BMI and eGFR might be predictive factors for its validity as well.
Funding
This study was funded by the Key Science and Technology Project of the Science and Technology Department of Hunan Province (2012WK2002). The authors have no conflicts of interest to declare.
References
- Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJ, et al. (2002) Selected major risk factors and global and regional burden of disease. Lancet 360: 1347-1360.
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, et al. (2005) Global burden of hypertension: Analysis of worldwide data. Lancet 365: 217-223.
- Dzau VJ, Antman EM, Black HR, Hayes DL, Manson JE, et al. (2006) The cardiovascular disease continuum validated: Clinical evidence of improved patient outcomes: part I: Pathophysiology and clinical trial evidence (risk factors through stable coronary artery disease). Circulation 114: 2850-2870.
- Sarafidis PA, Bakris GL (2008) Resistant hypertension: An overview of evaluation and treatment. J Am Coll Cardiol 52: 1749-1757.
- Calhoun DA, Jones D, Textor S, Goff DC, Murphy TP, et al. (2008) Resistant hypertension: Diagnosis, evaluation, and treatment: a scientific statement from the American Heart Association Professional Education Committee of the Council for High Blood Pressure Research. Circulation 117: e510-526.
- Zhang ZH, Yang K, Jiang FL, Zeng LX, Jiang WH, et al. (2014) The effects of catheter-based radiofrequency renal denervation on renal function and renal artery structure in patients with resistant hypertension. J Clin Hypertens 16: 599-605.
- Sobotka PA, Mahfoud F, Schlaich MP, Hoppe UC, Böhm M, et al. (2011) Sympatho-renal axis in chronic disease. Clinical research in cardiology: official journal of the German Cardiac Society 100: 1049-1057.
- Esler M, Jennings G, Korner P, Willett I, Dudley F, et al. (1988) Assessment of human sympathetic nervous system activity from measurements of norepinephrine turnover. Hypertension 11: 3-20.
- Schlaich MP, Lambert E, Kaye DM, Krozowski Z, Campbell DJ, et al. (2004) Sympathetic augmentation in hypertension: Role of nerve firing, norepinephrine reuptake, and Angiotensin neuromodulation. Hypertension 43: 169-175.
- Schlaich MP, Sobotka PA, Krum H (2009) Renal sympathetic-nerve ablation for uncontrolled hypertension. New Eng J Med. 361: 932-934.
- Hering D, Lambert EA, Marusic P, Walton AS, Krum H, et al. (2013) Substantial reduction in single sympathetic nerve firing after renal denervation in patients with resistant hypertension. Hypertension 61: 457-464.
- Ewen S, Ukena C, Bohm M, Mahfoud F (2013) Percutaneous renal denervation: new treatment option for resistant hypertension and more? Heart (British Cardiac Society) 99: 1129-1134.
- Krum H, Schlaich M, Whitbourn R, Sobotka PA, Sadowski J, et al. (2009) Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet 373: 1275-1281.
- Esler MD, Krum H, Sobotka PA, Schlaich MP, Schmieder RE, et al. (2010) Renal sympathetic denervation in patients with treatment-resistant hypertension (The Symplicity HTN-2 Trial): A randomised controlled trial. Lancet 376: 1903-1909.
- Krum H, Schlaich MP, Sobotka PA, Böhm M, Mahfoud F, et al. (2014) Percutaneous renal denervation in patients with treatment-resistant hypertension: Final 3-year report of the Symplicity HTN-1 study. Lancet 383: 622-629.
- Bhatt DL, Kandzari DE, O'Neill WW, D'Agostino R, Flack JM, et al. (2014) A controlled trial of renal denervation for resistant hypertension. N Engl J Med 370: 1393-401.
- Prochnau D, Figulla HR, Surber R (2012) Efficacy of renal denervation with a standard EP catheter in the 24-h ambulatory blood pressure monitoring-long-term follow-up. Int J Cardiol 157: 447-448.
- Amitabh Y, Sanjib P, Sanjeev G (2014) Renal denervation using standard 5F radiofrequency ablation catheter in patients with end stage renal disease: A 6 month follow-up. JACC: Cardio Inte 7: S3-S4.
- Rippy MK, Zarins D, Barman NC (2011) Catheter-based renal sympathetic denervation: chronic preclinical evidence for renal artery safety. Clinical research in cardiology : official journal of the German Cardiac Society 100: 1095-1101.
- Harvey M, Kim YN, Sousa J, el-Atassi R, Morady F, et al. (1992) Impedance monitoring during radiofrequency catheter ablation in humans. Pacing Clin Electrophysiol 15: 22-27.
- Reichlin T, Knecht S, Lane C, Kühne M, Nof E, et al. (2014) Initial impedance decrease as an indicator of good catheter contact: insights from radiofrequency ablation with force sensing catheters. Heart Rhythm 11: 194-201.
- Strickberger SA, Ravi S, Daoud E, Niebauer M, Man KC, et al. (1995) Relation between impedance and temperature during radiofrequency ablation of accessory pathways. Am Heart J 130: 1026-30.
- Hinojosa LC, Chapa I, Lange D, Haywood JR (1999) Gender differences in sympathetic nervous system regulation. Clin Exp Pharmacol Physiol 26: 122-126.
- Arcucci OG, de Simone G, Izzo R, Rozza F, Chinali M, et al. (2007) Association of suboptimal blood pressure control with body size and metabolic abnormalities. J Hypertens 25: 2296-2300.
- De Marco M, Simone G, Izzo R, Mancusi C, Sforza A, et al. (2012) Classes of antihypertensive medications and blood pressure control in relation to metabolic risk factors. J Hypertens 30: 188-193.
- Judd E, Calhoun DA (2015) Management of hypertension in CKD: beyond the guidelines. Adv Chronic Kidney Dis 22: 116-122.
- Wang Q, Xie D, Xu X, Qin X, Tang G, et al. (2015) Blood pressure and renal function decline: A 7-year prospective cohort study in middle-aged rural Chinese men and women. J Hypertens 33: 136-143.
- White WB, Gulati V (2015) Managing hypertension with ambulatory blood pressure monitoring. Curr Cardiol Rep 17: 2.
- Solak Y, Kario K, Covic A, Bertelsen N, Afsar B, et al. (2016) Clinical value of ambulatory blood pressure: Is it time to recommend for all patients with hypertension? Clin Exp Nephrol 20: 14-22.

