Prognostic Factors in Patients with Pancreatic Adenocarcinoma and the Impact of Pancreatic Fistula on Oncologic Outcomes
Keywords
Pancreatic Cancer; Prognosis; Pancreatic Fistula
Abbreviations
OS overall survival; DFS disease-free survival; mGPS
modified glasgow prognostic score; NLR neutrophil/lymphocyte
ratio; PLR platelet/lymphocyte ratio; LMR lymphocyte/monocyte
ratio; LNR lymph node ratio; AJCC American joint committee on
cancer; ASA American society of anesthesiologists; PPPD pyloruspreserving
pancreaticoduodenectomy; CA carbohydrate antigen; CEA
carcinoembryonic antigen
INTRODUCTION
Pancreatic cancer constitutes a small percentage of all
cancers, but it is the fourth leading cause of cancer-related
deaths with a five year relative survival of 8% [1,2]. With
increasing incidence and mortality rates in recent years,
pancreatic cancer is expected to be the second leading cause
of cancer related deaths by 2030 [3]. The vast majority
of pancreatic cancers are adenocarcinomas arising from
exocrine glands of the pancreas [4]. Surgery remains the
only therapy with curative intent. The silent nature of
pancreatic cancer hinders its early-stage diagnosis despite
technological advances and modern equipment. Only 20%
of patients present with potentially resectable disease [5].
Even after curative resection and adjuvant chemoradiotherapy,
most patients will have recurrence, and the
five-year survival remains at 25% [1]. Since pancreatic
cancer cells metastasize early in disease development, 85%
of patients eventually experience recurrence after curative
resection [6]. Therefore, investigating clinicopathological
factors as prognostic indicators are essential to help
clinicians develop appropriate treatment strategies
tailored for each patient.
The tumor marker Carbohydrate Antigen (CA) 19-9
has become the “gold standard” for diagnosing and
monitoring treatment in pancreatic cancer patients over
the past several decades. However, it remains insufficient
for screening patients with pancreatic cancer [7]. Α recent
study revealed that CA 19-9 combined with another tumor
marker Carcinoembryonic Antigen (CEA), could be used
as prognostic predictors in these patients [8]. The lymph
node ratio and the total number of positive lymph nodes
were also evaluated as potential prognostic factors [9].
Furthermore, the importance of inflammation-based
scores has been recently emphasized in various cancers as
well as in pancreatic cancer [10-14].
Pancreatic fistula is the most common complication
after pancreatic surgery, which can lead to serious
adverse effects on patient outcomes. The incidence rates of pancreatic fistula after pancreaticoduodenectomy and
distal pancreatectomy range from 0% to 24% and from
5% to 28%, respectively [15]. However, there are only a
few reports on the association between pancreatic fistula
and long-term survival and local recurrence.
The aim of this study was to evaluate potential
prognostic factors and to examine the relationship
between pancreatic fistula and both overall survival and
local recurrence in 226 patients with resectable pancreatic
cancer, who were treated in the Agios Dimitrios General
Hospital department during an 11-year interval.
METHODS
Study Population
Between 2004 and 2015, 226 (65.7%) patients
with resectable pancreatic adenocarcinoma underwent
macroscopic complete resection in the “Agios Dimitrios”
General Hospital department of surgery. Resectable
pancreatic cancers were defined as stage I or II disease
according to the sixth American Joint Committee on
Cancer (AJCC) [16]. Curative surgical procedures included
pancreaticoduodenectomy (including subtotal stomachpreserving
pancreaticoduodenectomy and Pylorus-
Preserving Pancreaticoduodenectomy, PPPD), distal
pancreatectomy and total pancreatectomy.
Data Collection
After surgery, follow-up information was updated by
hospital visits, written correspondence, and telephone
interviews. The patients were followed periodically until
death, loss of contact, or the end of the study, which was
May 2018. OS time, was defined as the time period from
the date of surgery to the date of last follow-up or death.
Recurrence status and site, including local recurrence,
liver metastases, para-aortic lymph nodes metastases,
lung metastases, and peritoneal carcinomatosis, were
examined to analyze the DFS. For each patient, the following
information was collected: demographic data including
age, sex, lifestyle factors including smoking, and alcohol
consumption, presence of diabetes mellitus, abdominal
pain, comorbidity index according to the American Society
of Anesthesiologists (ASA) risk classification system, tumor
staging based on the Union Internationale Contre le Cancer
classification, tumor characteristics, including location,
histological type, and differentiation, resection margin
status, and infiltration of the lymph nodes, perineural,
and vascular structures, postoperative complications,
pancreatic fistula development and early postoperative
mortality.
We also evaluated the number of the positive lymph
nodes and the LNR by dividing the number of the positive
lymph nodes with the number of all lymph nodes that were
examined, to evaluate their prognostic value in OS and
DFS. Additionally, to investigate the roles of inflammation
scores in pancreatic cancer prognosis, we evaluated
the Modified Glasgow Prognostic Score (mGPS) which
incorporates the C-reactive protein and albumin values, the Neutrophil/Lymphocyte Ratio(NLR), the Platelet/
Lymphocyte Ratio(PLR), and the Lymphocyte/Monocyte
Ratio(LMR) for each patient.
Statistical Analysis
Clinical characteristics were analyzed using Pearson’s
chi-square or Fisher’s exact test for categorical and
dichotomous variables, and Student’s t test for continuous
variables. OS was calculated from the date of initial surgical
treatment to the date of occurrence of either death from
any cause or last contact. DFS was defined as the period
from initial surgical treatment to disease recurrence.
The Kaplan–Meier method was used to create survival
curves, and differences were assessed with the log-rank
test. Statistical significance was assumed for a two-tailed
p-value of<0.05. To determine independent factors for OS
and DFS, the Cox proportional hazards model it was used
to determine potential factors, which were entered into a
forward regression procedure for the final identification of
independent prognostic factors.
RESULTS
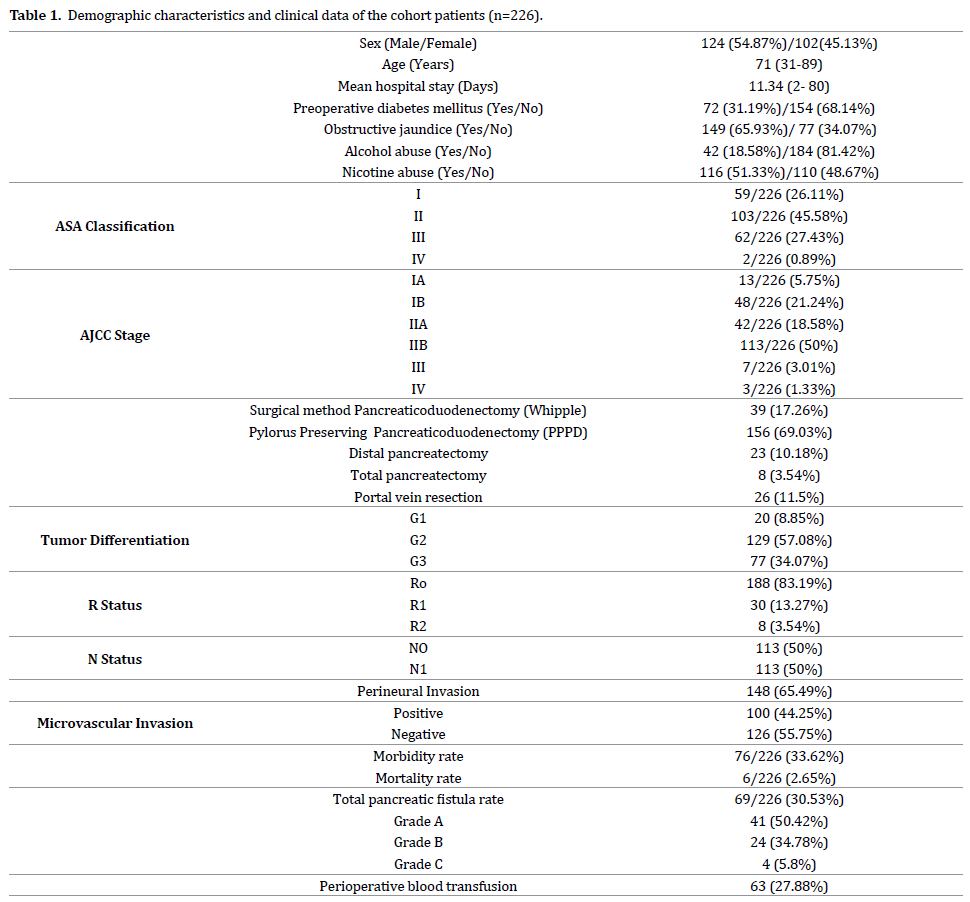
Study Patients’ Characteristics
We included 226 patients with resectable pancreatic
adenocarcinoma in this retrospective study. The median age
was 71 (31-89) years, and the male/female ratio was 1.2:1.
The presenting symptoms were jaundice and abdominal
pain in 65.93% and 47.35% patients, respectively. In the
study cohort, 116 (51.33%) patients were smokers, and
41 (18.14%) patients consumed alcohol. Diabetes mellitus
was diagnosed preoperatively in 72 (31.19%) patients,
and 44 (19.47%) patients were prescribed metformin as
diabetes mellitus therapy. Detailed information on major
demographic and clinic-pathological characteristics of the
study cohort is presented in (Table 1).
Intra-operative Parameters
In all study cohort patients, the indication for
surgery was suspicion of malignancy. Specifically, 226
patients who were found to have a resectable tumor
at exploratory laparotomy underwent subsequent
curative pancreatectomy. Among these, 156 (69.03%),
39 (17.26%), 23 (10.18%), and 8 (3.54%) patients
underwent PPPD, classic Whipple, distal pancreatectomy,
and total pancreatectomy, respectively. Partial resection
of the portal vein was necessary in 26 (11.5%) of patients
(Table 1).
Morbidity and Mortality Rates
The perioperative mortality in the first 30 postoperative
days was 2.65% (6/266) for the entire cohort. The mean
length of hospital stay for the entire cohort was 11.34
(2- 80) days. During the post-operative course, 33.62%
(76/226) of the patients in the study cohort developed one
or more complications. Additionally, 69 (30.53%) patients
developed pancreatic fistula after pancreatectomy.
Specifically, pancreatic fistulas developed in 27.18%
(53/195) and 69.57% (16/23) of the patients after pancreaticoduodenectomy and distal pancreatectomy,
respectively. Finally, 63 (27.88%) patients received blood
transfusions (Table 1).
Pathological Features
Most of the patients with resectable tumors had
AJCC stage IIb (50%) and stage Ib (21.24%) disease. The
pathologic evaluation of the surgical specimens revealed
R0, R1, and R2 resection in 188 (83.19%), 30 (13.27%),
and 8 (3.54%) patients, respectively. The pancreatic
adenocarcinoma was well-differentiated, moderateddifferentiated
and poorly differentiated in 20 (8.85%),
129 (57.08%), and 77 (34.07%) patients, respectively.
The median number of the excised lymph nodes was
14.38 (5-32), and the lymph nodes were positive in half
the patients. Perineural invasion was identified in 148
(65.49%) patients, whereas vascular invasion was found
in 100 (44.25%) patients (Table 1).
Survival and Prognostic Factors Analysis
The median OS of the entire cohort was 23.129 months,
with 1, 3 and 5-year OS rates of 35.84%, 15.48%, and
6.19%, respectively (Figure 1).
Figure 1: Plasma Na concentration (mmol/L).
We analyzed all variables to determine prognostic
factors associated with survival using the Kaplan–Meier
method with the log-rank test. Among these parameters,
PLR>160 (p=0.097, p>0.05 ), LMR<3 (p= 0.173, p>0.05),
CA 19-9>100 U/ml (p=0.274, p>0.05), CEA>10 mg/dl
(p=0.823, p>0.05), R resection status (p=0.203, p>0.05
), pancreatic fistula (p=0.818, p>0.05), blood transfusion
(p=0.666, p>0.05) had no statistically significant
association with OS. In contrast, age>65 years (p=0.004,
p<0.05), poorly differentiated tumor type (p<0.001,
p<0.05), tumor staging (p<0.001, p<0.05 ), perineural
invasion (p<0.001, p<0.05), microvascular invasion
(p<0.001, p<0.05), NLR>5 (p=0.019, p<0.05), mGPS score of 0(p=0.02, p<0.05), LNR>0,3 (p=0.033, p<0.05) were
associated with better OS (Table 2).
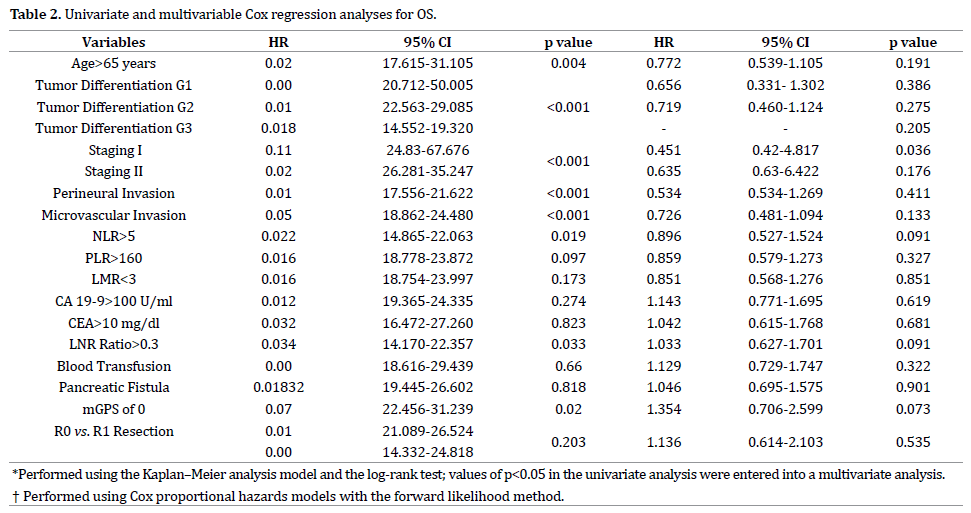
Multivariate Survival Analysis
Factors that were significantly associated with OS
in univariate survival were entered into a multivariate
analysis using the Cox proportional hazards model with
forward regression. Accordingly, the following variables
were identified as independent factors for prognosis:
age>65 years, tumor staging, microvascular invasion,
NLR>5 (p=0.091, p<0.2), mGPS of 0 (p=0.073, p<0.2), and
LNR>0,3 (p=0.091, p<0.2) (Table 2).
Analysis of the DFS Rates
The median DFS was 25.73 (2.45-145) months, and
1,3 and 5-year DFS rates were 64.6%, 14.16% and 4.87%
respectively (Figure 2). The most frequent relapse type was
local recurrence (65.04%), followed by liver metastases
(41.59%) and peritoneal carcinomatosis (22.57%).
Additionally, 63.77% of the patients with pancreatic fistula after pancreatectomy had local recurrence, whereas local
recurrence occurred in 65.6% of the patients without
fistula (p=0.670).
Figure 2: Plasma Na concentration (mmol/L).
In the univariate analyses, poorly differentiated tumor
type (p<0.001, p<0.05), tumor staging (p<0.001, p<0.05),
perineural invasion (p<0.001, p<0.05 ), microvascular
invasion (p=0.001, p<0.05), NLR>5 (p=0.017, p<0.05),
PLR>160 (p=0.03, p<0.05), CA 19-9>100 U/ml (p=0.037,
p<0.05) were significantly associated with the DFS. In
contrast, LMR (p=0.110), CEA>10 mg/dl (p=0.639),
R-resection status (0.097), pancreatic fistula (p=0.634),
mGPS of 0 (p=0.084), LNR>0.3 (p=0.052), blood
transfusion (p=0.744) were not significantly associated
with DFS.
The multivariate analysis revealed that only
microvascular invasion, NLR>5, and PLR>160 were
independent prognostic factors for DFS (Table 3).

DISCUSSION
Pancreatic cancer is one of the most lethal malignancies.
Surgery remains the only curative treatment option, and
there are no long term survivors among patients with unresectable
tumors [17]. The five-year survival rate after
curative resection varies form 15-25% based on the most
recent series [18-20]. However, despite curative resection
the actual survival rates remain disappointing, ranging
from 4.3% to 10.1%, as reported by two large populationbased
studies [21,22]. In the current study elucidated
outcomes and prognostic factors in 226 patients with
pathologically verified pancreatic adenocarcinoma who
were treated between 2004 and 2015. In the current series,
only 14/226 (6.19 %) patients survived for more than five
years, and the median survival was 23.129 months.
Our study revealed that age, tumor stage, and tumor
differentiation were negatively associated with prognosis,
consistent with the previous studies findings [23,24].
Furthermore, perineural and microvascular invasion were
associated with worse OS and DFS, and microvascular
invasion was an independent prognostic factor for OS and
DFS by the multivariate analysis, while perineural invasion
was identified in 65.49% of patients and microvascular
invasion in 44.25% of patients. In accordance with previous
studies, we found that although microvascular invasion is
less frequent than perineural invasion, it has a more severe
effect on survival. The reason could be that microvascular
invasion is responsible of metastatic recurrence of disease
and could lead to earlier metastasis, whereas perineural
invasion is responsible of local recurrence which is not
directly related to patient death [25,26].
Although postoperative mortality in pancreatic cancer
has declined significantly over the last decade, with
current rates less than 5% in certain specialized pancreatic
centers, the morbidity remains high, ranging from 25%
to 50% [23,24]. However, the impact of pancreatic
fistula on survival is controversial. In a retrospective
analysis of 184 patients, Nagai et al., found that the rate
of peritoneal recurrence was significantly increased in
patients with pancreatic fistulas. However, this increase
in the risk of peritoneal recurrence did not translate into
worse survival [27]. Assifi et al. conducted a retrospective
analysis of 221 patients with pancreatic cancer after
pancreaticoduodenectomy and found that pancreatic
fistulas did not affect local recurrence rates [28]. In
the current study, pancreatic fistulas developed in 69
(30.53%), 53 (27.18%), and 16 (69.57) of the patients who
underwent pancreatectomy, pancreaticoduodenectomy,
and distal pancreatectomy, respectively. We found no
statistically significant impact of pancreatic fistulas on local
recurrence (p=0.67) and the univariate and multivariate
analyses did not detect an effect of pancreatic fistulas on
OS or DFS.
“As the gold standard” tumor marker for monitoring
and diagnosing pancreatic cancer patients, CA19-9,
provides valuable information to assist in the therapeutic
decision-making especially for surgeons. Numerous studies
demonstrated that elevated CA 19-9 was associated with
poor prognosis [29,30]. Our study established that DFS
was lower in patients with CA 19-9 level above 100 U/ml.
Conversely, CEA, better known for its utility in colorectal
cancer, has been evaluated for pancreatic cancer as well. While the results suggest that CEA’s susceptibility was
unacceptably low in pancreatic cancer, recent studies
demonstrated CEA as an independent prognostic factor
for pancreatic cancer [31,32]. However, we could not
demonstrate a strong association between CEA and OS or
DFS.
Improvements in pathological evaluation methods for
pancreatic cancer have increased the R1 resection rate
from 20% to 80% [33]. The influence of resection status
on survival is controversial. In the present study, R1
resection was established in 13.27% of the patients after
pathological examination. The median OS (23.8 m vs. 19.5
m) and the DFS (29.3 m vs. 21.8 m) were better in patients
who underwent R0 resection compared with those
who underwent R1 resection. However, our univariate
and multivariate analyses failed to show an association
between the resection status and OS or DFS.
Lymph node involvement remains the most important
prognostic factor of survival in pancreatic cancer. LNR
provides information on the number of positive lymph
nodes as well as the total number of resected lymph nodes.
LNR’s prognostic value in pancreatic cancer has been
established by numerous recent studies [34-36]. However,
there is no consensus on the best cutoff value for LNR. We
used as a cut-off LNR of 0.3 in the current study and found
that an LNR>0.3 was an independent negative prognostic
factor on OS.
An interaction between pancreatic cancer cells and host
immune system, leading to a reduction in the lymphocyte
ratio, was recently documented [37]; therefore, we also
explored the potential associations of the inflammation
markers NLR, PLR, and LMR with OS and DFS in the
current study. NLR as a marker of active, cancer-associated
inflammation was demonstrated to be an important
prognostic factor in several cancers, such as colorectal,
gastric, and hepatocellular cancer [38-40]. A recent
retrospective study showed that an elevated preoperative
NLR was an important prognostic factor for early TNMstage
pancreatic cancer. In the current study, we evaluated
NLR with a cut-off value of five, based on previous reports
and found that NLR>5 was an independent prognostic
factor for OS as well as DFS, by univariate and multivariate
analyses. PLR as an inflammation marker was recently
shown to be a predictor of worse mid-term outcomes in
patients with borderline resectable pancreatic cancer
[41]. Yu et al. conducted a retrospective analysis and
found that a PLR>150 was an independent predictive
risk factor for postoperative long-term prognosis in
pancreatic cancer [42]. In the current study, PLR>160 was
associated with poor postoperative DFS after curative
resection in pancreatic cancer patients. Finally, LMR’s
prognostic impact on pancreatic cancer outcomes remains
unclear. A recent meta-analysis of 1,795 patients showed
that an elevated LMR predicts favorable survival [43].
Unfortunately, the current study failed to demonstrate a
similar effect of LMR on OS or DFS.
In addition to reflecting an upregulation of
inflammatory response, mGPS, which combines CRP with
hypoalbuminemia, also reflects the nutritional decline
of pancreatic cancer patients [42]. Few studies, thus
far, analyze the relationship of mGPS with survival in
pancreatic cancer. Most reports implicate mGPS as a strong
prognostic factor of recurrence and survival [44-48]. Our
results indicating mGPS is an independent prognostic
factor of OS are consistent with these findings.
CONCLUSION
Despite recent systemic treatment advances, the
prognosis of patients with advanced PDAC remain poor.
Surgery continues to be the only curative therapy and is
associated with statistically better survival rates after
curative resection. Currently, few predictive factors can
identify patients who will benefit the most from available
treatment options. We identified microvascular invasion,
NLR, mGPS, and LNR as independent prognostic OS
factors and microvascular invasion, NLR, and mGPS as
independent prognostic factors of DFS. Furthermore our
analysis showed that elevated CA 19-9 was a negative
prognostic factor for DFS, whereas R1 resection and
pancreatic fistula did not have a significant impact on
survival or recurrence.
Acknowledgements
The authors thank Dr. Chatzis Josef and all the members
of the Agios Dimitrios General Hospital, for their assistance
in data collection.
Conflicts of Interest
The authors report no conflict of interest.
References
- Rebecca L, Siegel, Kimberly D. Miller, Ahmedin Jemal. Cancer Statistics, 2018. CA Cancer J Clin 2018; 68:7–30.
- Rawla P, Sunkara T, Gaduputi V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J Oncol 2019; 10:10-27. [PMID: 30834048]
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014; 74:2913-2921. [PMID: 24840647]
- https://seer.cancer.gov/archive/csr/1975_2014/
- Shrikhande SV, Arya S, Barreto SG, Ingle S, D'Souza MA, Hawaldar R, et al. Borderline resectable pancreatic tumors: is there a need for further refinement of this stage? Hepatobiliary Pancreat Dis Int 2011; 10:319-324. [PMID: 21669578]
- O’Reilly E. Refinement of adjuvant therapy for pancreatic cancer. JAMA 2010; 304:1124–1125. [PMID: 20823441]
- Rückert F, Pilarsky C, Grützmann R. Serum Tumor Markers in Pancreatic Cancer—Recent discoveries. Cancers (Basel) 2010; 2:1107-1124. [PMID: 24281109]
- Zhou G, Liu X, Wang X, Jin D, Chen Y, Li G, et al. Combination of preoperative CEA and CA19-9 improves prediction outcomes in patients with resectable pancreatic adenocarcinoma: results from a large follow-up cohort. Onco Targets Ther 2017; 10:1199-1206. [PMID: 28280354]
- Marmor S, Burke EE, Portschy PR, Virnig BA, Jensen EH, Tuttle TM. Lymph node evaluation for treatment of adenocarcinoma of the pancreas. Surg Oncol 2015; 24:284-291. [PMID: 26303825]
- Abe T, Amano H, Kobayashi T, Hanada K, Nakahara M, Ohdan H, et al. Preoperative neutrophil-to-lymphocyte ratio as a prognosticator in early stage pancreatic ductal adenocarcinoma. Eur J Surg Oncol 2018; 44:1573-1579. [PMID: 29807728]
- Li W, Tao L, Lu M, Xiu D. Prognostic role of platelet to lymphocyte ratio in pancreatic cancers: A meta-analysis including 3028 patients. Medicine (Baltimore) 2018; 97:e9616. [PMID: 29465553]
- Stevens L, Pathak S, Nunes QM, Pandanaboyana S, Macutkiewicz C, Smart N,et al. Prognostic significance of pre-operative C-reactive protein and theneutrophil-lymphocyte ratio in resectable pancreatic cancer: a systematicreview. HPB (Oxford) 2015; 17:285e91. [PMID: 25431369]
- Stotz M, Gerger A, Eisner F, Szkandera J, Loibner H, Ress AL, et al. Increased neutrophil-lymphocyte ratio is a poor prognostic factor in patients with primary operable and inoperable pancreatic cancer. Br J Cancer 2013; 109:416e21. [PMID: 23799847]
- Inoue D, Ozaka M, Matsuyama M, Yamada I, Takano K, Saiura A, et al. Prognostic value of neutrophil-lymphocyte ratio and level of C-reactive protein in a large cohort of pancreatic cancer patients: a retrospective study in a single institute in Japan. Jpn J Clin Oncol 2015 45:61e6. [PMID: 25341546]
- Andrén-Sandberg A, Neoptolemos JP. Resection for pancreatic cancer in the new millennium. Pancreatology 2002; 2:431–439. [PMID: 12378110]
- Bilimoria KY, Bentrem DJ, Ko CY, Ritchey J, Stewart AK, Winchester DP, et al. Validation of the6th edition AJCC Pancreatic Cancer Staging System: report from the National Cancer Database. Cancer 2007; 110:738-74427. [PMID: 17580363]
- Oh SY, Edwards A, Mandelson MT, Lin 1, Dorer R, Helton WS, et al. Rare long-term survivors of pancreatic adenocarcinoma without curative resection. World J Gastroenterol 2015; 21:13574-13581. [PMID: 26730170]
- Lin R, Han CQ, Wang WJ, Liu J, Qian W, Ding Z, et al. Analysis on survival and prognostic factors in patients with resectable pancreatic adenocarcinoma. J Huazhong Univ Sci Technolog Med Sci 2017; 37:612-620. [PMID: 28786050]
- Yamamoto T, Yagi S, Kinoshita H, Sakamoto Y, Okada K, Uryuhara K, et al. Long-term survival after resection of pancreatic cancer: a single-center retrospective analysis. World J Gastroenterol 2015; 21:262-268. [PMID: 25574100]
- Benassai G, Quarto G, Perrotta S, Furino E, Benassai GL, Amato B, et al. Long-term survival after curative resection for pancreatic ductal adenocarcinoma-Surgical treatment. Int J Surg 2015; 21:S1-S3.
- Carpelan-Holmstrom M, Nordling S, Pukkala E, Sankila R, Luttges J, Kloppel G, et al. Does anyone survive pancreatic ductal adenocarcinoma? A nationwide study re-evaluating the data of the Finnish Cancer Registry. Gut 2005; 54:385–387. [PMID: 15710987]
- Zijlstra M, Bernards N, de Hingh IH, van de Wouw AJ, Goey SH, Jacobs EM, et al. Does long-term survival exist in pancreatic adenocarcinoma? Acta Oncol 2016; 55:259-264. [PMID: 26559995]
- Vernerey D, Huguet F, Vienot A, Goldstein D, Paget-Bailly S, Van Laethem JL, et al. Prognostic nomogram and score to predict overall survival in locally advanced untreated pancreatic cancer. Br J Cancer 2016; 115:281-289. [PMID: 27404456]
- Wang XD, Qian JJ, Bai DS, Li ZN, Jiang GQ, Yao J. Marital status independently predicts pancreatic cancer survival in patients treated with surgical resection: an analysis of the SEER database. Oncotarget 2016; 7:24880–24887. [PMID: 27036036]
- Garcea G, Dennison AR, Pattenden CJ, Neal CP, Sutton CD, Berry DP. Survival following curative resection for pancreatic ductal adenocarcinoma. A systematic review of the literature. JOP 2008; 9:99-132. [PMID: 18326920]
- Dusch, Weiss C, Ströbel P, Kienle P, Post S, Niedergethmann M. Factors predicting long-term survival following pancreatic resection for ductal adenocarcinoma of the pancreas: 40 years of experience. J Gastrointest Surg 2014; 18:674-81. [PMID: 24241965]
- Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006; 244:10–15. [PMID: 16794383]
- Seetharam P, Rodrigues GS. Postoperative Pancreatic Fistula: A Surgeon's Nightmare! An Insight with a Detailed Literature Review. JOP 2015; 16:115-124 [PMID:25791544]
- Nagai S, Fujii T, Kodera Y, et al. Recurrence pattern and prognosis of pancreatic cancer after pancreatic fistula. Ann Surg Oncol 2011; 18:2329-2337. [PMID: 21327822]
- Assifi MM, Zhang S, Leiby BE, Pequignot EC, Xia B, Rosato E, et al. Tumor recurrence is independent of pancreatic fistula in patients after pancreaticoduodenectomy for pancreatic ductal adenocarcinoma. J Am Coll Surg 2013; 217:621-627. [PMID: 23810574]
- O'Brien DP, Sandanayake NS, Jenkinson C, Gentry-Maharaj A, Apostolidou S, Fourkala EO, et al. Serum CA19-9 is significantly upregulated up to 2 years before diagnosis with pancreatic cancer: implications for early disease detection. Clin Cancer Res 2015; 21:622-631. [PMID: 24938522]
- Zhang S, Huang X, Tian Y, Aimaiti S, Zhang J, Zhao J, et al. Clinicopathologic characteristics, laboratory parameters, treatment protocols, and outcomes of pancreatic cancer: a retrospective cohort study of 1433 patients in China. Peer J 2018; 6:e4893. [PMID: 29868287]
- Rückert F, Pilarsky C, Grützmann R. Serum tumor markers in pancreatic cancer-recent discoveries. Cancers (Basel) 2010; 2:1107-1124. [PMID: 24281109]
- Lee KJ, Yi SW, Chung MJ, Park SW, Song SY, Chung JB, et al. Serum CA 19-9 and CEA levels as a prognostic factor in pancreatic adenocarcinoma. Yonsei Med J 2013; 54:643-649. [PMID: 23549809]
- Butturini G, Stocken DD, Wente MN, Jeekel H, Klinkenbijl JH, Bakkevold KE, et al. Influence of resection margins and treatment on survival in patients with pancreatic cancer: meta-analysis of randomized controlled trials. Arch Surg 2008; 143:75–83. [PMID: 18209156]
- Pawlik TM, Gleisner AL, Cameron JL, Winter JM, Assumpcao L, Lillemoe KD, et al. Prognostic relevance of lymph node ratio following pancreaticoduodenectomy for pancreatic cancer. Surgery 2007; 141:610–618. [PMID: 17462460]
- Hellan M, Sun CL, Artinyan A, Mojica-Manosa P, Bhatia S, Ellenhorn JD, et al. The impact of lymph node number on survival in patients with lymph node-negative pancreatic cancer. Pancreas 2008; 37:19–24. [PMID: 18580439]
- Slidell MB, Chang DC, Cameron JL, Wolfgang C, Herman JM, Schulick RD, et al. Impact of total lymph node count and lymph node ratio on staging and survival after pancreatectomy for pancreatic adenocarcinoma: a large, population-based analysis. Ann Surg Oncol 2008; 15:165–174. [PMID: 17896141]
- Inman KS, Francis AA, Murray NR. Complex role for the immune system in initiation and progression of pancreatic cancer. World J Gastroenterol 2014; 20:11160–11181. [PMID: 25170202]
- Harimoto N, Shirabe K, Nakagawara H, Toshima T, Yamashita Y, Ikegami T, et al. Prognostic factors affecting survival at recurrence of hepatocellular carcinoma after living-donor liver transplantation: with special reference to neutrophil/lymphocyte ratio. Transplantation 2013; 96:1008-1012. [PMID: 24113512]
- Shimada H, Takiguchi N, Kainuma O, Soda H, Ikeda A, Cho A, et al. High preoperative neutrophil-lymphocyte ratio predicts poor survival in patients with gastric cancer. Gastric Cancer 2010; 13:170-176. [PMID: 20820986]
- Yu J, Ding Z, Yang Y, Liu S. Increased platelet-to-lymphocytes ratio is associated with poor long-term prognosis in patients with pancreatic cancer after surgery. Medicine (Baltimore) 2018; 97:e11002. [PMID: 29923983]
- Asari S, Matsumoto I, Toyama H, Shinzeki M, Goto T, Ishida J et al. Preoperative independent prognostic factors in patients with borderline resectable pancreatic ductal adenocarcinoma following curative resection: the neutrophil-lymphocyte and platelet-lymphocyte ratios. Surg Today 2016; 46:583–92. [PMID: 26108488]
- Li W, Tao L, Zhang L, Xiu D. Prognostic role of lymphocyte to monocyte ratio for patients with pancreatic cancer: a systematic review and meta-analysis. Onco Targets Ther 2017; 10:3391-3397. [PMID: 28744143]
- Lien YC, Hsieh CC, Wu YC, Hsu HS, Hsu WH, Wang LS, et al. Preoperative serum albumin level is a prognostic indicator for adenocarcinoma of the gastric cardia. J Gastrointest Surg 2004; 8:1041–1048. [PMID: 15585392]
- Jamieson NB, Glen P, McMillan DC, McKay CJ, Foulis AK, Carter R, et al. Systemic inflammatory response predicts outcome in patients undergoing resection for ductal adenocarcinoma head of pancreas. Br J Cancer 2005; 92:21-23. [PMID: 15597096]
- Smith RA, Dajani K, Dodd S, Whelan P, Raraty M, Sutton R, et al. Preoperative resolution of jaundice following biliary stenting predicts more favourable early survival in resected pancreatic ductal adenocarcinoma. Ann Surg Oncol 2008; 15:3138-3146. [PMID: 18787902]
- La Torre M, Nigri G, Cavallini M, Mercantini P, Ziparo V, Ramacciato G. The Glasgow prognostic score as a predictor of survival in patients with potentially resectable pancreatic adenocarcinoma. Ann Surg Oncol 2012; 19:2917-2923. [PMID: 22488099]



