Keywords
Evidence-Based Practice; Pancreatitis, Acute Necrotizing
Abbreviations
ASA American Society of Anesthesiologists physical status; BMI body mass index; CCI Charlson Comorbidity Index; HPB hepatopancreatobiliary; ICU intensive care unit; IQR interquartile range; MSU modified step-up approach; SD standard deviation; SIR systemic inflammatory response; VARD video-assisted retroperitoneal debridement
INTRODUCTION
Acute pancreatitis is responsible for over 270,000 hospital admissions in the United States per year, and up to 20% develop necrotizing pancreatitis [1]. One-third of these are further complicated by infection, mandating invasive interventions in up to 95% of patients [2]. Infected necrotizing pancreatitis has historically been treated with an open necrosectomy, however, high rates of morbidity and mortality up to 95% and 39%, respectively, have prompted efforts to develop minimally-invasive techniques [3, 4, 5, 6, 7].
The management of infected pancreatic necrosis has evolved significantly over the past two decades, from CT-guided percutaneous catheters [8], fluoroscopyguided fragmentation and extraction [9], to endoscopic necrosectomy using transgastric or transduodenal catheters [10]. In 1996, Gagner et al. described minimally invasive surgical approaches including transgastric, retrogastric retrocolic and retroperitoneal techniques [11] and since then, multiple minimally-invasive techniques have been developed that utilize retroperitoneal access [12, 13, 14], including the video assisted retroperitoneal debridement (VARD) [15]. Today, optimal treatment remains debated, but recommended algorithms often combine multi-modality interventions [16, 17]. This paradigm shift was tested in the prospective randomized, controlled PANTER trial by van Santvoort et al. in 2010 comparing open necrosectomy to the “Step-Up Approach,” [18] which found that one-third of patients were spared an operation, with equal rates of mortality and lower complications. However, controlled trials on multi-modal interventions require abundant resources along with narrow expertise, and do little to inform implementation practices in typical settings for an otherwise rare disease.
The difficulty in applying evidence-based recommendations based on sound clinical trials has been well described [19]. It is estimated to take 17 years for research evidence to reach clinical practice [20], and an even longer gap before effecting health policy [21, 22]. Four years after the PANTER trial results were published, in a survey of 118 international pancreatologists, only 36% considered the evidence for performing percutaneous catheter drainage as a first intervention as being ‘strong’, and 33% believed the ideal timing for surgical necrosectomy for infected necrotizing pancreatitis was as early as possible after diagnosis [2]. Unfortunately, the translation gap exists across the medical-surgical spectrum; experts found a lag time of 6 to 13 years between publication of guidelines and widespread adoption for a variety of diseases [23, 24].
Despite numerous studies proving effectiveness of the Step-Up approach, there have no studies assessing efficacy and the realistic implementation of these guidelines in a pragmatic setting. Therefore, the goal of this study is to evaluate the practical adoption of the Step-Up approach in a tertiary care setting. We hypothesized that at an academic, high-volume, tertiary care institution, adherence to the Step-Up approach would increase dramatically over a short time period, resulting in fewer operations and improved outcomes.
METHODS
This is a retrospective observational study of a single academic tertiary-care institution between 2006 and 2014 and data were extracted from the electronic and paper medical record. Inclusion criteria were all admitted patients with proven or suspected infected pancreatic necrosis based on: 1) clinical presentation including the course and progression of symptoms, physical examination, and/or signs of systemic inflammatory response syndrome (SIRS) and sepsis characterized by fevers, tachycardia, tachypnea, leukocytosis, lactic acidosis, hypotension and organ failure, and 2) imaging evidence of a walled-off pancreatic collection that is air-filled on computed tomography (CT), or positive pancreatic cultures from fine needle aspiration (FNA). Exclusion criteria were patients with necrosis based on imaging, but no signs of infected necrosis, based on the lack of air on CT or negative FNA cultures.
Definition of Time Periods
The Step-Up Approach was published in the PANTER study by van Santvoort et al. for the Dutch Pancreatitis Study Group in the New England Journal of Medicine in April 2010 [18]. Our study population was divided into the era prior to publication between 2006 and 2010 (Pre- PANTER) and following publication between 2011 and 2014 (Post-PANTER) based on the date of admission. There were no system-level policies enforced across these two time periods at our institution. Outcomes during the post- PANTER period is believed to be influenced by the results of the PANTER study and dissemination of evidence.
Definition of the Modified Step-Up Approach
The Modified Step-Up Approach (MSU) is defined by the sequence of interventions for infected necrotizing pancreatitis. A treatment sequence that began with a percutaneous drain was classified as a MSU, including patients who received additional subsequent drains, endoscopic drainage, or any operative debridement. Operative debridement includes open necrosectomy, minimally invasive cyst-gastrostomy, and video-assisted retroperitoneal debridement (VARD). Treatments that excluded an initial drain, and went directly to surgical intervention were deemed non-adherent to MSU. The time interval between presentation and drainage, in between repeat drainages, or time to endoscopic or surgical intervention did not influence the classification of adherence.
This definition differs from the true Step-Up Approach as described in the original 2010 manuscript that culminates only in a VARD, rather than any operative debridement. The modification was applied in light of the very few VARD procedures performed at our institution during this time period. Although our modified definition includes more aggressive surgical interventions, we believe it preserves the decision making process of escalating invasive intervention when necessary, and embodies the ultimate goal of doing the least harm possible. Additionally, since the 2010 publication, several published treatment pathways for infected necrotizing pancreatitis have similarly incorporated recommendations from the PANTER trial along with traditional open surgery when necessary [25, 26, 27].
Long-Term Outcomes
Long-term complications were defined as new diabetes, exocrine insufficiency, hernia, or enterocutaneous fistula as assessed in the most recent clinical encounter. Survival at 2 years was chosen to minimize bias from varying length of follow-up between the two time periods, as 2 years had elapsed at the time of this study since the most recent admission of patients in 2014.
Ethics
This study was approved by the University of Pittsburgh Institutional Review Board (PRO14080151). As a retrospective study, informed consent from individual patients was waived. The study protocol conforms to the ethical guidelines of the “World Medical Association Declaration of Helsinki – Ethical Principles for Medical Research Involving Human Subjects.”
Statistics
Data elements were checked for variability and normal distribution. Normally-distributed data were summarized using means and standard deviations (SD). Not normallydistributed data were summarized using medians and interquartile ranges (IQR). Differences between groups were tested with Student's t-test when the test assumptions were met; otherwise the non-parametric Wilcoxon ranksum test (Mann–Whitney U test) was used. Categorical data were summarized using frequency and percentages. Chisquare or Fisher exact tests, as appropriate, were used to test related differences between categorical data. The main comparison of the study was carried out to test differences between Pre-PANTER and Post-PANTER groups. All statistical tests were of two-sided nature with a P value of <0.05 designated to indicate statistical significance in hypotheses testing. STATA software (StataCorp, Collage Station, TX, USA) was used in conducting the analysis.
RESULTS
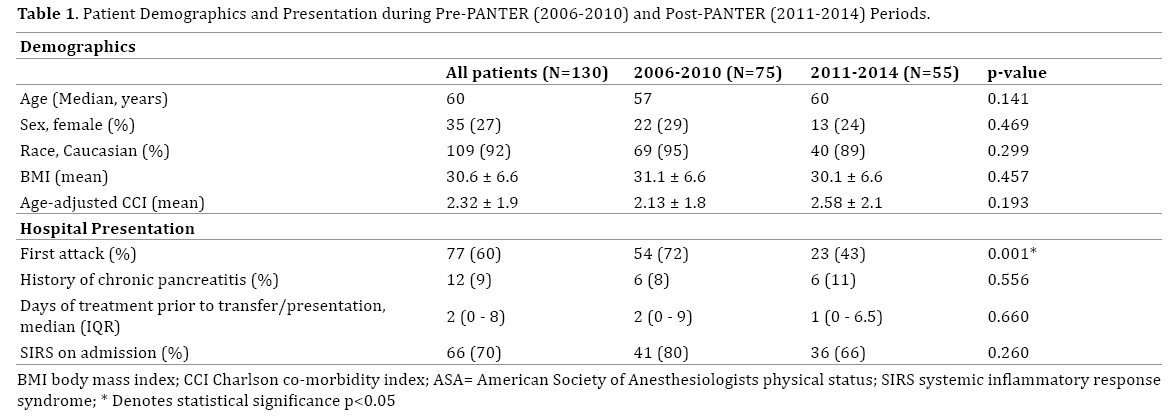
Between 2006 and 2014, 130 patients were admitted with infected necrotizing pancreatitis at the University of Pittsburgh Medical Center; 75 (58%) in the Pre-PANTER period and 55 (42%) in the Post-PANTER period. The median age was 60 years and 73% were males. No difference in patient baseline demographics on admission, including co-morbidities as measured by the Charlson Comorbidity Index (CCI), were observed between the two time periods (Table 1). Additional features of hospital presentation between the two time periods are also shown in Table 1. Patients in the post-PANTER period were less likely to present with their first episode of pancreatitis (43% vs. 72%, p=0.001). Comparable proportions presented with evidence of SIRS.
Adherence to MSU was 27% (n=20) in the early period vs. 46% (n=25) in the late period (p<0.05), with rates of interventions performed listed in Table 2. Using the true definition of the Step-Up algorithm as described by van Santvoort et al. [18] using VARDs, an improvement in adherence rates persisted (4% early vs. 27% late, p<0.0001). Rates of percutaneous drainage increased (43% to 65%, p=0.012) while rates of endoscopic drainage decreased (25% to 9%, p=0.022). The total median number of interventions per patient increased (2 to 3, p=0.0005).
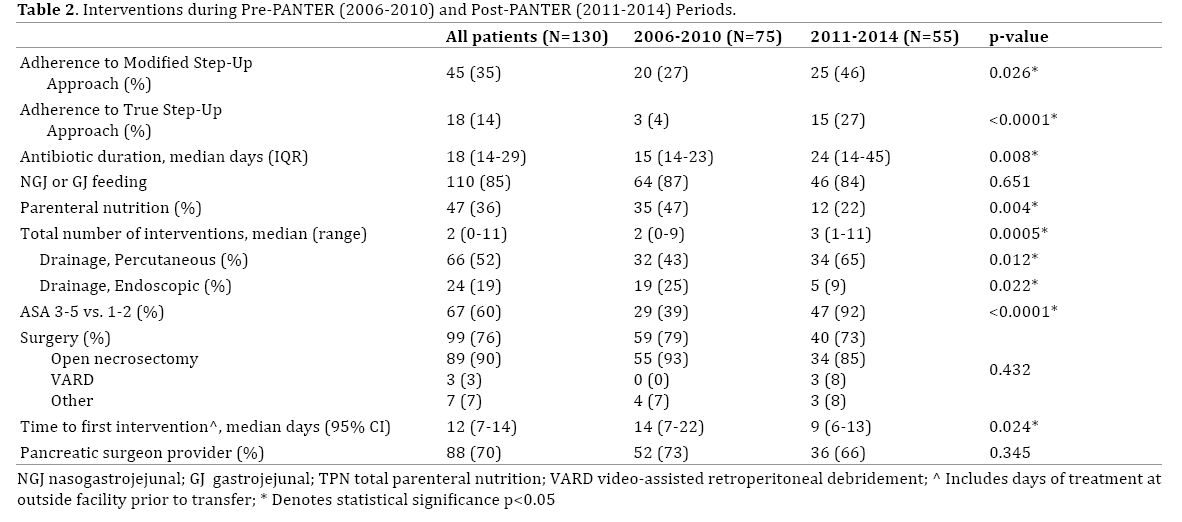
At the time of surgical intervention, patients in the later period had poorer physical status as measured by the American Society of Anesthesiologists physical status classification system (ASA); 92% (n=47) of patients had an ASA status 3-5 in the later period vs. 39% (n=29) in the early period (p<0.0001). Overall rates of surgery remained unchanged between the two time periods (79% early and 73% late, p=0.432), though the rate of open necrosectomy decreased from 93% (N=55) to 85% (N=33) and VARD increased from 0 to 8% (N=3). The median time elapsed between hospital presentation and first intervention (drainage or surgery) decreased from 14 t0 9 days (p=0.024). Rates of nasoenteric feeding was unchanged between the time periods, however, the proportion of patients receiving total parental nutrition (TPN) decreased significantly (47% to 22%, p=0.004). During the early period, 73% (n=52) of patients were cared for by a specialized hepatopancreatobiliary (HPB) surgeon, which was not statistically different from the 66% (n=36) of patients during the late period (p=0.345).
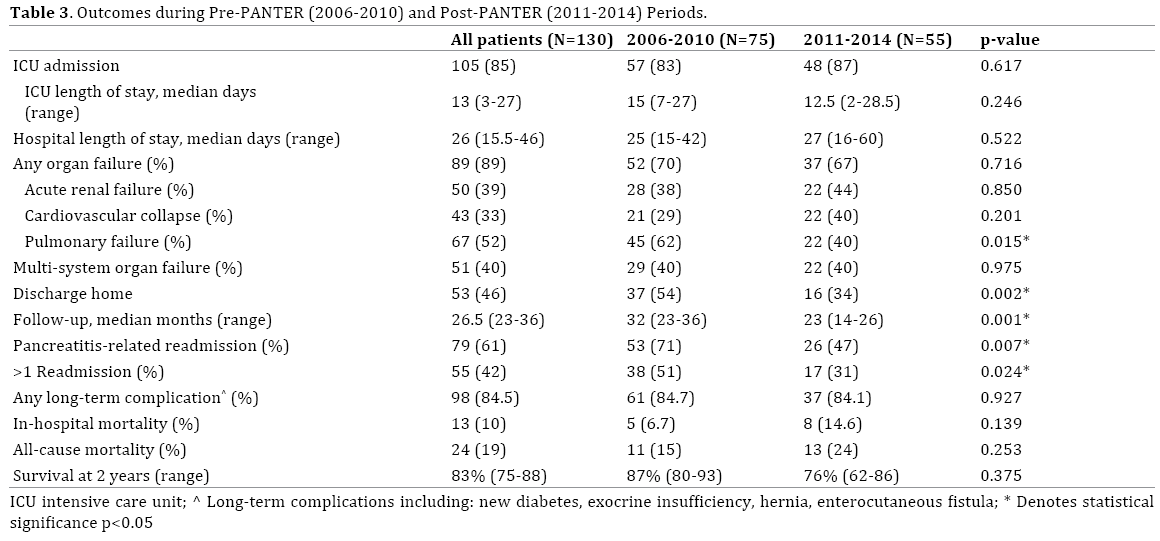
Median follow-up was 26.1 months (95% CI 22.7-30.9) with longer follow-up available for early period patients (32.2 vs. 22.9 months, p=0.001). In-hospital complications along with short and long-term outcomes following admission are displayed in Table 3. Overall, the rate of any organ failure across the two time periods was 89%, with no difference between the two time periods. However, there was a decreased rate of pulmonary failure in the late period. Median total length of hospital stay was 26 days, with no difference between the time periods. There were no differences in in-hospital mortality, all-cause mortality, long-term complications, or survival at 2 years. However, patients in the late period had fewer pancreatitis-related readmissions (47% late vs. 71% early, p=0.007), and were less likely to have multiple readmissions (31% late vs. 51% early, p=0.024). There were no differences in rates of longterm complications between the two study periods (84% late vs. 85% early, p=0.927) which included new diabetes (24%), exocrine insufficiency (27%), hernia (10%), and enterocutaneous fistula (17%). In a sub-analysis of all patients across the two time periods who received MSU vs. surgery first (data not shown), there were no differences in patient demographics, or presenting clinical characteristics to suggest that observed confounders influenced provider decision-making other than Step-Up recommendations.
Discussion
In this study, adherence rates to the MSU approach improved from 27% to 46% between the pre-PANTER and post-PANTER eras, representing an 81% increase based solely on clinical practice shifts, in the absence of instituted protocols. Despite slow and partial adherence, positive early results have been demonstrated with a reduction in pancreatitis-related readmissions and multiple admissions. This is evidence that timely adoption of clinical guidelines is feasible within a short period and can result in improved clinical outcomes. However, a wide translation gap persists, with a compliance rate at a resource-intensive, tertiary care academic center of less than 50 percent.
The early positive outcomes in this study support the adoption of the Step-Up Approach; however, while there was an improvement in adherence rates across time, it is significantly lower than the 87% of surveyed international pancreatologists who report using the Step-Up Approach [2]. Our low rate of VARD procedures (8%) likely reflects multiple components including the varying comfort levels of our institutional surgeons with the technique and familiarity with recently published evidence-based recommendations. Understandably, lack of trained interventional radiologists, gastroenterologists and minimally-invasive surgeons limits implementing interventional-based recommendations. In van Grinsven’s international survey, 98% reported availability of services to perform an open surgical necrosectomy, vs. 80% for minimally-invasive percutaneous necrosectomy, and only 71% for endoscopic transluminal necrosectomy [2]. After five years, our large academic tertiary center was still <50% compliant with MSU, leaving much room for improvement and serves as calling for more providers to change their practice patterns and institutions to monitor internal compliance levels.
In our study, no differences were seen in major complications akin to the PANTER trial. This may be due to the majority of necrosectomies being performed open by surgeons at our institution. The advantages of minimallyinvasive techniques, which often obviate the need for open necrosectomy and lead to improved outcomes, have been well-described, and endorsed by an international multidisciplinary consensus conference [5, 6]. Specifically, our results echo the impressive findings of Sugiomoto et al. who compared results from the PANTER trial and their institutional cohort using early and proactive percutaneous drainage [28]. We report an increase in our percutaneous drainage rates and we believe that use of these drains to provide VARDS access may have led to decreased rates of endoscopic drainage. Additionally, the late period experienced decreased readmission rates, which may reflect a combination of improved adherence, as well as improved intensive care services, and increased experience with peri-procedural care. We believe that lower rates of open necrosectomy and the complications traditionally associated with the morbid operation likely contributed to this observation.
The barriers to applying research evidence in clinical practice are multifold [24]. Firstly, the vast amount of published studies on a given surgical topic is burdensome and all compete for attention in the medical literature [29]. Secondly, ineffective reviews or continuing education programs may fail to update clinicians on new evidencebased practices. Antman et al. found that reviews failed to mention important advances, and treatments shown to be potentially harmful continue to be recommended by clinical experts for myocardial infarctions [23]. Thirdly, there is likely an unwillingness of providers to change current practices. Resistance of interventionalists to change practices that involve learning a new procedure also requires available proctorship, a substantial time commitment and inherent learning curve.
This study has multiple limitations, most notably this represents a retrospective study and given the rare presentation of infected necrosis, the sample size is small which limits the power to detect statistically significant differences between the time periods. As a single institution study, complications or readmissions occurring outside our hospital system were not captured, though likely infrequent given our wide catchment area of 31 hospitals and regional referral patterns. Additionally, improved results in the later period may be reflective of general improvement in medical management of pancreatitis, as reflected in the decrease of patients presenting with infected pancreatic necrosis during their first attack, and not attributable solely to improved Step Up adherence. Finally, the results reflect the experience of a single academic center with capabilities for advanced image-guided and endoscopic drainage procedures and minimally-invasive surgery and is therefore unlikely to represent the practice patterns of most non-tertiary care institutions.
CONCLUSION
In conclusion, timely adoption of evidence-based clinical guidelines can maximize the number of patients who receive optimal treatment and produce early improved clinical outcomes, as evidenced through this pragmatic assessment of translation of the Step-Up approach into practice. Institution-specific barriers to implementation of the Step-Up approach for infected pancreatic necrosis should be identified to improve adherence rates. Institutions should develop internal consensus-derived clinical pathways based on evidencebased guidelines and available local expertise for training, and monitor compliance as a measure of quality with continuous scrutiny of outcomes. Standardized multidisciplinary algorithms developed by specialized surgeons, gastroenterologists, radiologists, and intensivists may be beneficial for streamlining team-based approaches. By identifying and addressing barriers and facilitators of applying evidence-based recommendations, institutions can increase the speed of uptake and improve outcomes for challenging and morbid conditions.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-forprofit sectors. MEH received funding from the Department of Veterans Affairs by way of salary support.
Author Contributions
The number of authors reflects our institution’s multidisciplinary approach to infected pancreatic necrosis and includes efforts across 3 departments: The Division of Surgical Oncology, Division of Gastroenterology, and Department of Surgery.
1. Conception and Design: SD, AZ, KL, HZ, YD, MH
2. Data acquisition, analysis, interpretation: VT, CU, SD, MZ, AH
3. Drafting and revising: VT, CU, MZ, SD, AH, AZ, KL, HZ, YD, MH
4. Final approval: VT, CU, MZ, SD, AH, AZ, KL, HZ, YD, MH
Conflict of Interest
The authors have no conflicts of interests to declare.
References
- Thompson CC, Kumar N, Slattery J, Clancy TE, Ryan MB, Ryou M, et al. A standardized method for endoscopic necrosectomy improves complication and mortality rates. Pancreatology 2016; 16:66-72. [PMID: 26748428]
- van Grinsven J, van Brunschot S, Bakker OJ, Bollen TL, Boermeester MA, Bruno MJ, et al. Diagnostic strategy and timing of intervention in infected necrotizing pancreatitis: an international expert survey and case vignette study. HPB (Oxford) 2016; 18:49-56. [PMID: 26776851]
- Banks PA, Freeman ML, Practice Parameters Committee of the American College of G. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379-400. [PMID: 17032204]
- Easler JJ, Zureikat A, Papachristou GI. An update on minimally invasive therapies for pancreatic necrosis. Expert Rev Gastroenterol Hepatol 2012; 6:745-53. [PMID: 23237259]
- Freeman ML, Werner J, van Santvoort HC, Baron TH, Besselink MG, Windsor JA, et al. Interventions for necrotizing pancreatitis: summary of a multidisciplinary consensus conference. Pancreas 2012; 41:1176-94. [PMID: 23086243]
- Trikudanathan G, Arain M, Attam R, Freeman ML. Interventions for necrotizing pancreatitis: an overview of current approaches. Expert Rev Gastroenterol Hepatol 2013; 7:463-75. [PMID: 23899285]
- Umapathy C, Raina A, Saligram S, Tang G, Papachristou GI, Rabinovitz M, et al. Natural History After Acute Necrotizing Pancreatitis: a Large US Tertiary Care Experience. J Gastrointest Surg 2016; 20:1844-53. [PMID: 27619808]
- Freeny PC, Hauptmann E, Althaus SJ, Traverso LW, Sinanan M. Percutaneous CT-guided catheter drainage of infected acute necrotizing pancreatitis: techniques and results. AJR Am J Roentgenol 1998; 170:969-75. [PMID: 9530046]
- Gmeinwieser J, Holstege A, Zirngibl H, Palitzsch KD, Hugl S, Strotzer M, et al. Successful percutaneous treatment of infected necrosis of the body of the pancreas associated with segmental disruption of the main pancreatic duct. Gastrointest Endosc 2000; 52:413-5. [PMID: 10968863]
- Baron TH, Thaggard WG, Morgan DE, Stanley RJ. Endoscopic therapy for organized pancreatic necrosis. Gastroenterology 1996; 111:755-64. [PMID: 8780582]
- Gagner M. Laparoscopic Treatment of Acute Necrotizing Pancreatitis. Semin Laparosc Surg 1996; 3:21-8. [PMID: 10401099]
- Carter CR, McKay CJ, Imrie CW. Percutaneous necrosectomy and sinus tract endoscopy in the management of infected pancreatic necrosis: an initial experience. Ann Surg 2000; 232:175-80. [PMID: 10903593]
- Connor S, Ghaneh P, Raraty M, Sutton R, Rosso E, Garvey CJ, et al. Minimally invasive retroperitoneal pancreatic necrosectomy. Dig Surg 2003; 20:270-7. [PMID: 12748429]
- Horvath KD, Kao LS, Ali A, Wherry KL, Pellegrini CA, Sinanan MN. Laparoscopic assisted percutaneous drainage of infected pancreatic necrosis. Surg Endosc 2001; 15:677-82. [PMID: 11591967]
- van Santvoort HC, Besselink MG, Horvath KD, Sinanan MN, Bollen TL, van Ramshorst B, et al. Videoscopic assisted retroperitoneal debridement in infected necrotizing pancreatitis. HPB (Oxford) 2007; 9:156-9. [PMID: 18333133]
- Fagenholz PJ, Thabet A, Mueller PR, Forcione DG. Combined endoscopic trangastric drainage and video assisted retroperitoneal pancreatic debridement - The best of both worlds for extensive pancreatic necrosis with enteric fistulae. Pancreatology 2016; 16:788-90. [PMID: 27344627]
- Sorrentino L, Chiara O, Mutignani M, Sammartano F, Brioschi P, Cimbanassi S. Combined totally mini-invasive approach in necrotizing pancreatitis: a case report and systematic literature review. World J Emerg Surg 2017; 12:16. [PMID: 28331537]
- van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Boermeester MA, Dejong CH, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis. N Engl J Med 2010; 362:1491-502. [PMID: 20410514]
- Waddell C. So much research evidence, so little dissemination and uptake: mixing the useful with the pleasing. Evid Based Ment Health 2001; 4:3-5. [PMID: 11467070]
- Morris ZS, Wooding S, Grant J. The answer is 17 years, what is the question: understanding time lags in translational research. J R Soc Med 2011; 104:510-20. [PMID: 22179294]
- Brownson RC, Kreuter MW, Arrington BA, True WR. Translating scientific discoveries into public health action: how can schools of public health move us forward? Public Health Rep 2006; 121:97-103. [PMID: 16416704]
- Grimshaw JM, Eccles MP, Lavis JN, Hill SJ, Squires JE. Knowledge translation of research findings. Implement Sci 2012; 7:50. [PMID: 22651257]
- Antman EM, Lau J, Kupelnick B, Mosteller F, Chalmers TC. A comparison of results of meta-analyses of randomized control trials and recommendations of clinical experts. Treatments for myocardial infarction. JAMA 1992; 268:240-8. [PMID: 1535110]
- Haynes B, Haines A. Barriers and bridges to evidence based clinical practice. BMJ 1998; 317:273-6. [PMID: 9677226]
- Kokosis G, Perez A, Pappas TN. Surgical management of necrotizing pancreatitis: an overview. World J Gastroenterol 2014; 20:16106-12. [PMID: 25473162]
- Hackert T, Buchler MW. Decision Making in Necrotizing Pancreatitis. Dig Dis 2016; 34:517-24. [PMID: 27332898]
- Chang YC. Is necrosectomy obsolete for infected necrotizing pancreatitis? Is a paradigm shift needed? World J Gastroenterol 2014; 20:16925-34. [PMID: 25493005]
- Sugimoto M, Sonntag DP, Flint GS, Boyce CJ, Kirkham JC, Harris TJ, et al. Better Outcomes if Percutaneous Drainage Is Used Early and Proactively in the Course of Necrotizing Pancreatitis. J Vasc Interv Radiol 2016; 27:418-25. [PMID: 26806694]
- Haynes RB. Loose connections between peer-reviewed clinical journals and clinical practice. Ann Intern Med 1990; 113:724-8. [PMID: 2221658]

